
Abstract
While the relationship between offending and mental health is complex, research findings indicate that those in conflict with the law have higher levels of mental illness and need than the general population. This article considers the findings of a joint thematic inspection of the criminal justice journey for individuals with mental health needs, with a particular focus on the probation stage. Inspectors from across justice and health reviewed cases to establish the extent to which needs were identified and met. Interviews were also undertaken with 67 individuals who had lived experience of mental illness while in the criminal justice system. Findings are considered in relation to the identification of mental health needs; the role of trauma; probation practitioners’ skills, knowledge and support; case management; and access to required services. This inspection led to identified effective practice and key agencies agreeing to a number of actions in response to inspectors’ recommendations.
Introduction
The relationship between offending and mental illness is complex (Brooker et al., 2012). Due to data not being routinely gathered, it is not possible to make an accurate assessment on the number of people in conflict with the law who have mental health needs. However, evidence suggests that levels of mental illness amongst those in the criminal justice system (CJS) are higher than in the general population.
A recent study by Samele et al. (2021) which looked at a 2-week sample of people entering custody in one South London police station (n = 134) noted that 29% had a current mental illness, while 40% were believed to have had mental health needs at some point in their life. Leese and Russell (2017) had similar findings where they reported that more than a third of people entering police custody have some form of mental illness. An evaluation of the Liaison and Diversion 1 (L&D) service (Disley et al., 2021) found that 72% of the almost 37,000 people referred had mental health needs, a fifth of whom had two or more specific needs. In addition, 62% of the overall sample had previously utilised mental health services. And for those individuals in prison, research has widely indicated that levels of mental illness amongst this population are consistently higher than the general population (National Audit Office, 2017), and indeed that over 90% of those incarcerated may have at least one mental health need (NICE, 2017). In addition, the prison environment itself can be a trigger for developing or exacerbating mental illness (Schnittker et al., 2012).
Levels of mental health needs have also unsurprisingly been found to be high amongst those individuals under probation supervision. A study from 2012 (Brooker et al., 2012) found that in a random sample taken from one probation trust (n = 173), almost four in ten had a current mental illness, whereas almost half had a past/lifetime mental health condition. Similar levels of mental health need have been seen in HM Inspectorate of Probation data. Findings from 2016–2017 inspection data (n = 1066) revealed that in almost four in ten of the inspected cases, emotional well-being was a factor that the inspector judged to be a priority for supporting an individual’s desistance 2 (HM Inspectorate of Probation, 2019). Furthermore, unpublished analysis of HM Inspectorate of Probation data on more recent inspections (2018–2019) revealed that in just over a third of cases (n = 3308), mental health was recorded by inspectors as a disability.
It is equally challenging in getting a true estimate of the levels of mental illness in the general population to allow for comparison. However, to give an approximation, the Adult Psychiatric Morbidity Survey 2014 (McManus et al., 2016) estimated that approximately one in six people report symptoms of common mental health problems, around four per cent screen positive for post-traumatic stress disorder, three per cent for personality disorders, two per cent screened positive for bipolar disorder and less than one in a hundred for psychotic disorder.
The link with trauma
Although it is not possible to say with certainty why there is such a significant amount of mental health need in the CJS, it should be borne in mind that high levels of trauma and experiences of adversity have been found amongst people in conflict with the law. For example, the Welsh Adverse Childhood Experience Study (Bellis et al., 2016), which compared people with four or more of the listed incidences of childhood adversity
3
with those who had none, found that those with multiple experiences of trauma were: • fourteen times more likely to be a victim of violence in the last 12 months; • fifteen times more likely to be a perpetrator of violence in the last 12 months; and • twenty times more likely to have been incarcerated in their lives.
Furthermore, it has been found that prisoners who reported experiencing abuse or observing violence as a child were reconvicted more frequently in the year after release than those who did not (Williams et al., 2012).
It should be emphasised, however, that the association between trauma and adversity and criminality does not necessarily indicate a causal link. For while those who have experienced challenging life events have a greater likelihood of criminal justice involvement, many people with similar life experiences do not go on to be victims and/or perpetrators of crime. Protective factors in the life of an individual can provide a buffer, with having at least one stable relationship with a supportive parent, caregiver or other adults being seen as key (National Scientific Council on the Developing Child, 2015). Other potentially protective factors include low levels of poverty and deprivation; good behaviour and healthy coping mechanisms; positive attitudes and self-esteem; good education and higher levels of intelligence; and positive peers and neighbourhood connections (Scottish Government, 2018).
An ‘underserved’ population
Public Health England guidance entitled ‘Health Matters: Reducing Health inequalities in Mental Illness’ (Public Health England PHE, 2018) highlighted that those living with mental illness and in contact with the CJS can be described as an ‘underserved’ population. In addition, where services are provided, these are often not suitable or accessible. Reasons for this can include personal and structural barriers, such as stigma, low levels of help seeking behaviour, complex commissioning arrangements leading to fragmented pathways and challenging personal and social circumstances. Sirdifield and Brooker (2020) likewise emphasised several potential barriers for people on probation not accessing mental health services until they are at crisis point, including poor past experiences of accessing care and a mistrust of healthcare staff; low levels of literary and health literacy; lack of appropriate provision for complex needs; poor GP access; and the complexity of the healthcare landscape and sub-optimal commissioning processes.
As noted above, commissioning arrangements are a particular issue, described by Sirdifield et al. (2019) as being ‘complex and fragmented’. NHS England currently commission health services for prisons and L&D services, while Integrated Care Systems (ICSs) (formerly Clinical Commissioning Groups (CCGs)) are responsible for commissioning healthcare services for those individuals being managed in the community. Mental Health Trusts (MHTs) are commissioned by ICSs to provide services for people with mental ill health, with staff playing a role in Multi-Agency Public Protection Arrangements (MAPPA), supporting L&D teams, and the use of Mental Health Treatment Requirements (MHTRs) used as part of a community sentence. This complex landscape can cause a number of challenges, including gaining access to information from other agencies, disruption of care between custody and the community (and vice versa), and probation staff sometimes lacking awareness of the available care pathways and how to access them.
In addition to these organisational and awareness challenges, it seems that services are often not being commissioned specifically for those under probation supervision. In a 2017 article, NHS commissioning for probation in England was described by the authors as being delivered ‘on a wing and a prayer’ (Brooker et al., 2017), with a follow-up study (Sirdifield et al., 2019) suggesting that this was still very much the case. In this latter study, a survey to all CCGs (now ICSs) and MHTs in England revealed that just 4.5% of CCGs described commissioning a service specifically for probation service clients, and 7.6% described probation-specific elements within their mainstream service commission. More worrying still, almost a fifth of CCGs who responded incorrectly suggested that NHS England are responsible for commissioning healthcare to those on probation rather than themselves. MHT responses fared better, with almost seven in ten describing providing services specially for probation clients, and almost a further two in ten having probation-specific elements within their mainstream service provision.
A good time for inspection
In 2009, the Bradley Report (Bradley, 2009) provided a review of individuals in the CJS who were experiencing mental health needs and/or learning disabilities. Following this, Lord Bradley stated that the ‘failure to adequately address the mental health needs of offenders is a fundamental cause of chronic dysfunction in our CJS’. Key themes which resonate throughout the report include the need for early assessment and identification of mental illness; continuity of care and support for an individual throughout their time within the CJS; and joined up partnership working which includes timely information sharing. Following his review, Lord Bradley made a number of recommendations as to what was needed to reduce the number of mental health issues in prisons and impact on future reoffending.
In the same year as the Bradley Report, a joint criminal justice inspection report was published, with a focus on the services provided to individuals with mental health needs before sentencing (Criminal Justice Joint Inspection, 2009). The report found that across the vast majority of reviewed cases, concerns about the individuals mental health, even where these were not severe, were followed up and given due consideration during the pre-court and sentencing stages. However, it was noted that there was a lack of a commonly agreed definition across agencies for those with mental ill health, meaning that there were no consistent estimates of the number of people requiring supportive treatments. As such, the inspection recommended that a range of departments across health, children, justice, youth justice and the Home Office adopt a common definition. It was also found that few information exchange protocols existed between criminal justice agencies which focus explicitly on those with mental ill health.
Five years on from the Bradley Report, the Centre for Mental Health conducted an independent review of improvements made and priorities for further development (Durcan and Zwemstra, 2014). In a foreword, Lord Bradley himself noted that there had been significant progress towards achieving his recommendations. However, the report found that whilst some advances had been made in making greater use of MHTRs, further development was needed to improve sentencing, with training in mental health awareness recommended for sentencers.
Twelve years on from the original thematic inspection, the decision was made to revisit the experience of those with mental health needs in conflict with the law (Criminal Justice Joint Inspection, 2021). This was due to increasing concerns about the quality of services received by adults with mental health needs as they progress through all stages of the CJS. In 2018, Public Health England noted both structural barriers and significant gaps in access to appropriate and personalised services for people in contact with the CJS living with mental illness (Public Health England, 2018). High levels of mental health need in the CJS call for high levels of support, and for some individuals, entry into the CJS should provide them with an opportunity to receive the treatment they both require and deserve, where they have previously been missed by mental health services. Given the public interest and breadth and complexity of this topic, a joint inspection was considered to be appropriate in order to shed light on the decisions taken and the quality of services provided at each stage of the justice system.
Methods
The inspection, entitled A joint thematic inspection of the criminal justice journey for individuals with mental health needs and disorders, was led by HM Inspectorate of Probation, and supported by a team of inspectors from Her Majesty’s Crown Prosecution Service Inspectorate (HMCPSI), HM Inspectorate of Constabulary and Fire & Rescue Service (HMICFRS), Care Quality Commission (CQC), Healthcare Inspectorate Wales (HIW) and HM Inspectorate of Prisons (HMIP). Additional support was also provided by HM Courts and Tribunal Service (HMCTS).
The joint inspection looked at work carried out across the following six locations: Birmingham, Croydon, Durham, Exeter, Greater Manchester (Bolton) and Gwent, Newport, covering the corresponding CPS areas, police forces, L&D schemes, probation services and prisons. In total, from a sample of cases where the individual was sentenced to a community order or suspended sentence order or released from custody on licence during a set period, 45 cases were reviewed jointly by up to four criminal justice inspectorates as well as the appropriate healthcare inspectorate, with the following breakdown: • Fifteen licence cases (short prison sentence – under 2 years) reviewed by all inspectorates. • Fifteen licence cases (long prison sentence – over 2 years) reviewed by HMIP, HM Inspectorate of Probation and CQC/HIW only. • Fifteen community cases reviewed by HMICFRS, HMCPSI, HM Inspectorate of Probation and CQC/HIW only.
A further 15 community cases from this sample were reviewed by HM Inspectorate of Probation only.
In addition, a further 270 cases from across criminal justice caseloads were reviewed by single inspectorates, with interviews being held with approximately 550 staff working across different agencies. Penal Reform Solutions (PRS), a user engagement consultancy, also undertook interviews with 67 individuals with lived experience of mental health needs, who shared insights about their experience as a defendant or convicted person as they progressed through the CJS.
Despite the recommendation from the 2009 inspection, there still did not appear to be any commonly held definition of mental health used across the various justice agencies. As such, for the purpose of the inspection, it was decided to use the definition initially put forward by the National Association for the Care and Resettlement of Offenders (NACRO), one that was later adopted by Lord Bradley in his 2009 review:
‘Those who come into contact with the CJS because they have committed, or are suspected of committing, a criminal offence, and who may be acutely or chronically mentally ill. It may also include those in whom a degree of disturbance is recognised, even though it may not be severe enough to bring it within the criteria laid down by the Mental Health Act 1993 (now 2007)’.
Number and percentage of cases by type of mental health diagnosis/condition.
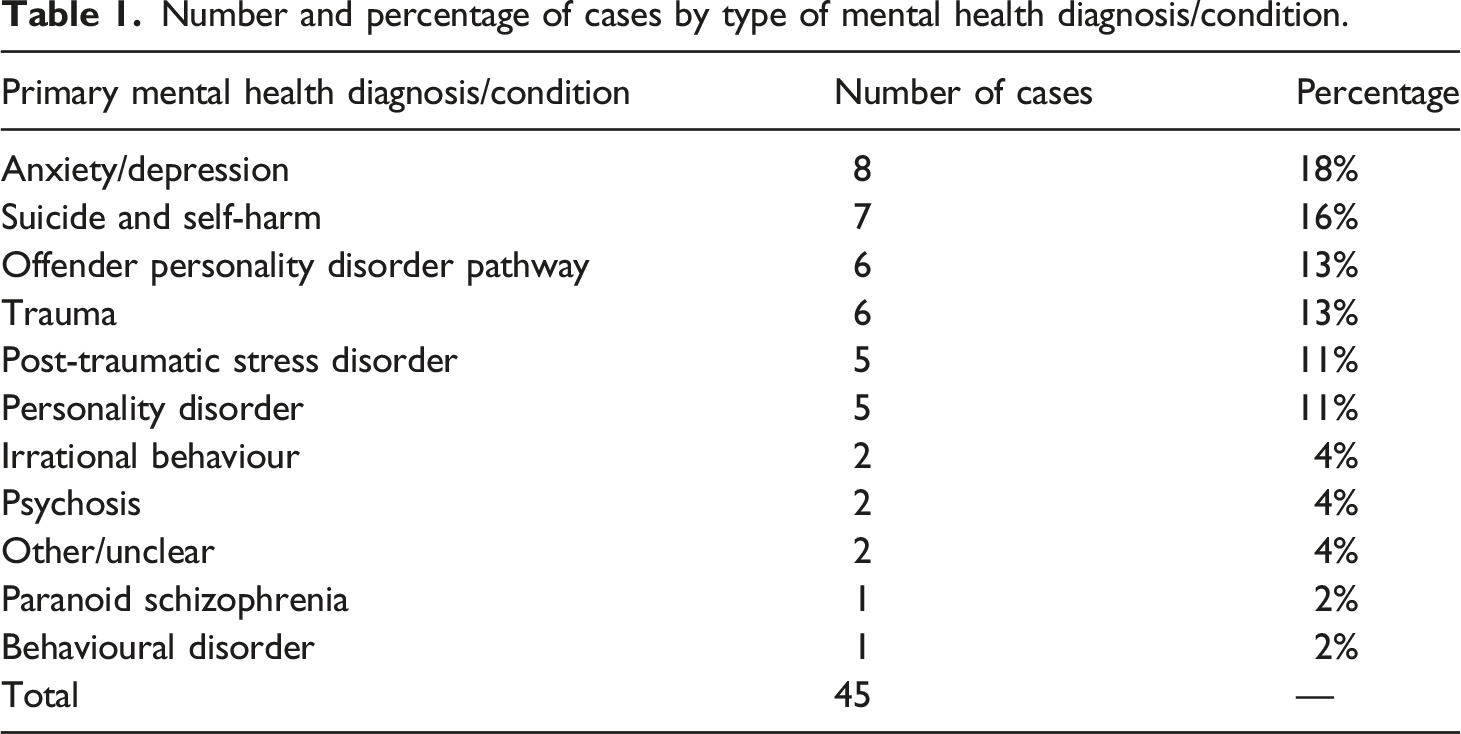
Of these 45 cases, 21 were assessed as having a co-existing issue of substance misuse, two of neurodiversity and four with both.
Findings
This section will provide a summary of the findings from the thematic inspection. It is important to note that the inspection took place shortly before the unification of the Probation Service, when the probation landscape was split between the National Probation Service (NPS) – the publicly owned service which managed MAPPA cases and other high-risk individuals – and Community Rehabilitation Companies (CRCs) – privately owned and managing all other low- and medium-risk individuals. In general, the findings were reflected across both the NPS and CRCs, but where differences were found these have been highlighted. In addition, the fieldwork took place during the COVID-19 pandemic, when many staff were working at home and service provision was reduced, paused and/or being delivered in a different way (often remotely).
Identification of mental health needs and disorders
Before an individual comes under the supervision of probation services, there will have been a number of previous opportunities for their mental health needs to be identified including in police custody, at court and in prison (where applicable). In order for those with mental health needs to receive the required care, support and treatment, it is essential that these needs are correctly and consistently identified at all relevant stages of a person’s journey through the CJS and for this information to be transferred from one agency to the next. However, inspectors noted several factors which prevented this from taking place.
Different assessment tools and criteria to determine mental health needs were found to be used across each agency. This inevitably led to varying conclusions in relation to the severity of the problem, as well as the level of need. The flagging of mental health on the various systems used by different agencies was described by inspectors as ‘muddled and inconsistent’. As such, individuals transferring from one agency to the next often did not have these concerns automatically raised.
Despite many individuals stating that they had been asked about their mental health needs at various stages of their criminal justice journey, even when these had been identified it did not necessarily mean that appropriate support was then received. One individual described assessment as ‘a box ticking exercise’, while another stated that they did not believe staff were being genuine when they asked them about any mental health needs. When this led to little or no appropriate action, this could make people less likely to disclose to staff in the future.
Interviews with those who had lived experienced of the CJS noted that they would have liked staff to have asked more questions about their mental health and encouraged them to seek help where there were any concerns. It was also found that often practitioners did not explain why the questions were being asked – that is, to ensure they got the required support – which could again lead to individuals being less likely to disclose.
It should be noted, however, that there could be legitimate reasons as to why mental health concerns identified at the probation stage were not picked up earlier. In some instances, these may have been sufficiently managed at the time, so that the individual did not require additional support. People may have also developed mental illness or trauma from their time spent in the CJS, especially after a period in custody. As such, these may not have been present at earlier stages. But it is also important to recognise that many people may feel uncomfortable in disclosing their mental illness due to fear of stigma. Where their presentation did not make their mental illness apparent, this alongside a lack of disclosure could lead to non-identification by criminal justice staff who are not trained mental health professionals.
Due to their contact with other agencies, probation staff have access to a range of relevant information to identify any mental health needs in the people under their supervision, potentially including CPS documents, court reports and historical case records, as well as relevant screening and assessment tools. Where individuals had positive relationships with immediate or extended family, these could also provide a vital source of information. However, it was found that these sources were often overlooked by probation practitioners, who instead based judgements on self-report by the individual, without viewing this within the context of other sources. Information was also not always accessed from statutory agencies working with the individuals. As such, a comprehensive analysis of mental health needs was only found in about half of inspected cases, with inspectors noting that practitioners need to be better equipped to talk to individuals about their mental health problems in order to gain an understanding of specific needs.
The role of trauma and the need for safety and certainty
At various stages of the CJS and especially as part of the lengthy assessments required during the probation stage, individuals will be asked questions which may potentially lead them to recall traumatic episodes which they have experienced in the past or may still be living through. Indeed, the theme of trauma emerged strongly through the stories told by those with lived experience of mental illness within the CJS. For some, this trauma was something they encountered so often that they had accepted this as a normalised part of their lives. While many chose to hide the full impact from others, this did not lessen the pain and raw emotion they could be feeling.
Some individuals noted that earlier stages of their criminal justice journey caused or exacerbated their trauma, including the experience of arrest and detention, appearing in court and, for some, spending time in custody. And while the experience of probation was less frequently identified as a place of trauma, the negative and triggering impact of having to discuss past trauma and ‘retell their story’ to multiple staff could be significant. This was illustrated by Cooper, who recalled ‘they are expecting a lot from me, there is no point bringing up s*** from when I was a kid…this causes mental health problems’. So, while probation offices are likely to feel safer physically than the prison environment for most, they have the potential to undermine the individual’s sense of psychological safety, which can be just as significant.
As such, trust between a practitioner and the person under their supervision is of the utmost importance in not only encouraging individuals to disclose their mental health needs but also in supporting positive change as well as avoiding re-traumatisation. However, trust can be difficult to establish when there are frequent changes in staff providing their supervision. This is something which is well known to be the case in probation practice, where individuals can experience multiple practitioners during their time with the service.
Linked to the feeling of safety is also having a good degree of certainty and clarity around the probation process, and those interviewed appreciated regular meetings with professionals who took the time to explain decisions and information about their sentence/order. This is especially important at points of transition, such as between custody and community or between youth offending and adult services, as these periods can be extremely stressful. Where individuals felt that they were being kept in the dark, this would likely enhance a sense of anxiety and concern for the future. Even where the outcome was negative, having this fully explained could go some way to lessen the impact, especially when it was felt that they were being treated fairly. However, when the process was perceived to be unjust and/or uncertain, this could have a significantly detrimental impact on an individual’s mental health. This finding links into the concept of ‘procedural justice’, which suggests that if people feel they have been treated in a procedurally fair and just way, they will be more likely to comply and engage, even when the outcomes of decisions or processes are unfavourable or inconvenient.
Probation practitioner skills, training and support
While it is important to note that probation practitioners are not and should not be expected to act as mental health professionals, they undoubtably play a key role in the identification of mental health needs. Despite a number of probation staff feeling a ‘weight of responsibility’ for those under their supervision who had complex mental health needs, significant gaps were found in staff knowledge and understanding of mental health. Many reported not having access to effective mental health learning. Where training was found to be available, this was mainly in the form of e-learning, most of which was not mandatory, and was too basic to meet staff needs for helping people on probation. This could leave staff feeling vulnerable in working with this population and left them managing cases for which they were neither fully competent nor experienced. Yet while some staff felt that this was frequently the case, they did not feel able to return these cases for reallocation due to fear of being seen as not being capable. Some of these concerns around insufficient training, skills and support may in part explain why inspectors found flagging of mental health needs and disorders to be muddled. The exception to this was those staff who had more recently joined the service from a PQiP 5 background and had undertaken an academic module which addressed mental health and offending directly.
In general, the dissemination of learning about mental health was found to be limited. While practitioners shared advice amongst each other in relation to what had worked for them with a particular individual under their supervision, there did not appear to be a strategic approach to sharing learning. In some areas, practice development events had been held to disseminate information, something which inspectors considered to be good practice. In addition, despite practice guidance around supporting those with mental health needs being produced regularly and being available on the intranet, many practitioners were unsure on how to access this, relying on other, unverified sources.
Management oversight was often found to be absent or ineffective, and while some managers had a background in mental health and felt confident in providing advice to practitioners, many revealed a limited understanding of how best to work with these individuals and thus provide support for staff supervising cases of this nature. Where discussions did take place in supervision, these tended to be general in nature rather than examining the quality of the mental health work being delivered. As such, poor work in this area could continue unchecked. Managers also seemed to lack awareness of guidance around flagging or how to access this, something which inspectors found to be ‘very concerning’ and requiring ‘urgent review’.
It is important to note, however, that the role of staff in supporting mental health is not exclusively about formal training and knowledge, but just as much about the humanity, compassion, care and understanding they show towards those under their supervision. From interviews with those with lived experience of mental health and the CJS, relationships were the strongest theme to emerged, with participants emphasising the importance of feeling that they were being treated as an individual and that their needs were being heard and understood. With consistency and time, a good degree of trust could be established, and as John stated, ‘my probation officer is my rock…her honesty and respect lifted me’. It was also apparent that when those under probation supervision felt like they had ‘someone on your side’, this could allow for a safe space to be established where individuals could be honest and open about their mental health needs. In contrast, where interactions with staff were seen as lacking in decency, they could have a detrimental impact. While most of the participants recalled incidences of being treated poorly at various stages of the CJS, on the whole, probation staff were viewed as much more understanding.
Case management – planning, implementation and delivery and review
While correctly assessing mental health is essential to ensure that needs are identified, this will only provide benefit to the individual if there is a plan for action which is then implemented and delivered, as well as being reviewed to check the proposed action is still relevant and appropriate.
With regards to planning by probation practitioners, inspectors found that this did not fully address the mental health needs of individuals in over half of reviewed cases, with notable deficits in planning where an individual had a dual diagnosis or a comorbid condition. Where plans did not set out how identified mental health needs would be specifically addressed, this resulted in any signs of deterioration not being recognised.
When planning supervision, it is also essential that people on probation themselves contribute to their assessments and plans, and that their diversity needs are understood and inform supervision. Unfortunately, inspectors found that this was not always the case, with some probation staff lacking an understanding as to how diversity needs can impact on mental health, as well as the confidence in having these conversations with those under their supervision.
Even taking into account the restrictions in place due to the COVID-19 pandemic, inspectors found that, in many cases, coordination of services – including referrals and follow-ups – was poor. Even when accessible, mental health services were not used well, with too much time being spent managing crisis. Where effective practice was found, inspectors noted that this was largely driven by the tenacity and persistence of individual practitioners. Mental health services often failed to attend MAPPA meetings, meaning that up-to-date information could not be obtained.
While this inspection found a range of systems and processes in place to support the delivery of mental health services, obstacles were seen in relation to accessing information from external providers. Concerns about the General Data Protection Regulation (GDPR) and breaching confidentiality meant that probation staff were left unable to access relevant details relating to those under their supervision from community mental health service providers, something which was even more challenging where the individuals had been receiving care from an out-of-area mental health service. This has been a constant and long-standing barrier to supporting individuals with complex needs.
Due to the dynamic nature of risk and need, probation practitioners are required to be proactive in responding when circumstances change for the individual under their supervision. Reviews should also include the active involvement of the person on probation as this can play an important role in enabling them to better understand the progress they have made, what has prevented or hindered this and what more they need to do to reach their goals.
The quality of reviews was found to be variable, and they often seemed to have been completed as an administrative exercise, with adjustments to plans following significant changes not considered in just under half of inspected cases. As with the other stages of case management, too much reliance was placed on self-report, rather than gathering information from relevant agencies where this could be obtained. Probation practitioners also failed to make contact with those people who play a significant role in the life of the individual who could verify the extent to which progress had (or had not) been made.
Access to required services
Within the community, there is a dearth of high-quality and comprehensive services to meet the spectrum of mental health needs of those on probation. While service provision was found to be good for those with a diagnosis under the Mental Health Act, this was not the case for those without this diagnosis. Probation staff were not always being clear about what mental health service providers could offer as well as the thresholds and criteria for a service to be accessed. In the main, for those with less severe but still challenging and potentially limiting mental health needs, the options available to them were to request a referral to the Improving Access to Psychological Therapies (IAPT) 6 service by their general practitioner, self-referral to a crisis team or referral to a mental health service by a probation practitioner. However, it was found that these routes did not always lead to individuals receiving the required intervention, and cases were being too readily closed when individuals failed to keep appointments.
Challenges could also arise for those transitioning from custody to the community, as thresholds for treatment of mental health are generally lower in prison. This meant many individuals were unable to get continuity of care on release and/or lengthy waiting times for treatment. This situation was exacerbated by differing commissioning arrangements for prison and probation.
Even though directories of services are generally kept by probation services, these were found to be irregularly maintained and updated. Furthermore, even where services were available, these were often not specialised enough to meet the variety of needs and protected characteristics. Little evidence was found that leaders were reaching out to source or access specialist services, and practitioners were not making use of the advice and guidance available through the Association of Mental Health Providers. 7
Those with a ‘dual diagnosis’ of mental health and substance misuse needs were generally not served well, with each agency refusing to begin treatment until the other aspect of their condition had been addressed. This could lead to people with nowhere to turn and falling between the gaps in service provision. On some occasions, substance misuse was treated in isolation, but this is unlikely to be successful without accompanying support for the thoughts and emotions which underly this condition.
There was also poor service provision in meeting the diversity needs of this population. Interviews with those from minority ethnic backgrounds who had lived experience of mental health needs while in the CJS revealed that they had a greater tendency to lack faith in the support they expected to be offered for their needs. As a result of feeling ‘let down’, they were less likely to disclose their mental illness, instead ‘going off their own back’ to seek support away from the CJS. While there appeared to be some good local provisions for women which were accessed by some of the participants, men seemed more reluctant to access the available support. Indeed, several of the male participants spoke about concerns around masculinity and the fact that they may appear ‘weak’ or ‘vulnerable’ if they disclosed that they required support for their mental health. Neurodiversity could also be a barrier to receiving appropriate support for mental health needs. This was raised by one individual who highlighted that emphasis was consistently placed more on his autism, leaving his mental health needs unmet.
The MHTR was introduced in 2005 as part of a community sentence, with the aim of supporting individuals with moderate mental health needs. However, due to historical challenges in securing the required psychological services to support the sentence amongst other factors, very few MHTR orders have been made in proportion to the level of need. Since October 2017, a number of Community Sentence Treatment Requirement sites have been established, leading to an increase in the numbers of MHTRs being made as well as an increase in combined orders which include drug and alcohol treatment. Where used appropriately, MHTRs can be an effective way of ensuring that individuals receive the tailored treatment to meet their needs.
While Offender Personality Disorder pathways were well established in the NPS, these were not always used as intended or where required. In addition, probation practitioners reported mixed views about the case consultations and case formulations they received through this service. The recent introduction of the enhanced Intensive Intervention and Risk Management Service (IIRMS) in some regions has been welcomed, as it offers casework by a psychologist.
The (lack of) prioritisation of mental health in probation services
Inspection findings revealed that while NPS senior leaders were familiar with overarching national health and well-being strategies and priorities, this knowledge and intent was not actively driving local policy. So, while there was much commitment to achieving positive mental health outcomes, there was also the acceptance that there was still much more work required. No equitable strategies were found in the CRCs which meant that mental health was more likely to be marginalised. The unification of probation services provides an opportunity for mental health to be seen as a priority and be embedded at local levels in a meaningful way.
In addition, while probation senior leaders were found to be well-represented at cross agency partnerships boards, such as those for health and well-being, their influence was often limited. As a result, leaders felt frustrated in a very complex commissioning environment for obtaining services to meet the mental health needs of people under probation supervision.
Inspectors were also concerned that despite the fact that cases could be selected by the presence of a flag for mental health risks and need, and/or self-harm/suicide, none of the inspected bodies were able to provide reports which would provide a comprehensive analysis of mental health needs across their caseloads. As a result, the potential for management information systems to inform service delivery had not been maximised or fully realised. In addition, little information was available with regards to the outcomes of interventions or how this had informed any strategic needs analysis.
Discussion
Inspection findings, including the life stories and insights of those with lived experience of mental health in the CJS, emphasised some of the factors which appear to help or hinder the progress and life quality of these individuals. Mental health needs were often not fully identified, with flagging of mental health across assessment systems appearing ‘muddled and inconsistent’. Staff were also not always making use of the range of sources of information available. Many staff believed they lacked the skills and training to work with this population of individuals, some of whom had complex needs, including co-morbidity. Managers similarly expressed that they too often had limited understanding of how best to work with those with mental illness, leading to a lack of confidence in providing support to their staff. Interviews with those who had lived experience of mental health needs while in the CJS emphasised that while positive relationships between themselves and criminal justice staff had the potential to support their mental health, this could be undermined where these relationships were poor. Aspects of case management show considerable room for improvement. Even taking into account the restrictions caused by the COVID-19 pandemic, mental health services were not being used well. Concerns around GDPR and breaching confidentiality meant that probation staff were often left unable to access relevant details from other agencies relating to those individuals under their supervision. Complex commissioning and lack of community provision led to many being unable to access the required services in a timely manner, if at all. National health and well-being strategies and priorities did not appear to be driving local policy, and while there was commitment to achieving positive mental health outcomes, there was also acceptance that much remained to be done.
Effective practice: Where we see out standards delivered well in practice
The inspection findings highlight a range of concerns in regard to the experience of those with mental health needs and disorders in the CJS. However, it is important to note that inspectors also witnessed many pockets of good practice across the fieldwork areas, as well as speaking with dedicated, experienced and hard-working staff who worked relentlessly to support those under their supervision. The lessons learned from these areas and individuals contributed to the production of an Effective Practice guide on mental health, intended to support practitioners, middle managers and strategic leaders to reflect on their experiences in practice and consider how they may apply the salient learning points to their own context (HM Inspectorate of Probation, 2022b).
A set of ‘guiding principles’ emerged for where our standards were being delivered effectively in relation to mental health service delivery. At the pre-sentence stage, effective interactions should be undertaken with sentencers to promote the sentence most likely to support and bring lasting change to the individual. For each individual, there should be an accurate identification of the extent of their mental health needs, followed by a robust assessment and comprehensive plan to address these needs. Where mental health appears to be more complex or severe, suitable and specialist assessments should be undertaken.
There should be evidence of trauma-informed approaches to working with these individuals, as well as full consideration given to diversity needs, with personalised activity planned and delivered to meet these needs. Robust information-agreements and protocols should be in place between local criminal justice partners to allow for the timely and efficient sharing of information which will best support the individuals under supervision, with multi-agency ownership and accountability across all stages of case management.
Practitioners should have the skills to allow them to meaningfully support lapses in the behaviour of those under their supervision and to advocate persistently for the right services. To support practitioners, an effective learning and development offer should be made available to help them understand how to work best with vulnerable people who have mental health needs. Where staff identify and experience effective ways of working with this population, the learning should be shared to enable good practice across the organisation.
To support all this work, leadership should be dynamic, and an unambiguous national strategy should be in place which positively guides and influences practice at a local level. Vigorous analysis and use of management information and data should be undertaken to identify need and inform service delivery.
Moving forward: Taking steps to improve practice
The findings of the inspection yielded recommendations for the range of health and justice partners who play a role in providing support for individuals with mental health needs and disorders in the CJS. Most of these were accepted by the relevant agencies, who proposed actions as to how these would be undertaken. 8 While there is not space to go into all the agreed actions here, a few are especially worthy of comment.
As in 2009, inspectors recommended that a joint definition of mental illness be agreed by Health and Justice partners. In response, relevant agencies believed that the internationally agreed clinical definition of mental disorders set by the World Health Organisation was the most appropriate 9 and that no new definition needed to be established. They did, however, recognise that further work was required in relation to identifying and recording mental health needs, and committed to a number of activities aimed to improve the ways in which staff identify, flag, harmonise and share information about an individual’s mental health, including the review and promotion of relevant guidance. Time will tell whether this established definition is sufficient to alleviate the issues caused by the wide variance with regards to the identification (or lack thereof) of mental health needs and if it is specific enough to support consistent flagging to ease transitions from one stage to the next.
However, if mental health needs are going to be consistently identified, staff also need to have the required knowledge and training to work with those with mental health disorders as well as explaining to those under their supervision why they are being asked certain questions. In response to recommendations, all agencies identified a range of awareness and/or training relating to mental health, which is currently available within their organisation, as well as a commitment to undertake additional training where gaps were identified. Yet what is also of crucial importance is the recognition that staff training is not just about awareness of signs and symptoms but that any training should also be trauma-informed as well as emphasising the function and value of relationships in criminal justice work. In addition, investment should be made in the supervision of practitioners to not only aid their understanding but also to help build reflective skills that will increase their capacity to show kindness and empathy.
All of this requires time and space, and this is something which those working in probation have in short supply. Inspections have consistently revealed dedicated, committed and compassionate staff who feel significant frustration, stress and at times, a lack of control due to the untenable number of cases they are holding alongside the many additional tasks which form part of their role (HM Inspectorate of Probation, 2022a). Only once this is made manageable will they be able to take advantage of available training, have time to absorb the learning, apply it to their practice and reflect on this with colleagues and managers.
Furthermore, all the work on identifying mental health and assessing need will be in vain if the required services are not available for those in the community. The inspection report included a number of recommendations to try to ensure that the needs of people in the CJS are given proper regard when commissioning mental health assessment and treatment provision. Both NHS England and the Welsh Government have current and ongoing plans to identify the levels of need in both the prison service and the wider CJS. It is also crucial when commissioning services that the diverse needs of the criminal justice population are taken into consideration, including ethnicity and gender. In addition, those with co-morbidity – such as those who have mental health needs alongside neurodiversity and substance issue – are often served poorly, and risk having one or both their needs neglected. However, given the complexity of need, dual diagnosis and challenging lifestyles which some of these individuals face, more leniency for missing appointments and support should be made available, as being denied access to this treatment can cause anxiety and a worsening of mental illness for these individuals (for more information on probation and substance misuse services, see Ball, K in this edition).
Conclusion
In the foreword to the inspection report, Justin Russell, Chief Inspector of Probation, noted that it ‘highlighted some worrying and disappointing findings’ and that ‘not enough progress has been made in over a decade a decade since the 2009 recommendations’. This article has identified the main challenges that are still being experienced within the probation service with regards to the identification and treatment of those with mental ill health. It has also highlighted the crucial role which criminal justice staff can play and the supporting or undermining impact of their relationships with those under their supervision.
Due to the high levels of mental health need amongst those supervised by the probation service, as well as across the CJS as a whole, it is of the utmost importance that improvements are made. Initial plans in response to recommendations appear encouraging. In addition, Skills for Justice have recently been commissioned by HM Prison & Probation Service (HMPPS) to develop a new Adult Health Care Well-being Core Capability Framework for staff in the prison and probation service working with individuals who have health, care and well-being needs. This framework intends to outline the core knowledge, skills and behaviour required to understand and recognise individuals who have such needs, the support available to them and the ways staff can help them access that support. 10
The unified probation service provides a good opportunity to ensure that commitment is secured from senior leadership in this area and that it filters down into consistent action and strategy at a regional level. However, it seems likely that challenges will remain with regards to the lack of clarity around commissioning arrangements and the poor availability of diverse and high-quality services. Even with HMPPS placing a focus on health and well-being, there are challenging times ahead, which leads one to feel some unease with the extent to which mental health needs can be fully met in the CJS.
Footnotes
Acknowledgements
With thanks to Dr Sarah Lewis, David Haze, Justine Best and Mark Borg from Penal Reform Solutions (PRS) for providing the lived experience element of this inspection. Extracts from their report (Penal Reform Solutions, 2021) are included in this findings section. Thanks also goes to those individuals who shared their stories and allowed us to gain a deeper insight into this important matter. Thank you to Kevin Ball and Dr Robin Moore from HM Inspectorate of Probation for their role in editing and commenting on this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.