
Abstract
The burden of asthma in most rural America is mirrored in part by the state of West Virginia, with a 2.2% higher rate than the national average. Most rural residents live in small communities of population size < 3000. While studies have reported on asthma management interventions elsewhere, only a few involved such small rural environments. Because of the unique socioeconomic demographics and challenges faced by these communities—including geographic isolation, indoor exposures to secondary tobacco smoke, and limited access to health care—school children and their families should be educated in asthma management skills. This article focuses on a school-based intervention approach for students and an assessment of their parents’ support and knowledge gained during the intervention. Although the school-based asthma education increased participating students’ asthma management skills, 3 major challenges emerged: Some parents exhibited persistent adverse behaviors in controlling asthma triggers in their homes; a small percentage of parents had little knowledge of irritants or asthma triggers; and some parents were unwilling to consent to their children’s participation in a school-based asthma education intervention. These challenges may be important to address in future asthma interventions aimed at hard-to-reach small rural communities.
Asthma is one of the most common chronic conditions among children, with almost 10 million diagnosed with the disease, which is attributed as the most common reason for hospitalization and a leading cause of missed school days in children aged 3 to 12 years.1-4 Children from low socioeconomic backgrounds and medically underserved populations, including minority families, are the most vulnerable to asthmatic episodes.4-8 While 21% of the US population live in rural areas, 8 the prevalence of asthma in children younger than 18 years may be higher than urban rates. 9 In West Virginia—the second-most rural state in the country, which lies in the heart of Appalachia—the prevalence for asthma is 2.2% higher than the national average. 10 West Virginia is known to have its own culture: a history of economic underdevelopment with high rates of unemployment, low adult educational attainment, poverty, poor housing stock, and high rates of chronic diseases, including asthma.11,12 During the 2004-2005 school year, there were nearly 13 000 asthma cases in West Virginia public schools, accounting for 21% of the overall 62 000 cases attended by school nurses. 13
Because of these rural demographics, young children encounter indoor air quality challenges from exposures such as secondary tobacco smoke.6,7 They also experience increased recurrent emergency department use for primary care. 14 In addition, there is a shortage of physicians and subspecialty medical care services in most small rural communities, thus resulting in children not being treated by a specialist for their asthma. 8 Given these health disparities, interventions modeled to simultaneously address access and disease management are certainly warranted. Studies have reported that asthma education can improve lung function and decrease emergency department visits, increase self-efficacy, and reduce school absenteeism.5,6,8,15,16 In parents, discrepancies in perceptions of asthma severity can be reduced by increasing their understanding of the disease and their asthma management skills. 17
Schools offer a location to efficiently reach children with asthma because they spend most of their weekdays in these environments.8,18 Proponents of successful programs have reported that interventions in disadvantaged populations should be culturally sensitive, to derive maximal impact. 19 Additionally, a few studies have reported that optimal asthma management requires that the caregiver and the child both be knowledgeable about the disease so that they can aptly comply with an effective regimen of care.3,20,21 While studies have reported on the impact of asthma education in different regions and diverse communities (including urban areas), few studies have reported on geographically isolated populations.20,22 We do not know of the acceptance or feasibility of a school-based program in disadvantaged, hard-to-reach small rural communities in West Virginia (populations < 3000), which are similar to many communities throughout Appalachia.
The purpose of this study was to demonstrate the feasibility of a school-based asthma education (SBAE) program for students (third to fifth grade) and to evaluate parents’ perspectives of the intervention.
Methods
The study was accomplished in 2 ways: first, by implementing the SBAE intervention for children, with parental participation, through homework assignments and through evaluation of the intervention’s impact on students using a preassessment-postassessment format; second, by administering a cross-sectional follow-up interview survey to parents with children in the SBAE. The study organization and implementation were carried out from October 2004 to July 2005.
The SBAE Intervention for Children
The SBAE intervention used school- and community-based volunteers who were trained by the local American Lung Association in a 1-day session. Specifically, the volunteers learned how to help implement the intervention using the Open Airways for Schools curriculum for students in grades 3 to 5. 18 Volunteers included a teacher and office staff member (n = 2), parents (n = 4), and senior nursing students assigned to the school nurse for their community health experience (n = 2). The efficacy of the Open Airways for Schools evaluation tools has been established in other studies,5,18,21,23 and it covers topics on how to (1) identify asthma causative agents in the environment; (2) identify asthma triggers such as dust mites, pets, molds, pests, and irritants (eg, secondhand smoke); (3) manage an asthma attack; (4) understand drug therapy and compliance; and (5) implement inexpensive methods of managing unavoidable allergens.
Recruitment and eligibility criteria
Students enrolled in grades 3 to 5 and those having documentation of asthma diagnosis in the school nurses’ records were eligible to participate in the SBAE. An enrollment package was sent home with a child, which included a letter of invitation detailing the nature of the intervention, the expected responsibilities of the student and parents in the study, a parental consent form, and a child assent form. Recruitment reminder cards were sent home with the child 2 times within a 2-week interval. In addition, telephone follow-ups were conducted to verify that the parents received the package (Table 1). To be eligible to participate in the SBAE intervention, a student had to provide an assent form along with a consent form signed by a parent or a guardian.
Parent Telephone Recruitment Conversations and Intentions to Give Child Consent to School-Based Asthma Education Intervention a
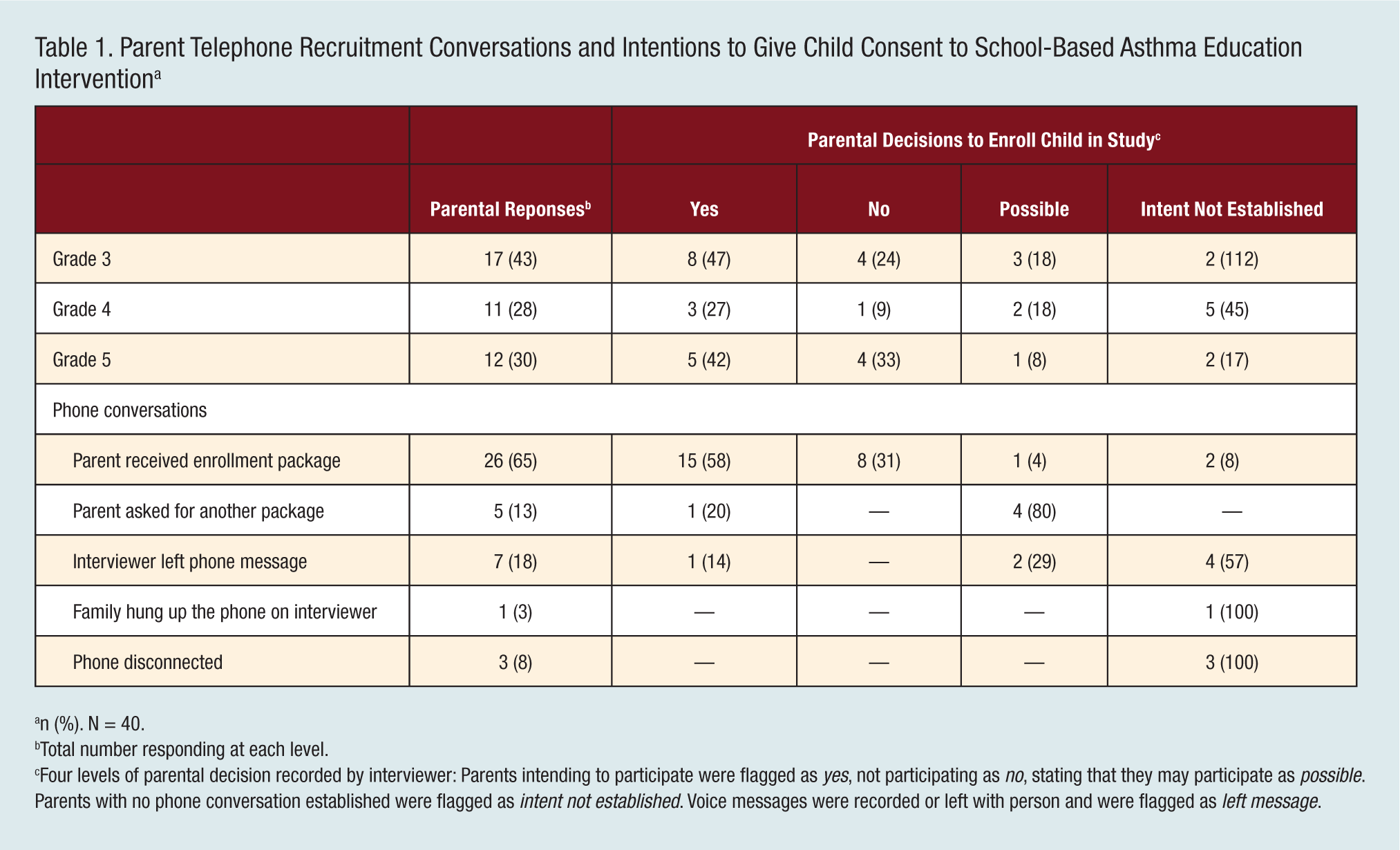
n (%). N = 40.
Total number responding at each level.
Four levels of parental decision recorded by interviewer: Parents intending to participate were flagged as yes, not participating as no, stating that they may participate as possible. Parents with no phone conversation established were flagged as intent not established. Voice messages were recorded or left with person and were flagged as left message.
The SBAE intervention
The SBAE was carried out from January to March 2005. To accomplish this objective, the students were released from class once a week for 40 minutes to participate in the intervention program. During the first session, a pretest was given to assess the student’s preintervention knowledge, and a posttest was given during the last sessions of the intervention. After each lesson, an Open Airways for Schools letter addressed to the parent/guardian was sent home through the children. The first part of the letter explained aspects of the lesson taught the preceding school day—for example, “Today in Lesson 2 your child learned about some tools to help manage asthma: peak flow meters, asthma medications and asthma action plans.” The second part of the letter was addressed from the child to the parent/guardian, seeking help in answering questions—for example, “Today in Lesson 2, I am trying to learn more about the medications I have to take for asthma. Please help me by answering the questions below. We will talk about medications during our next class.” The third and final part of the letter then listed the questions that the parent and child were expected to discuss and answer, such as “What are the names of my asthma medication?” “How does my doctor say I should take them?” and “What do you think is the biggest problem with my medication?”
Parent telephone interview
Eight weeks after the SBAE ended, a follow-up interview was administered to parents of children who had participated in the intervention. The primary goal of the follow-up interview was to ascertain if the SBAE intervention increased the asthma knowledge of parents through their participation in homework assignments (ie, indirect learning). 24 The interview also assessed changes in the parental strategies to control asthma allergens and irritants in the home following the intervention.
The survey instrument comprised 4 sections: (1) demographics, including the educational level of parents, family income, health insurance coverage for children, and size of household; (2) the indoor environmental exposures; (3) parents’ perceptions of common irritants and triggers; and (4) parents’ perceptions of the SBAE intervention. The survey contained a 32-item questionnaire designed by the investigators as based on a review of published medical literature. The questionnaire was pretested with nonparticipating adults for face validity before implementation and determined to be comprehensible and suitable for telephone implementation.
A telephone interview was chosen over a mailed questionnaire, which gave the interviewer an opportunity to answer or clarify respondents’ questions during the assessment. Telephone calling sessions were made in the morning, afternoon, and evenings. No calls were made earlier than 9:00
Institutional Review Board
The study was approved by the West Virginia University Institutional Review Board. Matching or identifying child-parent responses was restricted by the board for confidentiality owing to the involvement of the school personnel, parent volunteers, and student participants.
Data Analysis
The Open Airways for Schools prequestionnaire-postquestionnaire responses were categorized into can’t tell, might tell, and can tell levels of asthma management ability skills. For the purpose of analysis, each student’s response to each question was assigned 1, 2, and 3 points to the 3 Open Airways for Schools categories, respectively. In accordance with the current recommendations in literature pertaining to analysis of ordinal data, 25 a Wilcoxon signed-rank test was performed on the students’ preresponse-postresponse to each question to assess the change in asthma knowledge and the prevention and management of the disease. Parental responses to the interview survey were analyzed descriptively. Data was analyzed using SPSS 15.0. Results are reported as mean and percentage, where appropriate. A P value ≤ .05 was considered statistically significant.
Results
Participants
The elementary school had 586 students, 75 (12.8%) of which had a diagnosis of asthma recorded in the school nurse register. Forty students were identified as potential participants in the SBAE intervention. During the telephone calls, 26 parents indicated they had received the recruitment package; 16 intended to participate; 9 did not intend to participate; and 6 stated that they may participate and were thus flagged as possible in the codebook. No phone conversation was established with 10 parents, and they were flagged as “intent not established.” Voice messages were recorded or left with the person answering the phone, and these were flagged as left message (Table 1). After subsequent telephone calls and postcard reminders, 18 students obtained consent to participate (2 of whom were siblings, resulting in 17 households), comprising a 45% recruitment rate in students.
In the follow-up interview with parents, 8 initial sessions of telephonic contact were conducted in the first week, which resulted in collection of data from 11 participants. Five additional calling sessions were made in the second week, in an attempt to increase the number of respondents, which resulted in the acquisition of 2 additional participants. Of the 17 potential parent participants, 13 (77%) agreed to participate in the telephone interview. One parent refused, and 3 could not be contacted by postcards or telephone.
Family Demographics
Of the participating parents, 52% had a college degree or higher; the rest had a high school diploma. Forty-six percent reported an annual household income of $40 000 to $70 000; 30%, an income of $20 000 to $40 000; and 16% earned ≤ $20 000. Most of the families lived in a standard house (n = 11); 1 family lived in a mobile home. All participants indicated that they had health insurance coverage for their children, which included private insurance (54%), Medicaid (39%) and Children’s Health Insurance Program (7%). Ninety-two percent reported that their children had a physician’s diagnosis for asthma and that 54% had undergone allergy testing. Thirty percent of the families had more than 1 person with a diagnosis of asthma.
Impact of the SBAE intervention in students
In sum, 100% of the participants (n = 18) returned the Open Airways for Schools letters, as signed by a parent indicating parental participation in the homework assignments. The pretest results showed that 62% of the students had knowledge on when to take their medication, compared with 88% posttest. At pretest, the majority of the students could not tell what made them wheeze at home (54%) and at school (62%), compared with only 19% and 25%, respectively, at posttest. At pretest, 46% of the students could tell when they should go to the hospital because of asthma, compared with 94% at posttest. A Wilcoxon signed-rank test showed a statistically significant difference (P ≤ .05) between the pretest-posttest in knowledge on “what makes them wheeze at school” and “when to go to hospital” (Table 2). When asked to circle a face that showed how they felt about their asthma, 72% of the students indicated that they were either sad or very sad in the pretest and posttest periods.
Student Participants’ Pretest-Posttest Responses to the School-Based Asthma Education Questions a
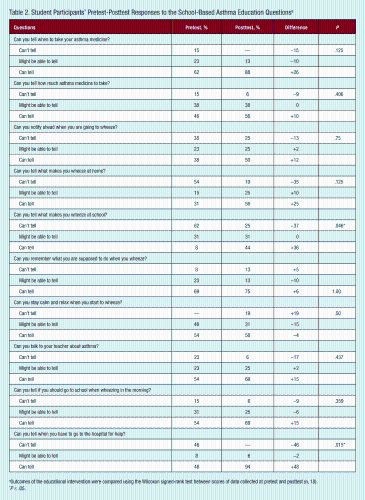
Outcomes of the educational intervention were compared using the Wilcoxon signed-rank test between scores of data collected at pretest and posttest (n, 18).
P ≤ .05.
Perceptions of parents to the SBAE intervention
In sum, 100% of the parents felt that the intervention was effective in increasing the children’s knowledge regarding asthma irritants and that it enabled children to more effectively manage their asthma (Figure 1). Furthermore, 77% reported that their children’s symptoms had improved following the intervention. Fifteen percent reported that they made changes in their homes following the intervention and installed plastic mattress covers for the children with asthma (77% were already using covers).
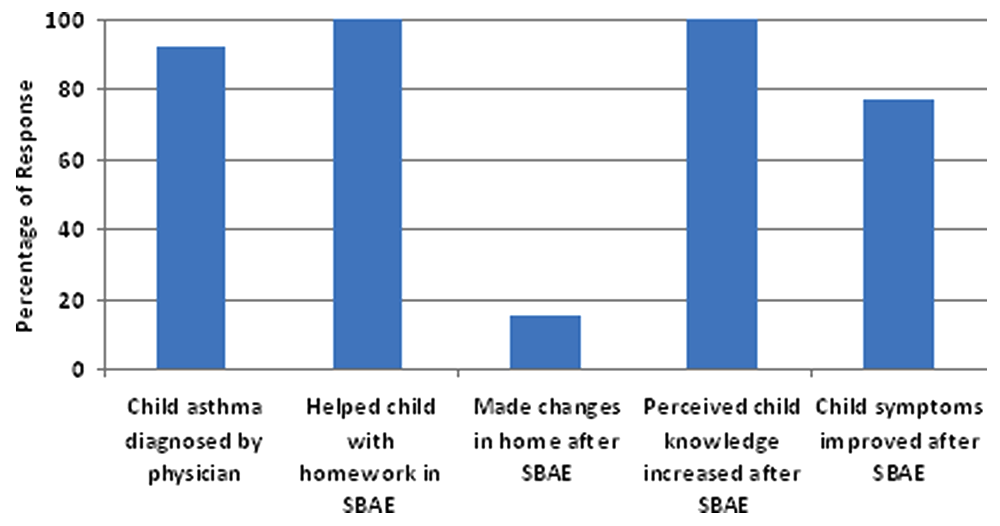
Parents’ Perceptions of the School-Based Asthma Intervention. Interviewer: “Now I have just a few more questions pertaining to the school-based asthma education program that has occurred at your child’s school.”
Parents’ perceptions of indoor environmental asthma triggers
Thirty-one percent of the parents reported that someone in the household smoked tobacco (the father was the most prevalent smoker in the household), and 12% smoked inside the house, as well as inside the car in the child’s presence (Figure 2). Sixty-two percent reported that they observed molds or mildew in the home, mostly in the basement. Forty-six percent of the parents allowed pets in the home and in the child’s bedroom. Fifteen percent used woodstoves as their main source of heating.
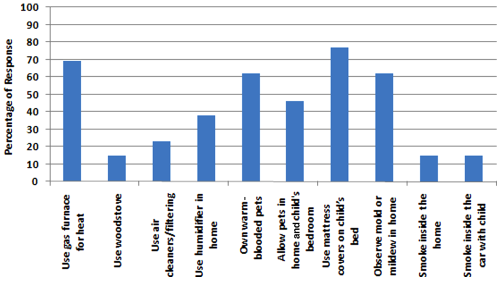
Parents’ Perceptions of Indoor Environmental Asthma Triggers. Interviewer: “For this next section, I am going to ask you a series of questions about your home environment.”
Parents’ perceptions of asthma irritants and triggers
Figure 3 shows the parents’ knowledge and perceptions of environmental exposures to asthma allergens and irritants. When the parents were asked “Do the following affect asthma symptoms?” 8% thought that cigarette smoke was not an asthma irritant, whereas 23% thought exposure to dogs and cats and to pollen did not affect asthma symptoms. When the parents were asked to indicate other conditions that they thought were asthma triggers or irritants, 33% indicated physical activity, pollution, smoke, odors, and heat.
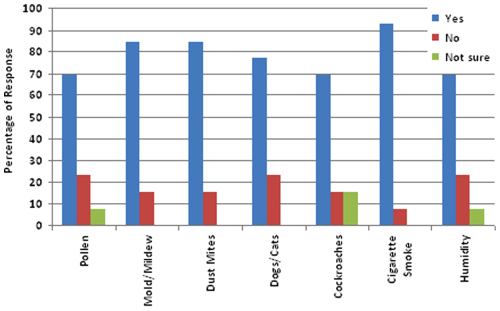
Parents’ Perceptions of Asthma Irritants and Triggers. Interviewer: “For this next section, I am going to ask you a series of questions about your perceptions on various things that may be in the home, and whether you feel they relate to your child’s asthma symptoms. Do the following affect asthma symptoms?”
Discussion
The school setting offers a unique opportunity to reach out to many children with limited access to health care and to educate them on managing their asthma condition.15,16,26,27 Our study provided an opportunity to explore the feasibility of a SBAE intervention in a hard-to reach small rural population. Volunteers, which included parents, teachers, school office staff, and nursing students, were readily available to assist with the program. Asthma education programs that include teachers and administrative staff are better prepared to effectively respond during an urgent situation at school.
Parents play a pivotal role in their children’s asthma management, including compliance with all facets of medical care and instituting appropriate environmental care in their homes. In this study, parents received concise responsibilities and instructions for each homework assignment and reported that they helped their children during the intervention. Barriers such as socioeconomic status and accessibility to care can be detrimental to parents’ participation in a community-based education program. Because of geographic isolation and the poor public transportation system in these small rural areas, the SBAE for the students during school hours and the indirect education for parents through homework assignments appear to be a feasible strategy. 24
Although parents reported a high level of asthma knowledge, compliance to recommended environmental remedial approaches showed persistent adverse behaviors. Fifteen percent of the parents reported that they continued smoking in the house and in the car in the presence of a child with asthma. Although the parents reported that they recognize pets such as cats or dogs as asthma irritants, 46% reported that they allowed the pets in the house and in the bedroom of a child with asthma. Having a dog and a cat in the home has been shown to be a source of residential exposure to endotoxin, which may worsen respiratory symptoms in asthmatic children. 28 Our findings corroborate other studies that suggest that knowledge of asthma risk factors alone is not a sufficient incentive to change negative behaviors that affect health.21,29
The other compliance factor was that of diagnostic testing, where 46% of the parents reported that their children had not undergone allergy testing. The low rate of allergy tests reported by parents in our study shows a discrepancy in understanding the severity of the disease and what an allergy test can signify. An allergy test is an important step in the diagnosis and control of asthma, and it can reinforce the need to eliminate particular irritants and allergens in the home. 30 Whereas the majority of the parents perceived exposure to pollen, molds, dust mites, dogs and cats, and cigarette smoke as irritants or asthma triggers, the small percentage that had no knowledge should not be disregarded. There is a need for the continued education of the parents, with an emphasis on allergy-free indoor environments.
Limitations
Our sample size was too small to generalize the results to a larger population. There was low participation in spite of our recruitment efforts, which included follow-up telephone calls and postcard reminders during the SBAE and the parental interview. Low participation in studies in rural areas is a common challenge. Other studies have reported factors such as prioritization of family needs, 26 concerns about health research, 31 or simply voluminous pages of consent forms to read and sign.32,33 Studies have also reported that parents in rural settings are frequently skeptical to the introduction of outsiders and new concepts and that these perceptions may be linked to culture and isolation.12,26,27 Others have postulated that parental refusal to participate in research may be due not to lack of interest but rather to fulfilling their legal and parental role to protect and do what is best for their children. 34 Another factor could be distrust of unknown health trainers or low level of confidence in the medical supervision provided at schools. 31
An additional limitation was that eligibility to participate in the SBAE was restricted to students who had an asthma diagnosis in the school nurse records. There may be students with asthma in the school who were not in the nurses’ records. Also, it is conceivable that highly motivated parents with higher-than-average education, moderate family income, and access to care predominantly consented to participate in the study. All participants had either private or federally sponsored medical insurance for their families. These parents conceivably understand that asthma is a major health problem for their children. Nonparticipating parents could shed some light on their understanding of asthma as a problem in their children and the hardships encountered in the disease management. But funding resources to address these issues were a major limitation. Despite these limitations, the study yielded information that can be incorporated in designing appropriate recruitment and acquiescence approaches in future interventions targeting populations in small rural areas.
Conclusion
This study demonstrated the feasibility of involving children and their parents in a SBAE in small rural communities. While the SBAE increased students’ asthma management skills, 3 major challenges emerged: Some parents exhibited persistent adverse behaviors in controlling asthma triggers in their homes; a small percentage of the parents had little knowledge of irritants or asthma triggers; and some parents were unwilling to consent to their children’s participation in an SBAE intervention. These challenges may be important to address in future asthma interventions aimed at hard-to-reach small rural communities.
Footnotes
Acknowledgements
We thank the elementary students and their parents, the teachers, the nursing student volunteers at the elementary school, and the American Lung Association of West Virginia for their participation in the in-school asthma program. We thank the Preston Memorial Hospital Respiratory Therapy Group and the Garrett Memorial Hospital for the demonstration of respiratory devices and equipment to the students at school.
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
This work was supported in part by a grant contract No. XA-97300101-0 from the Environmental Protection Agency, 2004-2005. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Environmental Protection Agency.