
Abstract
Objective. The prevalence of bronchial asthma is increasing globally by 50% every decade. With more individuals presenting with a medical history of asthma and concurrent medication usage, its impact on oral cavity needs to be recognized. The present study was conducted with an aim to assess the oral health status of individuals with asthma aged 12 years and older and to evaluate the effect of various antiasthma medications on oral health. Materials and Methods. Forty individuals with asthma (22 females and 18 males) between 12 and 66 years of age were included in the study after following extensive exclusion criteria. For all subjects a detailed case history was taken. A thorough oral examination was conducted to determine caries experience, periodontal status, and candidiasis. Furthermore, whole unstimulated saliva was collected for pH estimation and cytological smears obtained for the screening of candidiasis. Results. Of the 40 subjects examined, a history of xerostomia was found in 55%, stomatopyrosis in 22%, and halitosis in 5%. The mean DMFT (decayed, missing, filled teeth) was 4.97. Periodontal treatment need evaluation revealed the requirement for oral hygiene education and professional prophylaxis in most of the subjects. However, no significant correlation was found between use of antiasthma medications and periodontal needs. An acidic pH was found in 52.5% of the subjects and candidiasis was detected in 65%. Conclusion. A high incidence of xerostomia, acidic pH, and candidiasis was found in those having asthma. Studies with a larger sample size may help confirm these findings. However, it is suggested that asthma patients on regular antiasthma treatment need special attention in the area of oral health care.
Bronchial asthma is a chronic respiratory disorder affecting approximately 300 million people worldwide and 45.7 million in Southeast Asian countries alone. 1 The severity of the symptoms in an individual determine the treatment modalities used, such as use of β-2 adrenergic receptor agonists, inhaled or oral corticosteroids, antihistamines, and mast cell stabilizers. 2 Asthma status and the concurrent usage of medications may result in a higher incidence of dental caries, periodontal diseases, halitosis, alterations in salivary flow and pH, xerostomia, oropharyngeal candidiasis, burning mouth, geographic tongue, perioral dermatitis, and angina bullosa hemmorhagica.3,4 However, the aforementioned conditions may be modified by individual oral health care habits, dietary habits, and adverse habits such as smoking and alcohol intake.
Most past studies have assessed the oral health status in adolescents and children with asthma, and very little information is available with regard to the adult population. The present study was designed to assess the oral health status of individuals with asthma aged 12 years and older and to evaluate the effect of various antiasthma medications on oral cavity.
Materials and Methods
A total of 40 individuals diagnosed with asthma (22 females and 18 males) were included in the study. The age of the subjects ranged between 12 and 66 years. Informed consent was obtained from all subjects. Individuals with systemic conditions affecting salivary flow and periodontal health were excluded. Also, subjects with conditions known to increase predisposition to candidiasis were excluded from the study. Furthermore, pregnant women, lactating mothers, and individuals on medications known to affect the salivary pH and flow were also excluded from the study group.
A detailed history with regard to their asthma status, such as frequency and severity of asthma episodes, precipitating factors, and an elaborate drug history, was recorded. A history of oral symptoms, such as tooth sensitivity, tooth pain, bleeding gums, dry mouth, burning sensation, and halitosis, was also recorded.
A thorough oral examination was performed per the World Health Organization (WHO) guidelines. 5 The DMFT (decayed, missing, filled teeth) index was recorded in each subject and then the mean DMFT score was calculated. The oral hygiene of all the subjects was assessed using the Modified Oral Hygiene Index. The periodontal status and subsequent treatment needs were recorded with the help of World Health Organization and Fédération Dentaire International–specified Community Periodontal Index for Treatment Needs (CPITN) index. 6 Subsequently, a statistical analysis was performed using χ2 test to establish the correlation between the use of antiasthma medications and periodontal status and subsequent periodontal needs.
The oral cavity was also examined for the presence of candidal lesions. A clinical diagnosis of candidiasis was made in subjects presenting with pseudomembranous, erythematous, or nodular or plaque type of lesions. 7
A cytological smear from the posterior one third of the hard palate was obtained in all subjects. In subjects who were clinically diagnosed with candidiasis, an additional smear of the candidal lesion was obtained. The cytological specimens were stained with periodic acid Schiff (PAS) and examined under a light microscope for presence of candidal hyphae and yeast cells using multiple fields of vision.
Whole unstimulated saliva was obtained in all subjects 2 hours after meals in a test tube and the pH was tested using a wide range pH (2-10.5) indicator kit from SD Fine Chemical Limited (Mumbai, India). The pH indicator strips were dipped in salivary samples for 15 seconds and inspected for any change of color. The color change was compared with a reference chart to obtain a pH value.
Results
Of the 40 subjects examined, 54% were on β-2 agonists and corticosteroids, 35% on β-2 agonists, 3% on corticosteroids, and 8% on alternative medications or had not received any treatment.
With regard to the oral symptoms, 55% of individuals with asthma reported dryness of mouth or xerostomia. Stomatopyrosis or burning mouth and halitosis or bad breath was reported by 22% and 5% of the subjects, respectively.
The mean DMFT was found to be 4.97. The oral hygiene index scores revealed that 65% of the subjects had fair oral hygiene and 35% subjects had maintained good oral hygiene.
The assessment of periodontal needs using the CPITN index revealed that 72.5%, 10%, and 17.5% subjects belonged to TN2, TN3, and TN1 category, respectively. No significant correlation was found (P = .308) between use of antiasthma medications and the CPITN index.
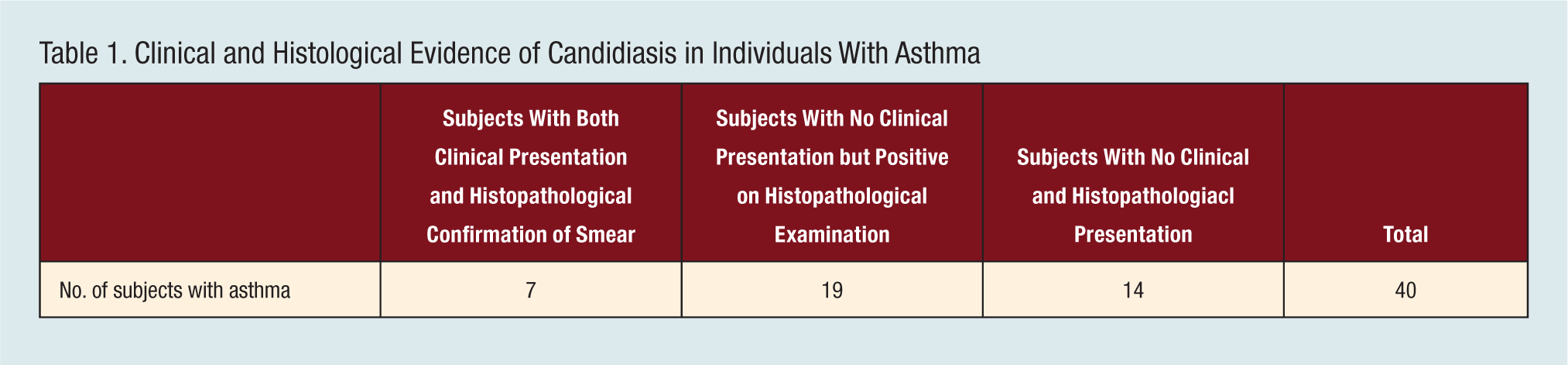
Clinically, candidal infection was detected in 17.5% of the subjects. Candidiasis manifested in these individuals in the form of erythematous areas, most commonly on the palate followed by the tongue and the buccal mucosa. PAS-stained cytological smears were positive for candidal infection in 65% of the subjects; however, 47.5% of the cases showed no clinical evidence (Table 1).
Clinical and Histological Evidence of Candidiasis in Individuals With Asthma
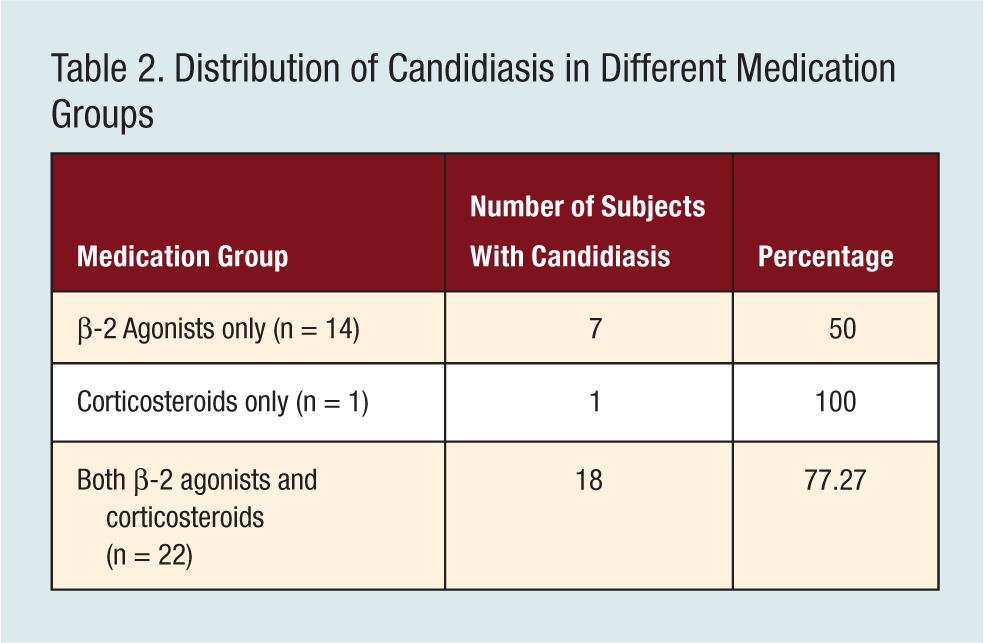
The prevalence of candidiasis in subjects on combination therapy (corticosteroids and β-2 agonists) was found to be 77.3%. Fifty percent of the subjects on β-2 agonists showed histologically positive candidal infection. One subject on corticosteroids therapy alone also had candidal infection (Table 2).
Distribution of Candidiasis in Different Medication Groups
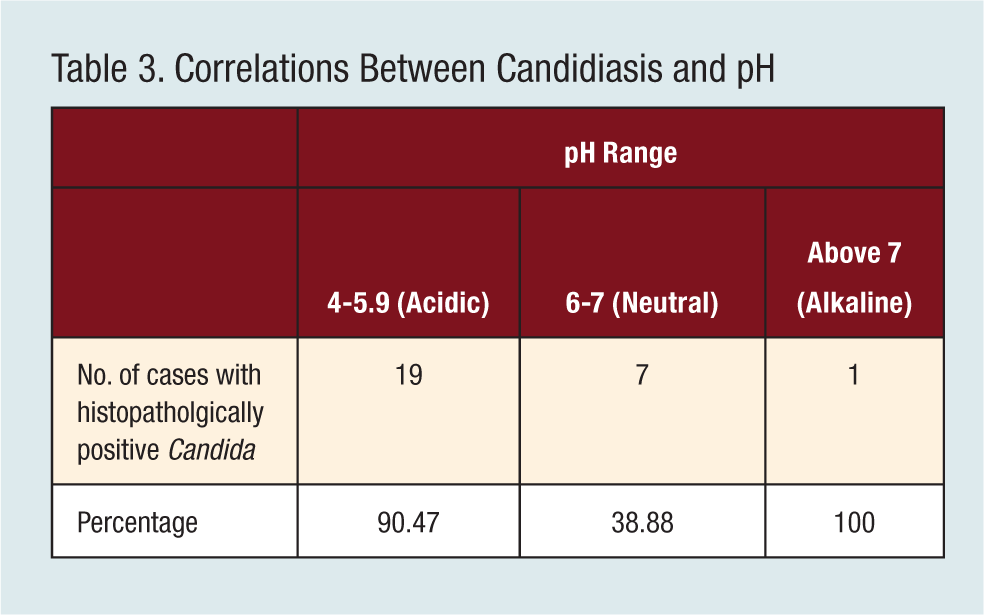
Acidic pH (4-5.9) was found in 52.5% of the subjects, whereas 45.0% had a pH ranging from 6 to 7. Only 1 subject had an alkaline pH. Subjects with an acidic pH showed a mean DMFT of 4.7 and a high prevalence of candidiasis (90.4%; Table 3).
Correlations Between Candidiasis and pH
The salivary pH values were compared among subjects on different antiasthma medications. A total of 58.3% of the subjects on β-2 agonists either exclusively or in combination with corticosteroids had an acidic pH.
Discussion
In India, according to the National Family Health Survey-3, asthma has an equal predilection among adult men and women. 1 In this study, a slight female predilection was noted, but this was not found to be significant.
The clinical course of asthma is variable. It is persistent in some individuals and progressive in others. 1 Hence, the treatment instituted depends on the severity of the disease. The commonly used antiasthma medications are β-2 agonists in mild episodic asthma, low-dose corticosteroids in mild cases with occasional exacerbations, and a combination therapy of both the aforementioned medications in moderate to severe asthma cases. 2 Asthma status and the related medication use have been reported to result in certain oral signs and symptoms.
Studies have reported a high prevalence of xerostomia in asthma patients. β-2 Agonists are probably responsible for the xerostomic condition. Salbutamol and terbutaline, besides relieving bronchospasm, also affect the β-1 and β-2 adrenergic receptors in the salivary glands. 8 This causes inhibition of neural stimuli to the salivary gland and subsequent downregulation of the density of the receptors, resulting in a decreased secretion of saliva and a relative decrease in the proportion of the salivary proteins. 8 It has also been suggested that xerostomia in asthma patients may be the result of increased water evaporation from oral mucous membranes if the patient is a mouth breather. 4 In the present study, 55% of the subjects presented with a history of xerostomia. These subjects were receiving β-2 agonists either alone or in combination with corticosteroids.
Asthma patients may also present with stomatopyrosis or burning mouth. It may be attributed to underlying allergic pathophysiology, reduced salivary flow, and increased predisposition to candidiasis due to antiasthma medications. 4 In the present study, 25% of the subjects presented with a history of stomatopyrosis.
The DMFT status has been a subject of conflict and contradictory studies have been published regarding the prevalence of caries in asthma patients. 4 Dental caries occurs due to a disturbed balance between the amount of saliva and its pH, nature of oral microbiota, tooth structure, plaque pH, and dietary substrates. 9 A higher incidence of caries in asthma patients has been attributed mainly to the action of β-2 agonists, which lower the secretion rate of whole saliva. This results in a subsequent decrease of biologically active components such as amylase, calcium, secretory IgA, and peroxidase. 9 The decreased output of secretory IgA and peroxidase favors both bacterial colonization and plaque growth. Furthermore, the lowered secretion of calcium and amylase may cause an unfavorable effect on the critical pH. 9 Bacterial colonization is also favored by an increase in salivary sugar concentration in patients using syrups as a part of their therapy. 4 In the present study, the mean DMFT in specific age groups was higher than the mean DMFT found in similar age groups in the normal Indian population. 10 However, individual dietary habits, socioeconomic status of the patients, water fluoride content, and oral hygiene habits could also affect the DMFT status of an individual.
A few studies have reported an increased incidence of gingivitis and periodontitis in those with asthma. Hyyppä 11 found that the incidence of gingivitis and the amount of plaque accumulation were higher in children with asthma than those without asthma. 11 Gingivitis in those with asthma is due to an increased amount of plaque and calculus formation in these subjects. Mouth breathing, especially during episodes of acute asthma attacks with subsequent dehydration of alveolar mucosa, also contributes to gingivitis. 4 A study by Yaghobee et al 12 reported a definite relationship between respiratory disease and periodontal health status. This is supported by studies reporting higher incidence of attachment loss in patients suffering from chronic respiratory diseases. 13 The association between asthma and periodontal health has also been attributed to the pathological activation of the immune and inflammatory processes, which result in an increase in the levels of immunoglobulin IgE in the saliva. 12 On the contrary, a few studies have proposed that there is weak influence of secretory immunity and no significant correlation exists between asthma status and periodontal health. 14 Corticosteroids, according to some researchers, may cause a decrement in bone mineral density and contribute to periodontitis. 15
In the present study, all subjects required oral hygiene instructions, with 82.5% of the patients requiring professional treatment. In this study, since no statistical correlation between the use antiasthma medications and the extent of deterioration of periodontal health was found, changes in the periodontium can be attributed to underlying allergy and immunological pathogenesis in asthma along with inadequate oral hygiene practices in the study subjects.
The incidence of oropharyngeal candidiasis in asthma patients has been reported in the literature to vary from 0% to 70%. 3 High incidence of candidiasis in asthma patients has been attributed to the effect of corticosteroids and β-2 agonist medication use. Use of β-2 agonists results in reduction in salivary output and altered salivary composition predisposing the oral cavity to candidiasis. 8
It is not very clear as to how corticosteroids could contribute to candidiasis. The following theories have been proposed. The long-term use of inhaled corticosteroids (ICS) leads to increased accumulation of the drug in certain sites such as the palate and tongue, which results in a local impairment in the defense mechanism of the host. 16 The local side effect is mainly seen among patients who use high doses of ICS regularly. 17 A study by Fukushima et al 18 suggested that ICS can decrease salivary IgA, which can contribute to the development of oral candidiasis. Increased salivary glucose levels due to corticosteroids 19 and dry inhalers containing lactose monohydrate as carrier vehicle have also been reported to cause increased growth, proliferation, and adhesion of candidal organisms. 20 However, some studies have shown that there is no direct effect of corticosteroids on the growth or production of pseudomycelium of Candida albicans in vitro, 16 but this might promote adherence to epithelium by the mechanism of surface receptor interaction.16,21
The present study showed a high incidence of candidal infection, and although only a few subjects had clinically appreciable candidiasis, most cases showed the presence of high concentration of yeasts and hyphae on cytological examination. This result is in accordance with a study by Milne and Crompton, 16 who reported that most patients were asymptomatic with no clinical lesions; however, they were positive for candidal infection on histological examination.
Six out 7 asthma patients with clinically appreciable candidiasis showed erythematous lesions. The literature also shows that the atrophic and pseudomembranous varieties are most commonly seen in patients using ICS. 21 One patient in this study showed inflammatory papillary hyperplasia. Interaction of the expression of basement membrane components and Candida involvement can be attributed to the development of inflammatory papillary hyperplasia of palate. 22
Previous studies have demonstrated a fall in the pH of interdental plaque and saliva during the 30 minutes following the use of β-2 agonists inhalers. 4 In the present study, an acidic salivary pH was detected in 50.5% of the study subjects. Studies have revealed that an acidic pH is conducive for the growth C albicans. The reason for this association may be attributed to increased yeast adherence to epithelial surfaces at low pH conditions. 21 In the present study, candidal infection was found in 90.47% of the subjects with an acidic pH. Furthermore, mean DMFT scores in subjects with asthma with an acidic pH was found to be high, signifying the role of acidic pH secondary to use of antiasthma medications.
A few rare oral manifestations related to asthma status and antiasthma medications have been detected. The presence of geographic tongue in asthma patients has been attributed to an underlying allergic cause. 23 Tongue hypertrophy due to the direct effect of ICS on muscle hypertrophy and local fat accumulation has also been reported. 3 Furthermore, the occurrence of angina bullosa hemorrhagica and perioral dermatitis in asthma patients on ICS has been noted. 3 However, none of the subjects in the present study revealed any of the above findings.
In conclusion, a high incidence of xerostomia, acidic pH, and candidiasis was found in the subjects with asthma. Studies with a larger sample size may help confirm this finding. However, it is suggested that adult asthma patients on regular antiasthma treatment with inhaled medications need special attention in oral health care. An interdisciplinary approach between health care team and oral health care providers is mandatory for the optimal oral health of such patients.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.