
Abstract
Aim:
Adherence to maintenance asthma inhaled therapy remains suboptimal globally. An asthma patient decision aid (PDA) can facilitate shared decision-making between patients and physicians when selecting asthma treatment options. This study aimed to explore the perspectives of the clinicians and patients in the implementation of this PDA in the primary care practice and to identify optimal delivery approaches for its sustainability.
Method:
Thirty primary care doctors, nurses, pharmacists, and 20 patients who were prescribed inhaled corticosteroids were interviewed through focus group discussions and individually to gather their perspectives on using a locally designed asthma PDA. The transcribed qualitative data were analysed and presented using the Normalisation Process Theory framework.
Results:
Platform preferences differed among the patients, with older patients favouring print formats whilst younger patients preferred digital versions. Nonetheless all participants agreed that the PDA should be written in layman’s language, have large font sizes, and good visual design. Most of the clinicians highlighted time constraints as a barrier to PDA use and emphasised the need for easy access to the materials during consultations. Clinicians suggested mutual sharing of experiences with the PDA to address implementation hurdles and facilitate integration into clinical practice and workflow, alongside conducting regular content updates.
Conclusion:
Successful asthma PDA implementation requires multi-format delivery to accommodate diverse patient preferences and streamlined access to address clinician time constraints. Peer sharing and regular content updates are essential for sustained adoption. This study’s findings provide practical guidance for integrating the asthma PDA into primary care.
Background
Asthma is a chronic respiratory condition affecting approximately 339 million people worldwide 1 with significant impacts on quality of life and healthcare resource utilisation. 2 A key contributor to poor asthma control is inadequate adherence to maintenance therapy, particularly inhaled corticosteroids (ICS). 3 Shared decision making (SDM) has been found to increase patients’ adherence to medications and improve asthma outcomes. 4 Patient decision aids (PDA) have emerged as valuable tools to support SDM between healthcare providers and patients. 5
PDAs are structured tools designed to support informed healthcare decision-making by providing patients with clear, evidence-based information about treatment options and their benefits and risks. For patients with asthma, these tools facilitate informed treatment choices by presenting comprehensive information about inhaler medications. They provide details about the benefits and limitations of the different inhaled medications, such as metred dose inhalers versus dry powder inhalers, and inhaled corticosteroids (ICS) alone versus combined ICS with long-acting bronchodilators. 6 In addition, they help patients clarify their personal values and preferences regarding different choices, as what matters most can vary significantly between individuals. PDAs help to enhance clinician-patient communication by creating a standardised framework for discussions about treatment options, ensuring critical information is consistently covered. Patients generally welcome the use of PDA as a form of educational and informational content and having greater involvement in medical decisions. 7 However, in the Asian context, the use of the PDA is limited to information provision instead of SDM as the majority patients still expected the doctors to make the final treatment decision. 8
The use of PDA and SDM in clinical practice faces several challenges. Time constraints in busy primary care settings often pose barriers to consistent use of the PDA and SDM as the discussion takes up additional consultation time. 9 Training clinicians to use the PDA is fundamental to effectively integrate these tools into their routine practice. 10 The PDA needs to be integrated into the care pathway so that clinicians will remember to use it, and that its use is recorded in the patient records to facilitate continuity of care. 8
Patients’ literacy and comprehension of the PDA can also hinder use, as the majority of patient education materials require a minimum reading level of Grade 12, making them inaccessible for low health literacy populations. 11 To ensure readability by the widest range of patients, it is recommended that materials are written at or below US grade 6, even though this can be challenging given the complexity of healthcare topics. 12 Logical layout of the PDA, signposted information, larger text size, labelled visual aids, and use of appropriate and relevant images were found to be important aspects of developing a PDA. 13 PDAs may be delivered in many formats, such as traditional paper-based which is most widely used, and digital formats, including mobile applications and interactive websites. 14 Paper formats offer familiarity and accessibility but face updating challenges, while digital versions provide multimedia features and real-time updates but can be limited by technological literacy. The mode of PDA delivery will impact on clinical workflow and resources required to deliver the PDA, such as printing hard copies of the PDA for paper formats or making digital devices available for digital formats. 15 Timing of PDA delivery is also critical in the time-constrained primary care setting. PDAs may be introduced during consultation, provided as pre-reading prior to consultation, or made available for post-consultation reference. 15
Healthcare-related PDA aims to support decision-making among patients in selecting their treatment option. One randomised controlled trial showed that patients who received the PDA were more certain on their inhaler choice. 16 A PDA was previously designed in a local primary care institution based on a Grade 12 reading level to target patients on Step 2 of the International GINA guidelines (required the use of either daily inhaled corticosteroids or as-needed combined inhaled corticosteroids with long-acting bronchodilators). It was evaluated for its content and layout by multidisciplinary primary care professionals, encompassing physicians, nurses, and pharmacists. 6 Despite the PDAs’ ability to facilitate discussions about inhaler medication, factors such as time constraints, training requirements, and guideline considerations can restrict their implementation. This study explored the perspectives of the clinicians and patients in the implementation of this PDA in the primary care practice and to identify optimal delivery approaches for its sustainability.
Methods
Study Design
This study employed qualitative semi-structured focus group discussions (FGD) for clinicians (doctors, nurses, pharmacists) and one-to-one interviews for patients. Participants were recruited from a network of Polyclinics in Singapore. Polyclinics are large, multi-disciplinary primary healthcare facilities that form part of the government-subsidised public primary care system, with each facility serving approximately 1000 patients per day. The research team incorporated early stakeholder input via a patient and public involvement workgroup that reviewed and refined the study protocol and consent documentation.
Participant Recruitment
Clinicians from various Polyclinics were invited to participate through email invitations, and the clinicians who indicated their interest to join were recruited. Patients were recruited from a single Polyclinic through referrals from the clinicians to the study team. Eligible participants were English-speaking individuals currently receiving ICS treatment. The primary investigator ensured that all patients met the inclusion criteria prior to recruitment. Purposive sampling was used to select patient participants based on age, gender, and education level. Patient demographics from medical records were used by clinicians to identify and refer suitable patients for interviews. Both individual interviews with patients and focus group interviews with clinicians were held in parallel.
Data Collection
All interviews were conducted in-person by the first author at the Polyclinics from January to September 2024 and were audio recorded using a voice recorder. Interviews with patients were scheduled on the day of referral to the study team or scheduled on a separate day to accommodate patient convenience. FGDs with clinicians were scheduled prior. Rapport was established with participants prior to the interview by explaining the PDA and clarifying any questions regarding the PDA. Individual interviews with patients lasted 15-30 min, while FGDs with clinicians lasted 40-50 min. Sessions ended when the interview guide was completed, participants had no additional comments, or practical time constraints were reached (for the clinician participants).
A previously developed asthma PDA was used as the exemplar for this study (Appendix 1). The topics included in the PDA were: What is asthma, what is controller inhaler, signs of asthma attack, evaluation of asthma control using GINA scoring, types of controller inhalers available, concerns of taking controller inhaler, and individual motivations for good asthma control. A semi-structured interview guide was developed for clinicians (Appendix 2) and patients (Appendix 3) based on the 4 key constructs in the Normalisation Process Theory (NPT), (1). Coherence; (2). Cognitive participation; (3). Collective action and (4). Reflexive monitoring. 17 The semi-structured nature of the interviews allowed for real-time exploration of emerging topics of interest within each session, with the interviewer using probing questions to delve deeper into relevant themes as they arose. First, coherence looks at whether people understand what the new practice is and why it’s important. Second, cognitive participation focuses on getting people on board and committed to actually using the new practice. Third, collective action involves the practical work of putting the new practice into everyday use, including decisions about its delivery, making sure they are easily accessible, and fitting them into existing work routines. Finally, reflexive monitoring is about continuously checking how well the new practice is working. Together, these 4 constructs represent the comprehensive work that individuals and organisations must undertake for new practices to become normalised and sustained in routine practice. 17 Successful implementation of interventions is complex, involving both clinician behaviour (attitudes, beliefs, skills, and willingness to adopt new practices) and patient engagement workflows (systematic processes that facilitate meaningful patient participation in healthcare decisions and SDM). 15 This approach was also previously used to implement PDAs in Primary Care. 18 Data saturation was determined using inductive thematic saturation, where no new themes or insights emerged from additional interviews. Saturation was assessed after each interview during ongoing analysis, with the research team reviewing emerging themes after every focus group interview with clinicians, and 2 patient interviews. Saturation was reached after 20 patient interviews and 5 focus groups interviews, when 3 consecutive patient interviews and 2 focus group interviews yielded no new codes or themes, and existing themes were well-developed with sufficient depth and breadth of data.
Data Analysis
Audio recordings were transcribed verbatim by a paid transcriber and verified by another study team member for accuracy before qualitative analysis using Nvivo software for coding and organisation of themes. The qualitative interviews were analysed using the 6-step process of thematic analysis by Braun and Clarke. 19 Data analysis began with thorough familiarisation of the data through repeated reading of interview transcripts and listening to audio recordings. Initial coding involved 3 team members jointly coding the first 3 interview transcripts to establish consistency. Two members then independently coded each remaining transcript. After completing initial coding, the full research team reviewed all codes collectively to the verify coding and identify emerging themes. Following initial coding, codes were systematically reviewed and grouped based on conceptual similarity and shared meaning. Related codes were clustered together, and these clusters were developed into subthemes through team discussion and iterative analysis Following the development of subthemes through inductive analysis, a deductive approach was applied using NPT. Subthemes were systematically mapped and organised according to NPT’s 4 constructs: coherence, cognitive participation, collective action, and reflexive monitoring. This involved reviewing each subtheme and determining which NPT construct it best represented based on the theoretical definitions. Finally, representative quotes were selected to illustrate the findings. The Consolidated Criteria for Reporting Qualitative Research checklist (COREQ) was used as a guide to reporting. 20
Results
Sample
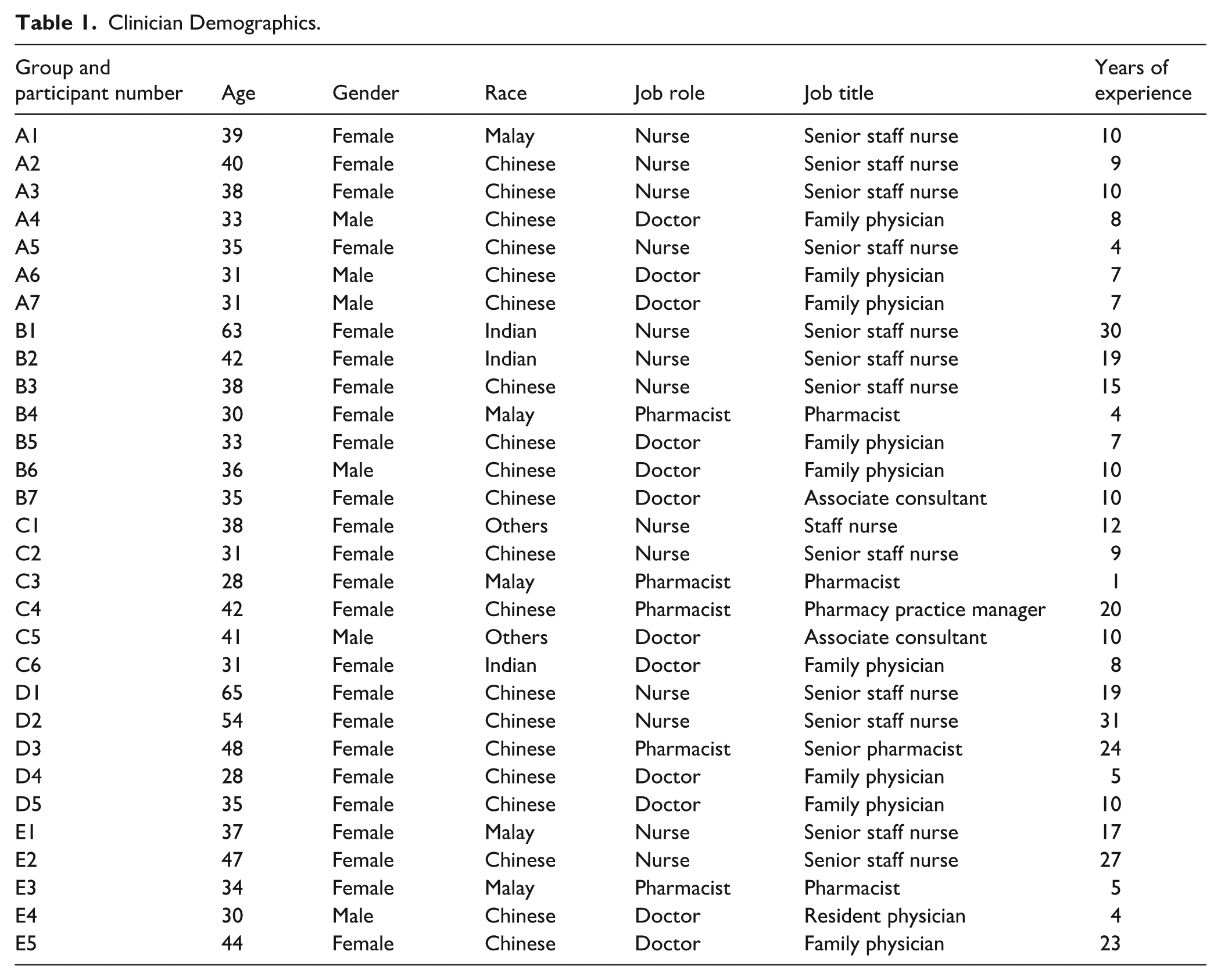
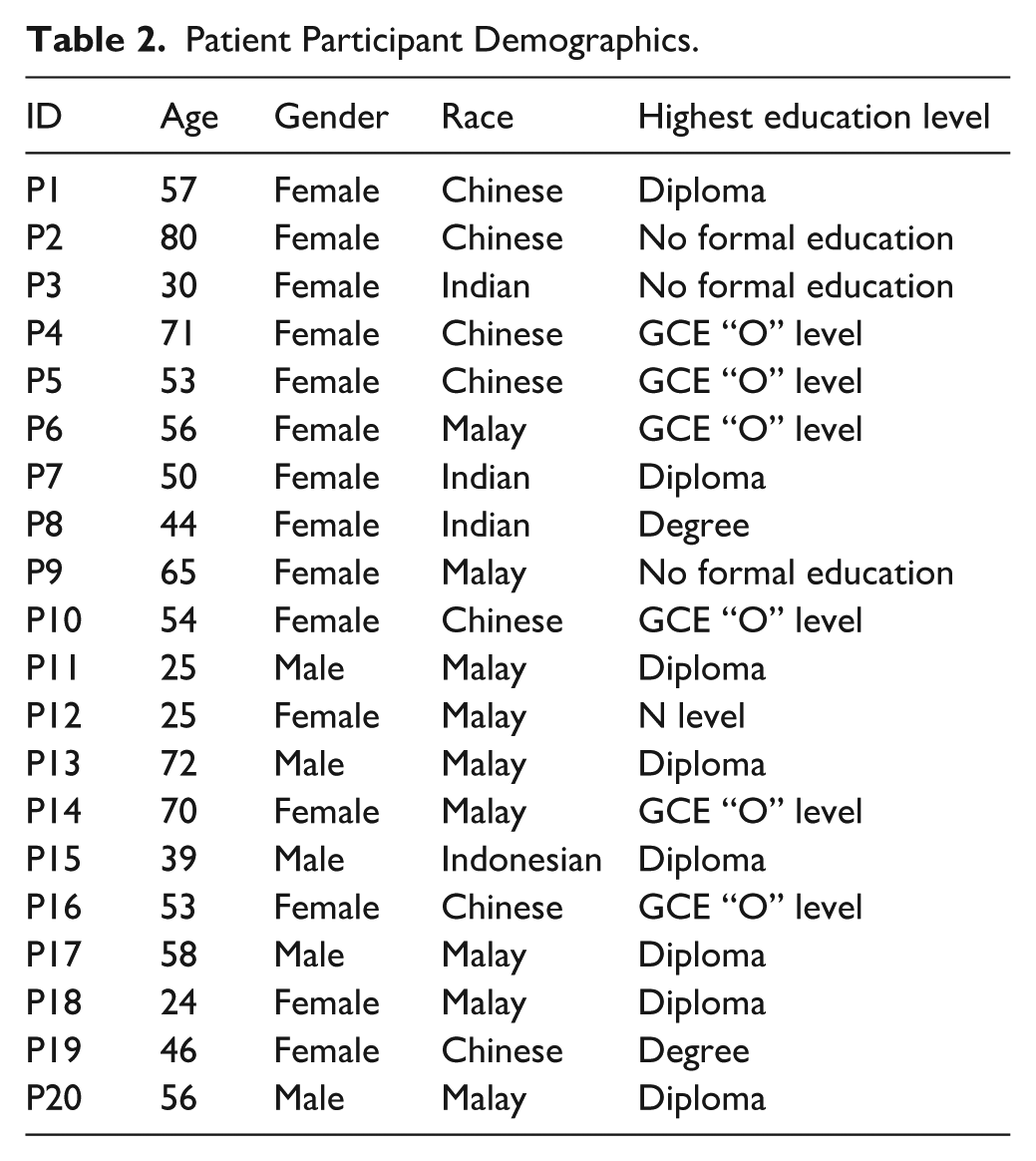
Thirty clinicians were recruited over 5 FGDs, with 12 doctors, 13 nurses, and 5 pharmacists with average experience of 12.5 years (range 1-31; Table 1). Each FGD lasted 40 to 50 min. Of the 20 patients, 15 were females, with a mean age of 51.4 years (range 24-80; Table 2). There were 7 Chinese, 9 Malays, 3 Indians and 1 Others, with education levels ranging from having no formal education to degree holders. Each individual interview lasted 15 to 30 min.
Clinician Demographics.
Patient Participant Demographics.
Both clinicians and patients provided insights to coherence, cognitive participation, and collective action. Reflexive actions were suggested by clinicians (Table 3).
Themes and Subthemes.
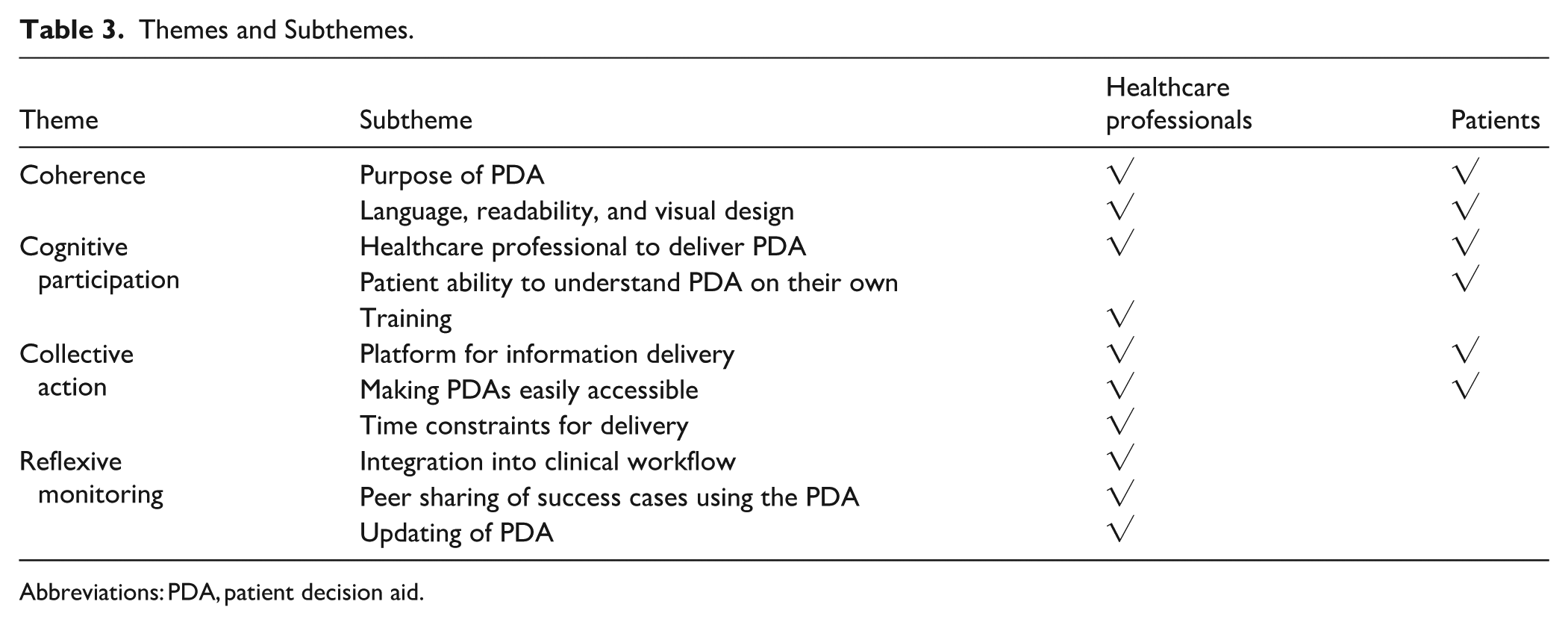
Abbreviations: PDA, patient decision aid.
Coherence
Both clinicians and patients described what they believed was the purpose of a PDA and commented on its visual design and languages.
Purpose of a PDA
Clinicians and patients viewed PDAs as an educational resource to enhance their understanding of their medical conditions. Patients focussed on their educational value, whilst clinicians saw them as a tool that could empower informed medical decision-making.
“In a way we empower them to make their decision” (Nurse A1, age 39) “I think in general it’s quite comprehensive. On top of providing information about what exactly is asthma and the types of medications available (. . .) it talks about the FAQ [Frequently Asked Questions] as well as talking about side effects, looking at what do I want to achieve as a patient.” (Patient P15, age 39)
Language, Readability, and Visual Design
Both clinicians and patients believed that the information in the PDA should be short and to the point, using simple language that those with basic education can understand. Clinicians specifically identified the need for optimisation of the PDA for black and white printing within the clinic during consultations, as their clinic printer did not have colours. However, patients emphasised the importance of colours and attractive cover pages to keep attention. Having larger font size sizes was important for seniors to read. Both clinicians and patients emphasised the need for multiple language options. Pictures could also be useful in helping patients understand the content.
“If you make it basic then someone with basic education up to secondary school level should then be able to understand.” (Patient P16, age 53, Chinese) I find that they are quite clear, quite good. They got colour for you to see more clearly, rather than all in black. Then, also most important thing the wordings are big because most of them especially seniors can’t see small print. (Patient P4, age 74, Chinese) “If it is multi-language, then it will be easier for [our] multi-racial society.” (Nurse C2, age 31) “As long as there are some pictures to you know? At a glance, you know what are the things that they want to convey.” (Doctor D5, age 35)
Cognitive Participation
Cognitive participation delved into the clinicians’ roles and training required to deliver the PDA, and patients’ ability to understand the PDA on their own.
Healthcare Professional to Deliver PDA
Although most patients can read the PDA on their own, many patients preferred a clinician to deliver the PDA. Majority of patients preferred the doctor to deliver the PDA as they perceived doctors to be most knowledgeable. However, they acknowledged doctors lacked the time to do so, and believed the nurse would be the next most appropriate person. A suggestion by some patients to mitigate this problem was to have a doctor initiate the PDA to emphasise its importance, followed by a nurse to explain the PDA. The pharmacists saw themselves as gatekeepers to identifying patients who are frequently requesting for reliever inhaler without using controller inhaler. However, they viewed themselves as having little role in sharing the PDA as medication decisions were finalised by doctors, followed by nurse patient education if required. Similarly, patients perceive the pharmacists’ to be too busy to provide education, or that their role was only to dispense their medication.
“If you don’t have time to go through the decision aid, then you might try to get the nurses help, especially for patients that don’t know how to read.” (Doctor E5, age 44)
Pharmacist only prescribe [dispense] the medicine. (Patient P10, age 54, Chinese)
Patient Ability to Understand PDA On Their Own
Many patients expressed their ability to comprehend the PDA on their own without explanation from a healthcare provider. However, they were concern that patients who have not received basic education would not be able to do so.
“I can understand (the PDA) myself because I’m a person who is educated. But if I were to give this to someone of the older age range, [they] definitely need help.” (Patient P15, age 39, Indonesian)
Training to Use the PDA
Clinicians had differing opinions regarding the need for training to use the PDA. A limited number believed that training is necessary to teach patients to use it on and how to address concerns, but majority placed more emphasis on the need to advertise the existence of the PDA. Most common suggestions included a short introduction session held during pre-existing staff meetings on what it is, who to use it for, and concerns to address.
“Not so much of training but maybe telling them, “Okay, like how to use” (Doctor C5, age 41)
Collective Action
Collective action looked at the platform for information delivery, steps in making the PDA easily accessibility to clinicians, and their concerns with time constrains using the PDA.
Platform for Information Delivery
Multiple forms of media were suggested, including physical or digital information pamphlets through utilisation of QR codes and videos. Majority of patients and clinicians found the hard copy format easier to use in the healthcare setting. Some clinicians suggested using softcopy options as the hardcopy paper could go missing over time. Participants highlighted that the younger patients might appreciate digital format and/or using interactive media, while older patients preferred physical forms. The video format could be played at the clinic television so that patients can watch while waiting to see the doctor. Patients who did not have asthma could also watch and share the information with their family members or friends who were living with asthma.
“Pamphlets will work especially for older folks, then I think the QR [is] for younger people.” (Pharmacist D3, age 48) “Oh, during consult, paper form. Ya, like before or after BP [Blood Pressure], after height and weight taken, they let you read in paper. (Patient P8, age 44, Indian) “[Clinic] Tv~ [television] advertisement. Because they got nothing to do, right? They are watching. They have their friends, relatives and all that. They can bring home this message.” (Nurse B1, age 63)
Making PDAs easily accessible Healthcare professionals emphasised the importance of making the PDAs accessible in clinical settings. They expressed a preference for having physical copies readily available in consultation rooms to eliminate time spent retrieving digital versions. However, this approach would require regular stock maintenance. If digital formats were implemented, clinicians stressed the need for a well-organised shared folder system with easy search functionality to ensure quick retrieval during consultations.
“As long as it’s readily available, we know where to find it whether is it softcopy or Infopedia [company’s information storage place], or whether is it available in the consult rooms, [so] when we see suitable patients then we can use it.” (Doctor B5, age 33)
Time Constraints for Delivery
Clinicians frequently cited time pressure as a major obstacle, noting the difficulty of incorporating detailed PDA discussions within brief consultation windows. To address this constraint, several practical solutions were proposed, including breaking down the delivery of PDA into sections, providing the PDA to patients for pre-consultation review, or using it as a post-consultation reinforcement tool.
“It’s time consuming. I think to go through the whole decision aid, [it is] probably a bit difficult. But I think if you want to focus on certain sections then it’s still okay.” (Doctor E4, age 30)
Reflexive Monitoring
This theme covers elements that will facilitate continued use of PDAs. Subthemes include methods of incorporation into workflow, peer sharing and positive review, and updating of the PDA.
Integration Into Clinical Workflow
Some clinicians suggested making PDAs part of the clinical workflow in the computer system for the specific target patient type, in this case asthma patients, to allow all patients to be given the PDA that is relevant to their specific issue.
“It probably has to be incorporated into the system or like the patient journey. Especially for asthma patients, I think there are a few ways that they very commonly present to us. Whether it’s an exacerbation needing rescue or like routine follow-up with a high GINA score pick-up at the HMS [Health Monitoring System]. Maybe in some of those points, it can be a like very routine - they will straightaway be given [the PDA].” (Doctor B7, age 35)
Peer Sharing of Success Cases Using the PDA
Many clinicians stated that having positive anecdotal experience shared from colleagues regarding successful instances at using the PDA would be key in increasing usage rates among clinicians, as well as to provide insight to others on how to better use the PDA through these instances where it was effective.
“If we have heard from maybe peers or other colleagues that they have successful counselled a patient using this patient decision aid, maybe that will help us as well. They say, “Oh, you know based on (. . .) after I used this patient decision aid, actually I find that a lot of my patients converted [to using a preventer].” (. . .) Previous success stories.” (Doctor B5, age 33)
Updating of PDA
Some clinicians identified the importance of being able to easily update the PDA regularly according to the latest clinical guidelines and feedback from patients, to maintain clinical relevance and improve usage.
“I think with any documents, we will need to have this up-keeping of documentations, in this case including the PDA [Patient decision aid], to make sure that they are relevant and still appropriate and safe for use.” (Pharmacist C4, age 42)
Discussion
This qualitative study aimed to explore the delivery method and facilitate continued use of a PDA to discuss use of preventive asthma inhaler. The application of Normalisation Process Theory provided a valuable theoretical framework for understanding the complex process of implementing the asthma PDA in primary care. For coherence, the results demonstrated a need for the PDA to be provided in different formats, such as paper, digital, and video formats due to generational divide in platform preferences, with older patients favouring physical formats while younger patients preferred digital options. This finding emphasises the need for multi-modal and flexible delivery approaches that can be tailored to individual patient needs, which was echoed in the literature. 21 Nonetheless all participants agreed that the PDA should be written in layman’s language, have large font sizes, and good visual design.
A variance in patients’ ability to understand PDAs independently was observed, with some patients expressing that they can read it on their own, while others require explanation. The choice of clinician for PDA administration was explored. Patients expressed a preference for doctors to explain the PDA, which aligned with findings from a Malaysian study. 8 In our setting, the doctors indicated that they do not have time to go through the entire PDA and could at most only discuss one section of the PDA. The doctors believed that the nurses should take on the role of going through the PDA with the patient if required. A possible solution is for the doctor to introduce the PDA to the patient, then refer them to a nurse who can review the PDA in detail, an approach that has been implemented in some clinical settings. 22 In some countries, pharmacist play an integral part in providing education for patients with asthma. 2 In our local context, most patients perceived the pharmacists to be too busy to provide education, and that their role was in dispensing medicine only.
Collection action explored the accessibility and delivery platforms for the PDA, with time constraint cited as a major barrier that deterred the doctors from using the PDA. This aligns with current evidence in a systematic review, where usage of PDAs extended patient consultations by an average of 1.5 min. 4 The comprehensive nature of PDAs, which incorporate essential elements such as asthma background information, treatment options, and patient motivations, approach reflects the core principles of SDM yet creates practical implementation challenges through increased consultation timing. Similar findings have been reported in other chronic disease contexts, where clinicians expressed concerns about the feasibility of incorporating detailed decision support tools within standard consultation timeframes. 23 While patient motivation and treatment preferences are crucial components of SDM that can enhance medication adherence, the time-constrained nature of clinical consultations makes it challenging to fully utilise PDAs. To address this limitation, approaches such as having patients review PDAs before their consultation, nurse-led follow-up discussions using the PDA post-consultation, 23 or the use of decision coaches 24 can be considered. Additional solutions from the literature include implementing technology-enhanced delivery methods, such as tablet-based PDAs in waiting areas 25 or interactive online platforms that patients can access at home, allowing for self-paced engagement with decision support materials. 26
For reflexive monitoring, clinicians consistently emphasised that successful implementation experiences shared by colleagues could serve as powerful catalysts for wider adoption. This aligns with the diffusion of innovation theory, which identifies peer-to-peer communication as more influential than formal training or top-down mandates in changing clinical practice behaviours.27,28 Firstly, positive anecdotal experiences from colleagues could provide practical evidence of the PDA’s effectiveness, potentially overcoming initial scepticism. Secondly, peer sharing could offer valuable insights into practical implementation strategies, helping other clinicians navigate common challenges. This is known as “situated learning” that is often more contextually relevant than formal educational approaches. 29 While senior level-buy in has been recommended as a key strategy in the literature, the findings in our study acknowledged the difficulties in doing so due to them being accustomed to using their own practice. 16 In addition, the need for regular PDA updates emerged as a crucial factor for continued use. Clinicians emphasised that PDAs must remain aligned with current clinical guidelines and evolving healthcare practices to maintain their relevance and credibility. This reflects the dynamic nature of evidence-based medicine and the challenge of maintaining decision support tools as clinical guidelines evolve.
Implications for Policy and Research
PDAs should be offered in both digital and physical PDA formats to accommodate diverse patient preference. There should be particular attention to visual design such as large fonts, simple language, and pictures. Multiple language options should be provided to cater to the multi-lingual society. Policy frameworks should also clarify roles and responsibilities for PDA delivery across different healthcare professionals, recognising that whilst patients prefer physician involvement, time constraints necessitate task-sharing models where nurses take primary responsibility for PDA administration, with doctors providing initial endorsement.
Healthcare organisations should implement systematic approaches to PDA integration within clinical workflows, including dedicated time allocation for shared decision-making activities and consideration of pre-consultation or post-consultation PDA delivery models to address time constraints. Additionally, policies should establish mechanisms for regular PDA content updates to ensure alignment with current clinical guidelines and maintain clinical relevance over time.
Future research should examine the effectiveness of asthma PDAs in discussing ICS treatment and their impact on asthma control and patient outcomes. Studies should investigate optimal delivery timing within clinical consultations, comparing pre-consultation patient review versus post-consultation nurse-led discussions to assess effects on both patient outcomes and healthcare efficiency. Implementation research should evaluate the feasibility and effectiveness of PDA integration in real-world clinical settings.
Strengths and Limitations
The strength of the study is the use NPT as the theoretical approach, which provided a comprehensive framework to understand implementation factors. Second, the study included diverse perspectives from multiple stakeholder groups - doctors, nurses, pharmacists, and patients - providing a holistic view of PDA implementation. The limitation of the study is the recruitment of English-speaking only, potentially missing important perspectives from non-English speaking patients who may have different needs and preferences for PDA delivery. Also, the study focussed on patients already using ICS, potentially missing perspectives from newly diagnosed asthma patients who might have different informational needs.
Conclusion
PDAs should be available in print copies or access to its digital form readily available to cater to different patient populations. Time constraints in clinical consultations present a significant barrier to PDA implementation. Alternative delivery approaches, including allowing patients to review the PDA prior to clinical consultation, nurse-led follow-up sessions, and decision coach support, are possible solutions to overcome the limitation. Peer sharing of successful PDA implementation experiences emerged as a key driver for wider adoption among clinicians. The use of PDA requires regular review among clinicians to update its content to ensure its relevance to current clinical practice.
Footnotes
Appendix
Interview Guide for Patients Based on the Normalization Process Theory (NPT).
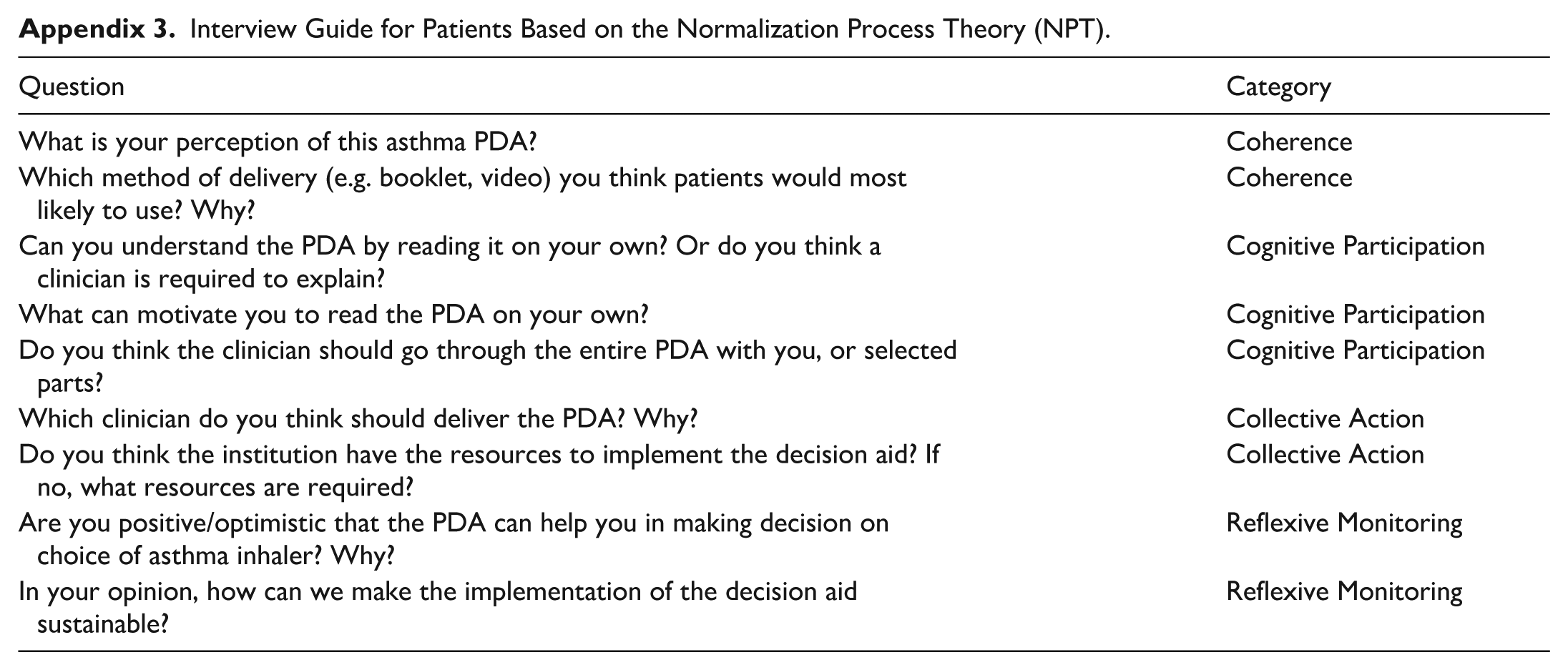
| Question | Category |
|---|---|
| What is your perception of this asthma PDA? | Coherence |
| Which method of delivery (e.g. booklet, video) you think patients would most likely to use? Why? | Coherence |
| Can you understand the PDA by reading it on your own? Or do you think a clinician is required to explain? | Cognitive Participation |
| What can motivate you to read the PDA on your own? | Cognitive Participation |
| Do you think the clinician should go through the entire PDA with you, or selected parts? | Cognitive Participation |
| Which clinician do you think should deliver the PDA? Why? | Collective Action |
| Do you think the institution have the resources to implement the decision aid? If no, what resources are required? | Collective Action |
| Are you positive/optimistic that the PDA can help you in making decision on choice of asthma inhaler? Why? | Reflexive Monitoring |
| In your opinion, how can we make the implementation of the decision aid sustainable? | Reflexive Monitoring |
Acknowledgements
The study team would like to thank Mr. Fei Yang Tan for assisting with recruitment of participants.
ORCID iDs
Ethical Considerations
Ethics approval was obtained from the Centralised Institutional Review Board (CIRB; reference: 2023/2635), with informed consent from participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by SingHealth Polyclinics Centre Grant (SHPCG-RSF23-02). The publication cost was supported by SingHealth Polyclinics – Centre Grant (CG21APR3006 (NMRC/CG3/001/2022-SHP)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data is available upon request.