
Abstract
Objective:
Digital health literacy (DHL) is a critical component for the effective self-management and secondary prevention of hypertension. However, the multi-level determinants of DHL in community settings are not yet fully understood. This study aimed to assess the status of DHL and identify its key sociodemographic, psychosocial, and health system determinants among adults with hypertension in China.
Methods:
A cross-sectional survey was conducted (October 2024-January 2025) across 1 tertiary general hospital and 3 community health service centers in Changzhou, China. Data were collected from 660 hypertensive adults using a structured questionnaire, including the eHealth Literacy Scale (eHEALS), and scales for physician-patient interaction, perceived internet health information quality, and perceived family support. Determinants were analyzed using multivariate logistic regression and a random forest model to rank factor importance.
Results:
Nearly half of the participants (49.45%) demonstrated low DHL. Multivariate logistic regression indicated that older age (specifically ≥75 years: OR = 13.33, 95% CI = 1.73-99.88), limited internet use (<1 h/day: OR = 2.50, 95% CI = 1.04-5.88), and concerns regarding data privacy (OR = 3.42, 95% CI = 1.01-11.58) were significant predictors of low DHL. Additionally, higher perceived quality of internet health information (OR = 0.72, 95% CI = 0.67-0.78), better physician-patient interaction (OR = 0.92, 95% CI = 0.86-0.99), and greater family support (OR = 0.37, 95% CI = 0.25-0.55) were associated with lower odds of low DHL. The random forest model identified the perceived quality of internet health information as the most influential predictor, followed by age and data privacy.
Conclusion:
DHL levels among individuals with hypertension in the community are suboptimal. These findings highlight the potential importance of a multilevel approach to supporting DHL. Efforts to improve the perceived quality of internet health information and strengthen social support systems may be beneficial, and primary care providers could play an important role in guiding patients’ use of digital health resources.
Keywords
Introduction
Digital health literacy (DHL) is essential for effectively accessing and using online health information, fostering positive health behaviors, and improving health outcomes. 1 Individuals with higher DHL are more likely to follow medical advice, adopt healthier behaviors, and manage chronic conditions effectively, thereby enhancing their quality of life.2,3 In contrast, those with lower DHL often rely on unreliable information sources, increasing their risk of exposure to misinformation and disinformation.1,4 Although improving DHL is widely recognized as a key strategy for promoting health equity, the potential of digital health tools remains underutilized due to persistent disparities in digital access and literacy levels. 1
For individuals with hypertension, digital health interventions have been shown to improve health behaviors and clinical outcomes, particularly among those with uncontrolled hypertension, while also enhancing adherence to self-management practices. 5 Evidence suggests that 71% of patients using digital tools achieved blood pressure control targets, compared with only 31% of those receiving standard care. 6 This substantial disparity underscores the potential of digital interventions in chronic disease management. However, the effectiveness of these services is highly dependent on patients’ DHL. 1 For individuals with lower DHL, the adoption of digital technologies may inadvertently widen the digital divide, further exacerbating health inequities. 7
Existing studies have found that DHL in individuals with hypertension is usually at a moderate to low level, 8 especially in China.9,10 To improve DHL, it is necessary to explore the formation mechanism of DHL. Existing studies have shown that DHL is affected by various socio-demographic factors, such as sex, age, place of residence, education level, income, marital status, retirement method, internet use, and medical insurance type.4,11,12 However, according to the World Health Organization’s Social Determinants of Health (SDH) framework, disparities in DHL are not solely driven by socioeconomic status. 13 Differences in material circumstance, behavioral factors, and psychosocial factors, as well as the accessibility of medical and health systems, may jointly contribute to the divide across populations. Among the material circumstance, data privacy and the quality of internet health information are considered to be important variables. Concerns about data privacy may hinder patients from actively seeking and sharing health information and participating in health management behaviors. 14
The quality of internet health information will affect individuals’ interest and confidence, which will further affect their information acquisition and health behaviors. 15 Among the behavioral factors, physician-patient interaction is considered to promote patients’ trust in and enthusiasm for using digital portals. 16 Among psychosocial factors, family support may be helpful for those with weak digital literacy,17,18 and accessibility to the health system affects the convenience of patients seeking online medical care. 19 Exploring these important environmental, behavioral, psychosocial, and health system factors can help identify factors that are more modifiable than sociodemographic factors and provide a theoretical basis for improving DHL. However, there is a lack of direct evidence showing that these important factors are directly associated with DHL in individuals with hypertension. The purpose of this study was to explore the important material circumstance, behavioral, psychosocial, and health system determinants of DHL based on the SDH theoretical framework to optimize the design of digital interventions.
Methods
Study Design and Participants
A cross-sectional descriptive study was conducted in a tertiary general hospital and 3 community health service centers in Changzhou, Jiangsu Province. Based on the sample distribution ratio between tertiary general and community hospitals, 396 participants were recruited from the tertiary general hospital and 264 from the community, for a total sample size of 660. Convenience sampling was used for the general hospital, while a multi-stage stratified sampling approach was applied for the community: districts and counties in Changzhou were first classified into high, medium, and low levels according to annual per capita GDP, followed by random selection of a district or county from each level, a street or town within each selected district or county, and finally a community within each street or town. Convenience sampling was then employed within each selected community.
Inclusion criteria were: (1) diagnosis of essential hypertension according to ICD-10 criteria, (2) disease duration >6 months, (3) age ≥18 years, and (4) prior experience using the internet or social media. For community-dwelling patients, an additional requirement was residence in the community for ≥6 months without tertiary hospital visits for hypertension in the past 3 months. Exclusion criteria included: (1) mental or cognitive impairment, (2) blood pressure >180/120 mmHg, 20 (3) illiteracy or dyslexia, (4) hearing or mobility impairments, and (5) severe cardiovascular or other comorbid conditions that could affect hypertension treatment and management (eg, stage IV heart failure, renal failure, liver dysfunction, or malignancy). The participant selection process is illustrated in Figure 1.
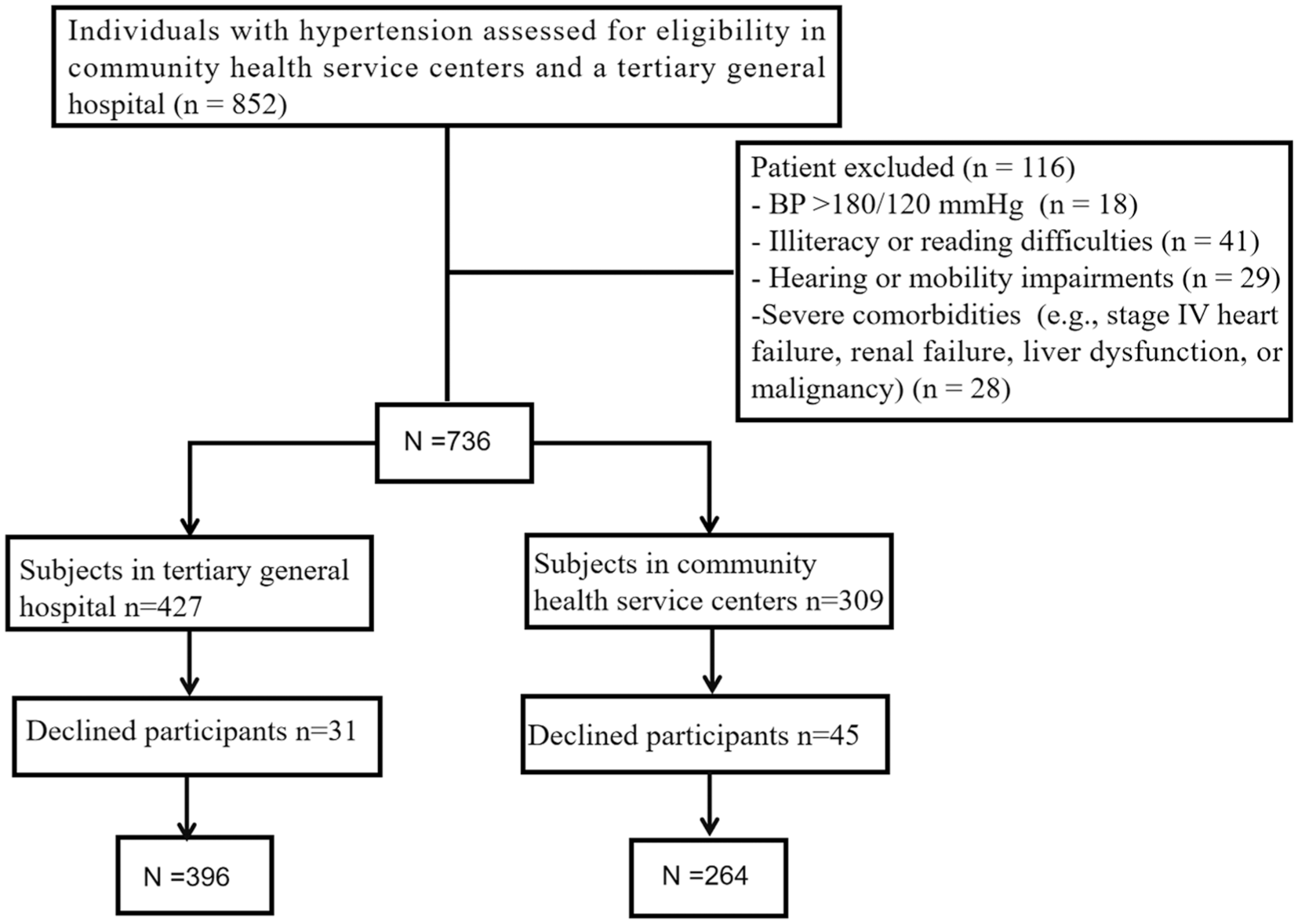
Flow diagram of participant selection.
Using G*Power 3.1, the required sample size for a multivariate binary logistic regression (OR = 1.43, 21 α = .05, power = 0.80, R2 = .10) was calculated as 596 participants. Allowing for a 10% loss to follow-up, a total of 660 participants are required. The questionnaire was administered in person using paper-based forms. After providing informed consent, participants voluntarily and anonymously completed the survey. Ethical approval for this study was obtained from the Human Research Ethics Committee.
Measures
The general information form collected data on sex (male, female), age, marital status (married, unmarried, non-married [non-single]), education (primary school or below, junior high school or above), residence (urban, rural), sample source (tertiary general hospitals, community health service centers), household annual income (less than 100 000; 100 000 or above), type of medical insurance (urban and rural employees’ health insurance, urban and rural residents’ health insurance, new rural cooperative medical insurance, other), data privacy (relatively safe or safe, unsafe or fair), and daily internet usage time (≤1 h; >1 h).
The eHealth Literacy Scale (eHEALS) developed by Norman and Skinner was used to measure the DHL. 22 eHEALS is the most widely used tool for assessing DHL. 23 eHEALS is a unidimensional scale with 8 items that assess the use of online health information and services, as well as judgment and decision-making abilities. Each item is rated on a 5-point scale (1 = strongly disagree; 5 = strongly agree), with higher scores indicating better DHL.
The Chinese version of eHEALS was translated and validated by Guo et al. 24 A standardized cross-cultural adaptation process was used, including forward translation, back translation, and comparison with the original English version, with appropriate adjustments for Chinese linguistic and cultural contexts. Exploratory factor analysis supported the construct validity of the scale, with the extracted factors explaining 62.38% of the total variance. In the present study, the eHEALS demonstrated good internal consistency (Cronbach’s α = .853). Consistent with previous research, a total score below 26 was defined as indicating low DHL.25,26
Questionnaire on quality of physician-patient interaction (QQPPI) was used to evaluate the quality of physician-patient interaction. 27 It is a unidimensional scale consisting of 14 items rated on a 5-point scale (1 = “do not agree” to 5 = “fully agree”), with higher scores indicating better interaction. The Chinese version of the QQPPI was translated and validated through a 4-stage process: forward-backward translation, expert review, psychometric validation, and internal consistency assessment, and has demonstrated strong internal consistency (Cronbach’s α = .939), excellent content validity (SCV = 0.968), as well as good convergent validity and cross-rater invariance. 28 In the present study, the Chinese version of the QQPPI showed acceptable internal consistency reliability (Cronbach’s α = .827).
Quality of Internet Health Information Questionnaire (QIHIQ) was used to assess the perceived quality of internet health information. 29 It comprises 4 dimensions: information quality relevance, information quality understanding, information quality adequacy, and information quality utility. Responses are rated on a 5-point scale (1 = “strongly disagree” to 5 = “strongly agree”), with higher scores indicating better perceived quality. The QIHIQ was translated into Chinese by Lu et al 30 using a forward-backward translation approach, and the psychometric properties of the Chinese version were subsequently evaluated. Confirmatory factor analysis demonstrated good convergent validity, with a composite reliability (CR) of .947 and an average variance extracted (AVE) of 0.535. In the present study, the Chinese version of the QIHIQ showed excellent internal consistency reliability (Cronbach’s α = .988).
The Perceived Social Support from Families Scale (PSS-Fa) was employed to assess family support in this study. 31 The Chinese version of the PSS-Fa consists of 15 items, with responses recorded as “yes” or “no,” where “yes” is scored 1 point and “no” 0 points. Higher scores indicate greater perceived family support. The scale was translated and culturally adapted using forward-backward translation, expert review, and pre-testing. 32 In the present study, the PSS-Fa demonstrated good internal consistency reliability, as assessed by the Kuder-Richardson Formula 21 (KR-21 = 0.909).
The Access to Health Care Questionnaire (PAHCQ) was used to evaluate accessibility to the healthcare system. 19 The PAHCQ comprises 5 dimensions: accessibility, accommodation, availability, acceptability, and affordability. The Chinese version of the PAHCQ consists of 30 items rated on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree,” with higher scores indicating better healthcare accessibility.
The questionnaire was translated into Chinese using the Brislin back-translation method and validated in a sample of 591 patients with cardiovascular diseases. 33 Construct validity was supported by acceptable model fit indices (χ2/df = 2.39, GFI = 0.92, AGFI = 0.91, RFI = 0.94). The original validation study demonstrated excellent internal consistency (Cronbach’s α = .960) and good split-half reliability (Guttman coefficient = .803). In the present study, the PAHCQ showed good internal consistency reliability (Cronbach’s α = .856).
Statistical Analysis
To mitigate potential selection bias arising from convenience sampling, post-stratification weighting was applied to adjust the sample distribution. Specifically, weights were calculated using sex, age group, and region as calibration variables, based on the demographic distribution reported in the China Hypertension Survey. 34 Weights were generated using an iterative proportional fitting (raking) procedure in SPSS and applied to all descriptive and regression analyses. First, descriptive analyses were conducted on all data related to DHL and its influencing factors. Next, chi-square tests were conducted to compare the incidence of low DHL across different sociodemographic groups. Univariate logistic regression analyses were used to examine the associations between internet quality of health information, physician-patient interaction, family support, healthcare accessibility, and DHL among individuals with hypertension. Subsequently, a multivariate binary logistic regression model was employed to identify key factors influencing DHL, with effect sizes expressed as odds ratios (ORs). Prior to multivariable regression analysis, variance inflation factors (VIFs) were used to assess multicollinearity among independent variables. A VIF value below 5 was considered indicative of no significant multicollinearity. Finally, a random forest model was used to determine the most important factors contributing to DHL. All analyses were performed using SPSS 25.0 and R version 4.1.2, with 2-sided tests and a significance level of α = .05.
Results
The mean total DHL score among the 660 participants was 24.19 (SD = 8.27). Using 26 points as the cutoff, 49.55% of participants were classified as having low DHL, and 50.45% as high DHL. Table 1 presents the associations between sociodemographic characteristics and DHL. The mean age was 54.17 years (SD = 14.67), and the risk of low DHL increased progressively with age. Individuals with primary school education or below had a higher probability of low DHL (86.83%) compared to those with junior school education or above (27.81%; χ2 = 213.89, P < .001).
Analysis of DHL Across Sociodemographic Groups.
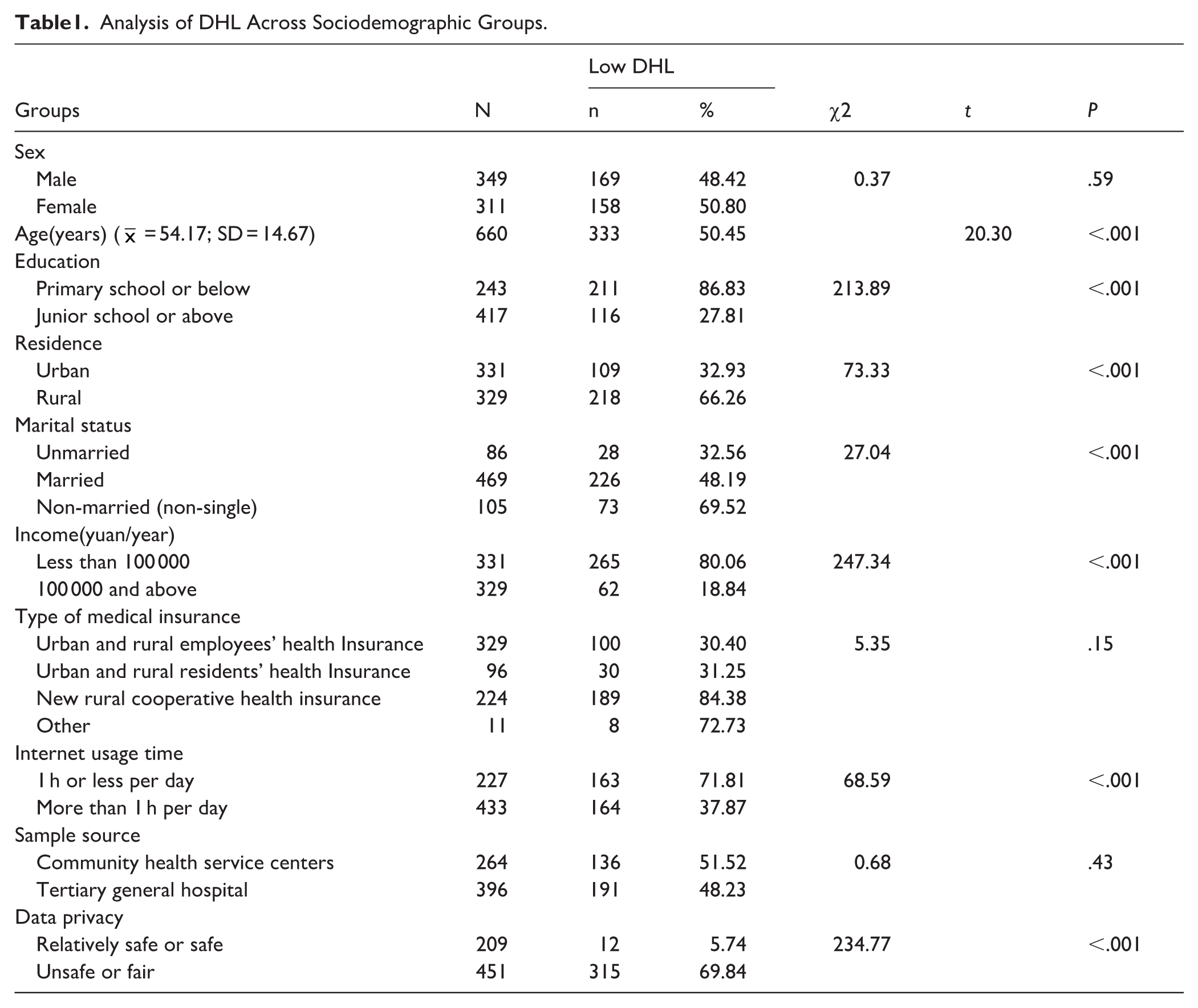
Rural residents (66.3%) were more likely to exhibit low DHL than urban residents (32.93%; χ2 = 73.33, P < .001). Unmarried participants had a significantly lower proportion of low DHL compared with married and non-married (non-single) individuals (χ2 = 27.04, P < .001). Participants with household annual incomes below 100 000 RMB had a higher prevalence of low DHL (80.06%) than those with incomes ≥100 000 RMB (18.84%; χ2 = 247.34, P < .001). Additionally, individuals spending 1 h or less per day (χ2 = 68.59, P < .001) or perceiving data privacy as unsafe or fair(χ2 = 234.77, P < .001) were more likely to have low DHL. However, DHL was not significantly associated with participants’ sex, sample source, or type of medical insurance (all P > .05).
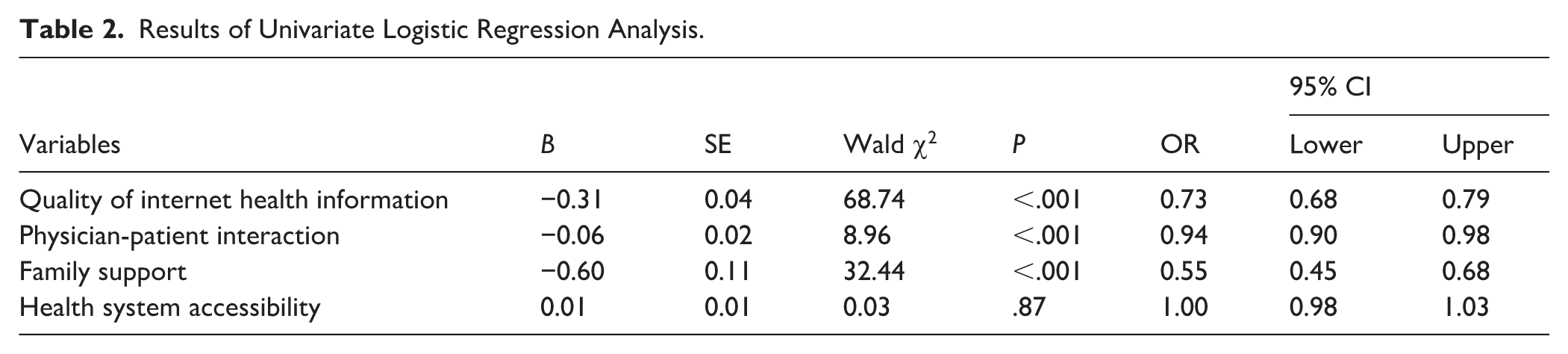
Univariate logistic regression analysis showed that among individuals with hypertension, higher perceived quality of internet health information was associated with an decreased risk of low DHL (OR = 0.73, 95% CI = 0.68-0.79). Similarly, better physician-patient interaction was linked to a lower risk of low DHL (OR = 0.94, 95% CI = 0.90-0.98), and greater family support was also associated with decreased risk (OR = 0.55, 95% CI = 0.45-0.68). Health system accessibility was not significantly associated with low DHL (OR = 1.00, 95% CI = 0.98-1.03), as shown in Table 2.
Results of Univariate Logistic Regression Analysis.
Multivariate logistic regression was conducted to identify independent predictors of low DHL among hypertensive individuals (Table 3). All variables had VIFs below 5, suggesting that multicollinearity was not a concern. After adjusting for confounding variables, 6 variables, age, data privacy, internet use time, quality of internet health information, physician-patient interaction, and family support emerged as significant independent predictors of low DHL. Compared with participants aged ≤44 years, those aged 60 to 74 and ≥75 years showed significantly higher odds of low DHL, with ORs of 3.61 (95% CI = 1.10-11.83) and 13.33 (95% CI = 1.73-99.88), respectively. No significant difference was observed between the 45 and 59 age group and the ≤44 age group. Participants spending 1 h or less online daily had significantly higher odds of low DHL compared with those spending more than 1 h online (OR = 2.50, 95% CI = 1.04-5.88). Similarly, participants who perceived data privacy as unsafe or fair had a 3.42-fold risk of low DHL compared with those who perceived it as relatively safe or safe (95% CI = 1.01-11.58). In contrast, higher perceived quality of internet health information, better physician-patient interaction, and greater family support were associated with lower odds of low DHL, with ORs of 0.72 (95% CI = 0.67-0.78), 0.92 (95% CI = 0.86-0.99), and 0.37 (95% CI = 0.25-0.55), respectively.
Multivariate Logistic Regression Analysis of Low DHL in Individuals With Hypertension.
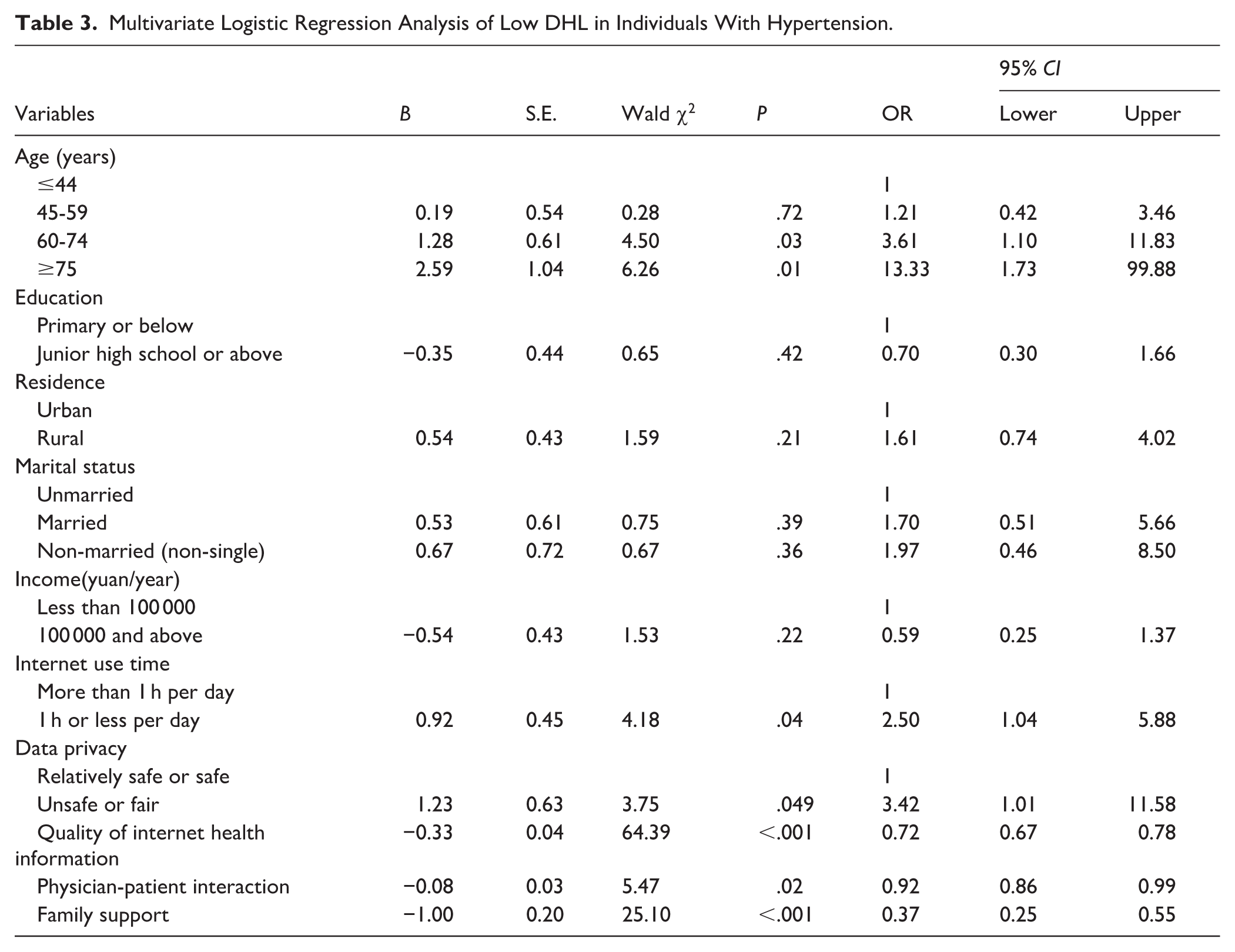
In contrast, education, residence, marital status, income, and health system accessibility were not significant predictors in the multivariate model. The model demonstrated good fit, with a Nagelkerke R2 of .64, indicating that the included predictors collectively provide strong discrimination between participants with low and high DHL.
Variable importance was ranked based on the mean decrease in Gini index, with higher values indicating a greater contribution of each variable to classification performance in distinguishing between low and high DHL. The dataset was randomly divided into training (n = 462) and testing (n = 198) sets. Random forest hyperparameters were tuned using grid search with cross-validation, yielding optimal values of ntree = 500 and mtry = 2.
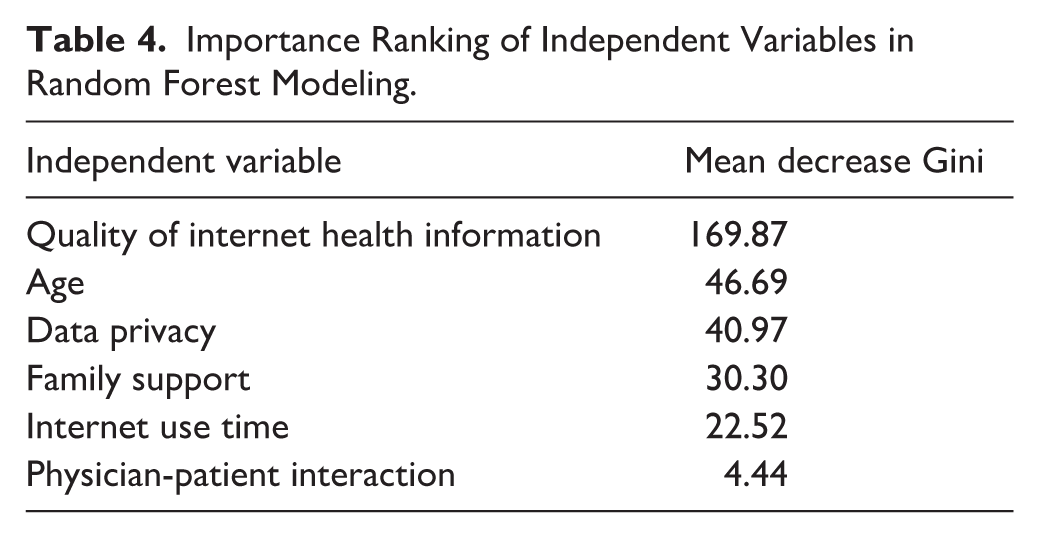
The results showed that the quality of internet health information was the most important variable in classifying low DHL, followed by age, data privacy, family support, internet use time, and physician-patient interaction (Table 4; Figure 2).
Importance Ranking of Independent Variables in Random Forest Modeling.
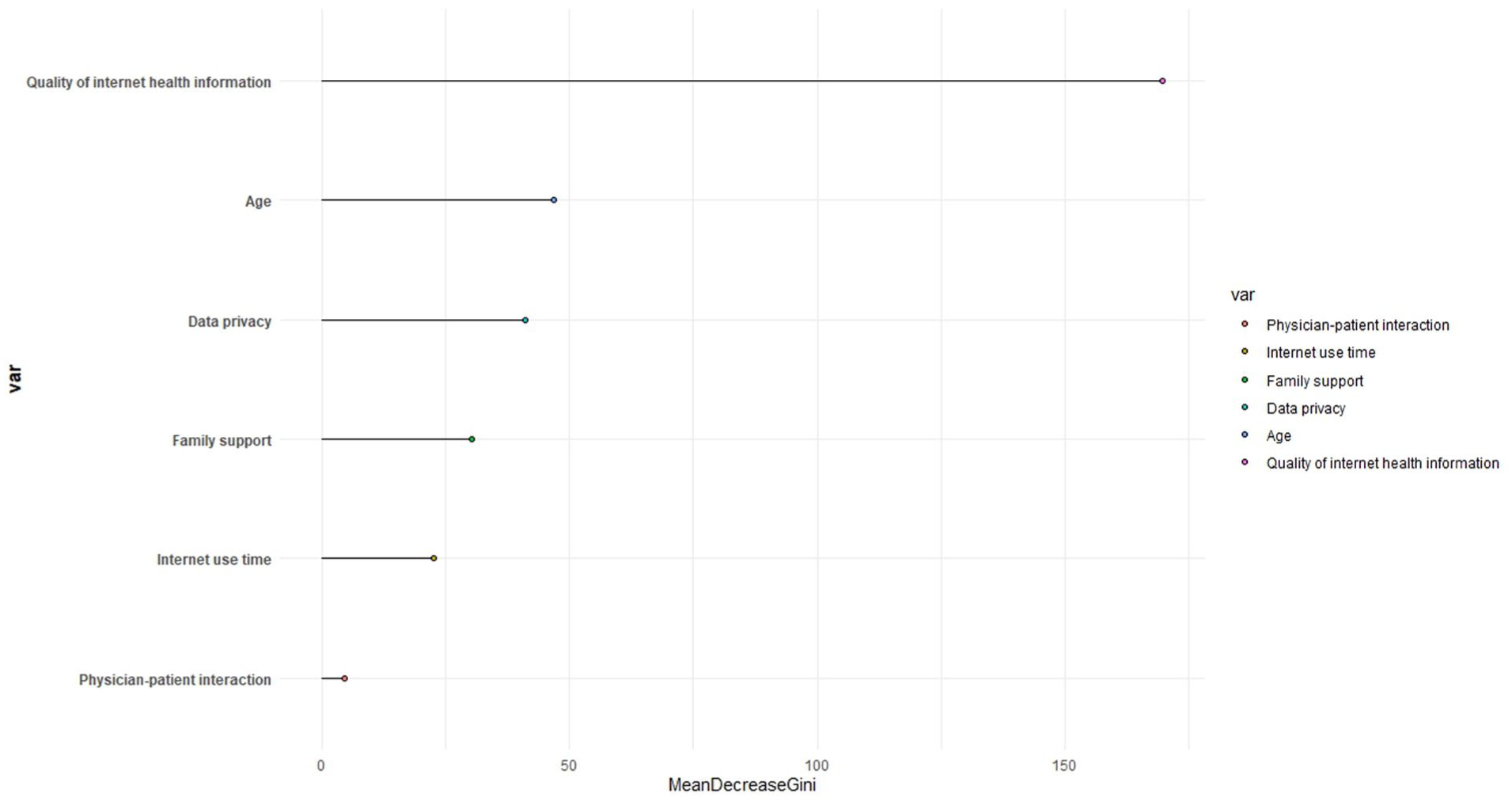
The importance analysis based on the random forest model.
Discussion
This study employed the WHO’s SDH framework as its theoretical foundation to explore the impact of socioeconomic factors, material circumstance, behavioral, psychosocial, and health system factors on DHL among individuals with hypertension. The study found that DHL of individuals with hypertension in China is at a moderately low level.8-10 Participants showed difficulties in finding and evaluating online information. Socioeconomic factors such as age, education, residence, income, and marital status were associated with variations in DHL. However, after controlling for confounding variables, only age remained a significant predictor of DHL. This aligns with findings from numerous existing studies,11,35,36 suggesting that DHL interventions should prioritize individuals aged 60 years and above, particularly those aged 75 years and older who constitute a high-risk group.
The study also identified other potential factors: low quality internet health information, concerns about data privacy, poor family support, poor physician-patient interactions, and limited internet use time place patients at a disadvantage in enhancing their DHL. Among all influencing factors, the quality of internet health information exerted the strongest impact on patients’ DHL, emerging as the most significant determinant. Social Cognitive Theory posits a dynamic interaction between individual behavior, personal factors, and environmental factors. High quality internet health information, as a material environmental factor, not only influences users’ trust in and willingness to use the information,15,18 but may also strengthen individuals’ self-efficacy in evaluating online health information, thereby creating a positive feedback loop that ultimately improves patients’ DHL.
Data privacy, as a important material circumstance factor, has attracted increasing attention in recent years. Public trust in medical institutions’ privacy protections and concerns regarding access to online health data can influence individuals’ willingness to engage with and use digital health services.37,38 In the context of participatory medicine and widespread social media use, privacy concerns may further discourage patients from actively seeking or sharing health information, 14 thereby impacting their DHL.
Previous research has shown that the use of digital health tools can affect physician-patient interactions. 39 Our study suggests that patients’ DHL may also be influenced by physician-patient interactions. First, physicians remain the most trusted source of health information and play a crucial role in helping patients interpret online health content. 29 Second, doctors can guide patients on the appropriate use of digital tools 40 and provide support when difficulties arise. 41 These findings indicate that physician-patient interaction, as a behavioral factor, may influence patients’ DHL through multiple pathways.
Family support, as a psychosocial factor, can empower populations with low digital literacy, particularly the elderly. Older adults may access health portals and utilize digital health tools with the assistance of family members,17,18 who can also serve as intermediaries to interpret and explain online health information when needed. 42 Such support may contribute to improved DHL.
While previous studies have shown that health system accessibility is associated with the use of health portals, 43 it did not emerge as an independent predictor of DHL in this study. After controlling for socioeconomic variables such as income and place of residence, its independent contribution was no longer evident, which may reflect overlapping effects with these factors. In addition, this study primarily assessed healthcare accessibility in terms of convenience of care, and did not fully capture dimensions more directly related to DHL, such as the availability of digital services and information support. Future research could further refine the dimensions of accessibility to better elucidate its mechanisms. Furthermore, sociodemographic characteristics, such as sex, occupation, type of health insurance, and sample source were not significant predictors of DHL, reinforcing prior findings that the influence of sociodemographic factors on DHL is inconsistent. 4
Strengths and Limitations
One of the major strengths of this study is that, guided by the SDH model, we identified representative variables beyond sociodemographic factors, including material circumstances, behavioral and psychosocial factors, and health system characteristics that influence DHL in individuals with hypertension, which is relatively rare in previous studies. Moreover, using random forest modeling, we identified one of the most influential variables, the quality of internet health information, which has received little attention in prior research. These findings provide a foundation for optimizing interventions to improve DHL among individuals with hypertension.
Nevertheless, several limitations should be acknowledged. First, part of the sample was obtained through convenience sampling in a tertiary hospital. Although post-stratification weighting was used to improve the sample structure, this approach may still have introduced selection bias, potentially underrepresenting individuals with more pronounced digital divides and affecting the estimation of overall DHL levels and related factors. Second, the sample was drawn from a city in eastern China, and the generalizability of the study’s conclusions to other regions (especially those with relatively limited healthcare resources) should be interpreted with caution. Third, due to the cross-sectional study design, this study is limited in its ability to support causal interpretation. Finally, although this study was guided by a social determinant model, the number of included variables remains relatively limited. Future research could explore additional potential determinants to achieve a more comprehensive understanding of the mechanisms influencing DHL.
Implications and Suggestions
This study found that the DHL of individuals with hypertension is influenced by factors such as age, quality of internet health information, data privacy, family support, physician-patient interaction, and internet use time, indicating that DHL varies across different populations. Elderly patients and those who spend less time online tend to have lower DHL, highlighting the need to consider patient characteristics and accessibility differences when designing digital health tools or interventions. For these populations, healthcare providers are encouraged to recommend digital health tools with simple interfaces and clear step-by-step instructions during community or outpatient follow-up visits, accompanied by brief demonstrations to facilitate mastery of basic functions. At the same time, patients should be guided to prioritize high-value online activities, such as accessing authoritative health platforms and managing personal health data, while minimizing exposure to unverified or low-quality information.
Based on the SDH framework, this study found that the quality of internet health information has the most significant impact on DHL among individuals with hypertension. These findings suggest that healthcare providers should proactively recommend 1 or 2 authoritative health information sources during routine hypertension follow-ups and briefly explain how to evaluate credibility, such as by checking publication dates, author credentials, and other relevant criteria, to help patients strengthen their ability to screen and appraise health information. In addition, digital health platforms should establish standardized information evaluation criteria and enhance transparency regarding potential conflicts of interest to improve the reliability of health information, 44 while strengthened government oversight and professional review mechanisms may further help curb the spread of false health information online. 45
Regarding privacy protection, it is essential to strengthen legal safeguards and oversight mechanisms, 46 ensure that patients have control over their own data with clearly restricted access rights, 47 and prioritize the use of public platforms. 48 At the same time, in primary care settings, healthcare providers can briefly explain the platform’s data usage policies and privacy settings to enhance patients’ awareness of data security. Furthermore, integrating technology, education, and personalized interventions can help foster patient trust and engagement. 49
To maximize the role of physician-patient interaction in enhancing patients’ DHL, it is recommended to first improve healthcare professionals’ digital literacy. 50 Brief DHL assessments can be embedded into routine follow-ups, such as using 2 or 3 open-ended questions to understand how patients access and evaluate health information. This approach helps identify individuals who require additional support and enables the provision of targeted guidance. Finally, family members should actively participate in accessing, evaluating, and applying health information. This is particularly important for older patients with lower digital literacy, as family members can assist them in accessing and understanding online health information in daily life.
Conclusion
The study found that DHL of individuals with hypertension in China is at a moderately low level. In this study, we highlighted the predictive role of social determinants in shaping DHL among individuals with hypertension. Among the various influencing factors, the quality of internet health information emerged as the most critical determinant of DHL. Demographic and socioeconomic factors, particularly age, were significantly associated with DHL, with adults aged ≥60 years, and especially those aged ≥75 years, showing a higher likelihood of low DHL. Furthermore, concerns about data privacy, the level of family support, time spent online, and the quality of physician-patient interaction were found to significantly affect participants’ DHL. These findings indicate that enhancing DHL requires a comprehensive approach, involving not only the efforts of individual patients but also active engagement from healthcare providers, families, and broader societal support. Interventions should therefore focus on improving the accessibility and reliability of online health information, strengthening privacy protections, fostering supportive family environments, promoting effective physician-patient interaction, and encouraging appropriate use of digital tools. Such a multifaceted strategy can help bridge disparities in DHL and ultimately contribute to better self-management and health outcomes for individuals with hypertension.
Footnotes
Acknowledgements
We sincerely thank the Department of Cardiology at Changzhou Second People’s Hospital and the 3 community health service centers for their support in data collection, and we are grateful to all participants for their time and contributions.
Author Contributions
JL conducted the data analysis and drafted the manuscript. TT interpreted the data and provided critical revisions. AS and PMD contributed to revising the manuscript. All authors have read and approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.