
Abstract
Background
Hypertension is a major cardiovascular risk factor that is insufficiently controlled. Management, which is challenging due to the asymptomatic nature of the disease and limited patient awareness, depends on lifestyle factors, comorbidities, and health literacy. Self-measurement of blood pressure may improve blood pressure control and patient engagement, although evidence regarding the accuracy of these measurements remains limited. The aim of this study was to analyse the level of knowledge about hypertension and self-blood pressure measurement skills among individuals with this condition.
Methods
A descriptive cross-sectional observational study was conducted in Spain in 2025 in urban and rural primary care centres, including 151 patients aged over 18 years with diagnosed hypertension and preserved cognitive capacity. Sociodemographic, clinical, and blood pressure self-measurement data were collected. Knowledge about hypertension was assessed using the Hypertension Knowledge Questionnaire, which includes 15 items covering the disease, risk factors, treatment, and complications.
Results
Most participants were unaware of the diagnostic blood pressure threshold for hypertension, defined according to European guidelines as ≥ 140/90 mmHg, and 94% exhibited poor control of systolic blood pressure. Educational level was significantly associated with better knowledge of cardiovascular, renal, and cerebrovascular complications, as well as with more accurate self-blood pressure measurement practices. However, no association was observed between educational level and overall blood pressure control. Sex-based differences were identified, with better diastolic blood pressure control among women.
Conclusions
Higher educational level is associated with improved knowledge of hypertension and higher quality of self-blood pressure measurement, but not with better blood pressure control. The persistence of poor blood pressure control despite adequate knowledge and skills suggests that factors beyond education, particularly comorbidities such as chronic kidney disease and sociodemographic inequalities, may play a major role. Health education remains important to support self-management; however, it should be integrated within a broader, multifactorial and individualized approach to hypertension care in primary health care in the Spanish context.
Keywords
Introduction
Hypertension is one of the main modifiable risk factors associated with an increased risk of cardiovascular disease, stroke, and renal failure.1,2 However, blood pressure control among individuals with hypertension remains insufficient. 3 According to the World Health Organization (WHO), 4 only 23% of people with hypertension worldwide achieve adequate blood pressure control, leading to a significant increase in healthcare expenditure and greater exposure to complications and adverse events related to cardiovascular risk. 5
Hypertension management has evolved over time, with changes in diagnostic thresholds and treatment approaches influencing current clinical practice. Contemporary European and American guidelines emphasize cardiovascular risk-based management and strongly recommend out-of-office blood pressure measurement, including home blood pressure monitoring, as an essential component for diagnosis and follow-up6-8 Blood pressure control is influenced by multiple factors, including genetic determinants, the presence of comorbidities, lifestyle behaviours, and health literacy. These factors influence the ability of individuals to understand and manage health-related information and play a crucial role in active participation in health-related decision-making. 9
Self-measurement of blood pressure is a key tool in the monitoring and management of hypertension. It enables patients to obtain blood pressure readings outside the clinical setting, facilitate greater patient engagement in self-management, and provides values that are more representative of usual blood pressure levels.10,11 Several studies have reported that between 60% and 80% of individuals with hypertension own a home blood pressure monitoring device.12,13 However, there is limited evidence assessing the quality and accuracy of the measurements they make with these devices. 14
Emerging evidence suggests that a substantial proportion of patients perform home blood pressure monitoring incorrectly, which may lead to clinically relevant misclassification of blood pressure levels. 15 Current guidelines emphasize the importance of structured education and training programmes, as well as periodic assessment and validation of patients measurement technique by healthcare professionals.6,16 In this context, interventions incorporating direct observation of patients performing home blood pressure monitoring by trained professionals have been shown to improve measurement technique, increase reliability of readings, and contribute to better blood pressure control.17,18 However, despite this findings, the specific errors most commonly made by patients during home blood pressure monitoring remains insufficiently described in the literature.
Hypertension is often asymptomatic, which contributes to a low perception of risk among patients and hinders the adoption of behaviours aimed at blood pressure control. 19 Despite the clinical and epidemiological impact of this condition, few studies have focused on evaluating population knowledge regarding hypertension and the factors that determine its complications. Recent systematic reviews indicate that limited hypertension-related knowledge and low health literacy are associated with poorer adherence, worse self-management behaviors, and suboptimal blood pressure control.20,21 Educational and behavioral interventions aimed at improving patient knowledge have been shown to significantly improve clinical outcomes. 22 Insufficient knowledge about hypertension may be a key determinant affecting therapeutic adherence and the adoption of lifestyle modifications required to control blood pressure and prevent complications associated with sustained elevated blood pressure levels.
Definitions and management of hypertension have evolved over time, with differences between international guidelines (e.g., ≥140/90 mmHg in Europe vs. ≥130/80 mmHg in the United States), which can affect clinical interpretation and prevalence estimates.6-8 These differences reflect distinct but complementary approaches; however, both emphasize patient involvement, self-monitoring, and education as key elements in hypertension care. 23 Although hypertension has been widely studied, there is limited evidence on patients’ knowledge and their practical skills in self-measuring blood pressure in primary care. This gap is clinically important, as inadequate skills and low health literacy may contribute to poor blood pressure control. Addressing it is essential to improve outcomes.
The aim of this study was to assess the knowledge of hypertension and self-blood pressure measurement skills among individuals diagnosed with this condition.
Methods
Participants and Procedures
A descriptive, cross-sectional, multicentre study was conducted between September and December 2025 in 10 community care centres affiliated with two Primary Health Care Areas in Catalonia (Spain), encompassing both rural and urban settings. Participants were consecutively recruited from primary care registries, reflecting routine clinical practice and a population of older adults with multimorbidity typical of the Spanish primary care setting. A total of 150 individuals aged over 18 years with a diagnosis of hypertension and chronic kidney disease, who were Catalan or Spanish speakers, were included. Individuals with a score below 10 on the LOBO test, a Spanish-adapted and validated version of the Mini-Mental State Examination widely used to assess global cognitive function and screen for cognitive impairment in older adults, 24 and score below 2 on the Pfeiffer test, 25 and those receiving palliative care were excluded.
Nurses contacted eligible individuals by telephone based on clinical records from the two participating primary care areas to explain the study details and invite them to participate. Those who agreed were scheduled for an in-person visit by one of the four collaborating investigators at their reference health centre. During the call, participants were asked to bring their home blood pressure monitoring devices to the appointment. When they did not own one, a device was provided by the centre.
During the in-person visit, participants individually completed a self-administered questionnaire assessing their knowledge of hypertension in a quiet setting that ensured privacy and confidentiality. Subsequently, participants performed self-measurement of blood pressure while the investigator observed the procedure and recorded the results. The total duration of the visit was approximately 20 minutes. Clinical data were obtained from the participants’ electronic health records. To ensure anonymity, a numerical code that was known only to the principal investigator was assigned to the data collection forms.
Measures
Sociodemographic (age, sex), clinical (comorbidity, years since diagnosis, hospitalizations during the previous year), and self-blood pressure measurement–related variables (body position, cuff placement) were collected. Participants’ self-blood pressure measurement technique was assessed by direct observation following European Society of Hypertension recommendations. 6
Knowledge of hypertension was assessed using the Spanish adaptation of the Hypertension Knowledge Questionnaire. 26 This descriptive instrument consists of closed-ended questions (yes/no/don’t know) and is organized into nine sections. The first six sections assess knowledge regarding hypertension, risk factors, complications, diet, physical activity, and medication. The final three sections include independent variables such as social support, educational level, and employment status. In the present study, the questionnaire demonstrated good internal consistency, with a Cronbach’s alpha of 0.774, which is comparable to that reported in the original validation study. 26
Data Analysis
Data were analysed using SPSS version 27.0 (IBM Corp., Chicago, IL, USA). Quantitative variables were expressed as mean and standard deviation whereas categorical variables were described using absolute frequencies and the corresponding percentages. Associations between categorical variables were assessed using Pearson’s chi-square test.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Jordi Gol Research Ethics Committee (protocol code 25/226-P; approval date: September 3, 2025). The provisions of Organic Law 3/2018 on Data Protection and Guarantee of Digital Rights were respected. The ethical principles of the World Medical Association for medical research involving human subjects were followed. Prior to completing the questionnaire, all participants were informed about the study, received an information sheet, and provided written informed consent. Confidentiality was ensured through anonymization of the data collection forms.
Results
A total of 151 individuals, with a mean age of 73 years (SD 6.8), participated in the study. Of these, 54% were male and 46% female, most were retired (87%) and had been living with hypertension for over 10 years (75%). Regarding education, 35% had no formal education, 31% had primary education, 19% secondary, and 15% university education. Men were younger than women, with mean ages of 72.1 years (SD 7.28) and 74.1 years (SD 6.0), respectively. All participants had chronic kidney disease in addition to hypertension. Furthermore, 51% had heart disease, 41.7% had vascular disease, and 30.5% had diabetes mellitus.
Overall, 75.5% of participants owned a home blood pressure monitoring device. The mean systolic blood pressure was 153.6 mmHg, with 94% of patients exceeding the reference value (systolic blood pressure ≥140 mmHg). With regard to diastolic blood pressure, the mean value was 83 mmHg, with 15.2% of patients above the established threshold (diastolic blood pressure ≥90 mmHg). Men showed poorer diastolic blood pressure control compared with women (p = 0.040).
Adherence to Self-Blood Pressure Measurement Recommendations

Pearson’s chi-square test was used to assess associations between categorical variables.
Knowledge of Hypertension (n=151)
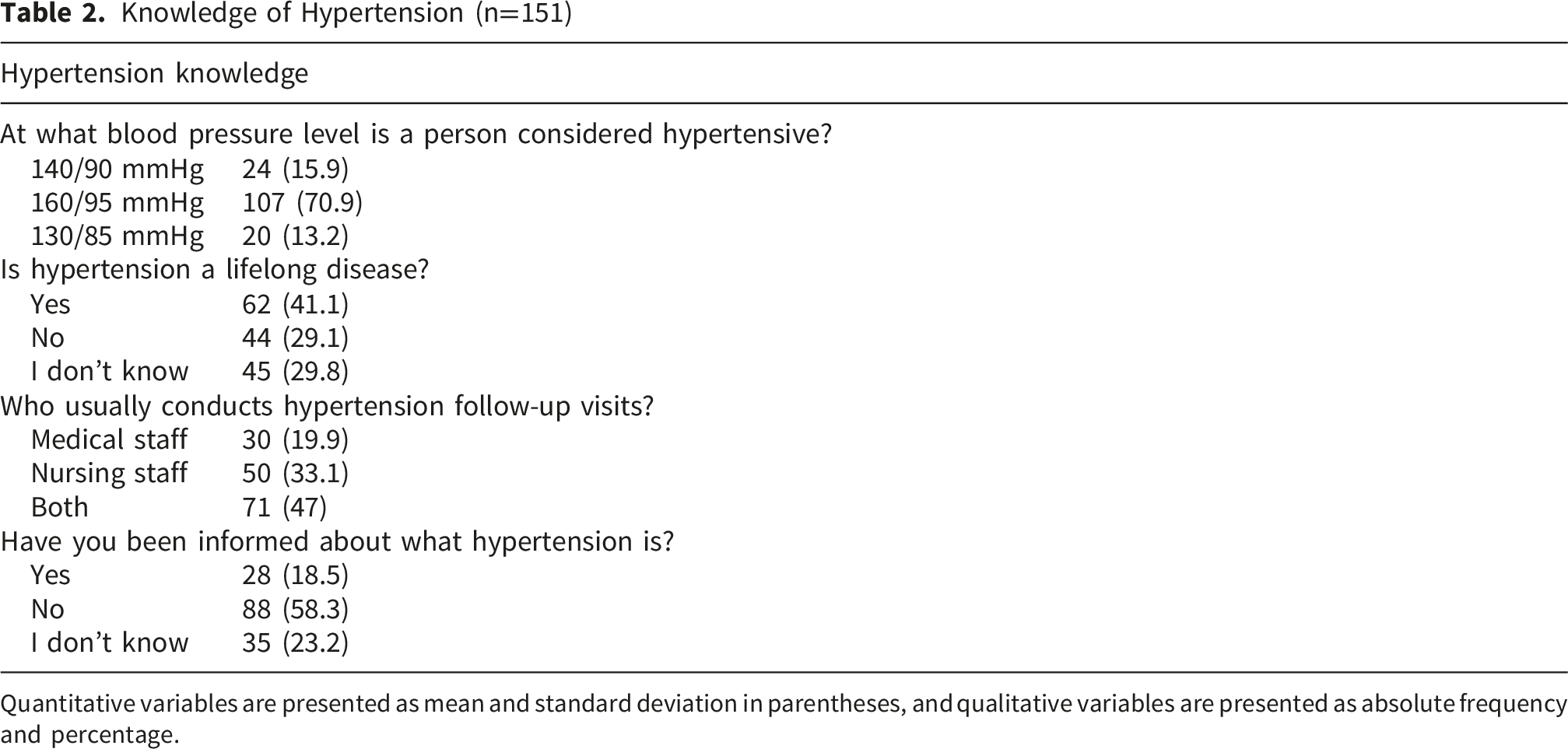
Quantitative variables are presented as mean and standard deviation in parentheses, and qualitative variables are presented as absolute frequency and percentage.
When comparing educational level with knowledge of both hypertension-related complications and lifestyle measures for its management, individuals with secondary education were significantly more aware that hypertension can cause eye problems (p = 0.003), heart disease (p < 0.001), cerebrovascular events (p < 0.001), and kidney damage (p = 0.004) compared with those with primary education.
With regard to habits and preventive measures, participants with secondary education more frequently recognized the benefits of a heart-healthy diet (p = 0.027), weight loss (p < 0.001), daily physical activity (p < 0.001), and maintaining a calm attitude toward life (p = 0.013). Additionally, individuals with secondary education were less likely to agree with the statement that hypertension can be controlled solely with medication (p < 0.001) and were less inclined to consider that treatment can be discontinued once blood pressure is controlled (p < 0.001).
Knowledge of Hypertension According to Educational Level
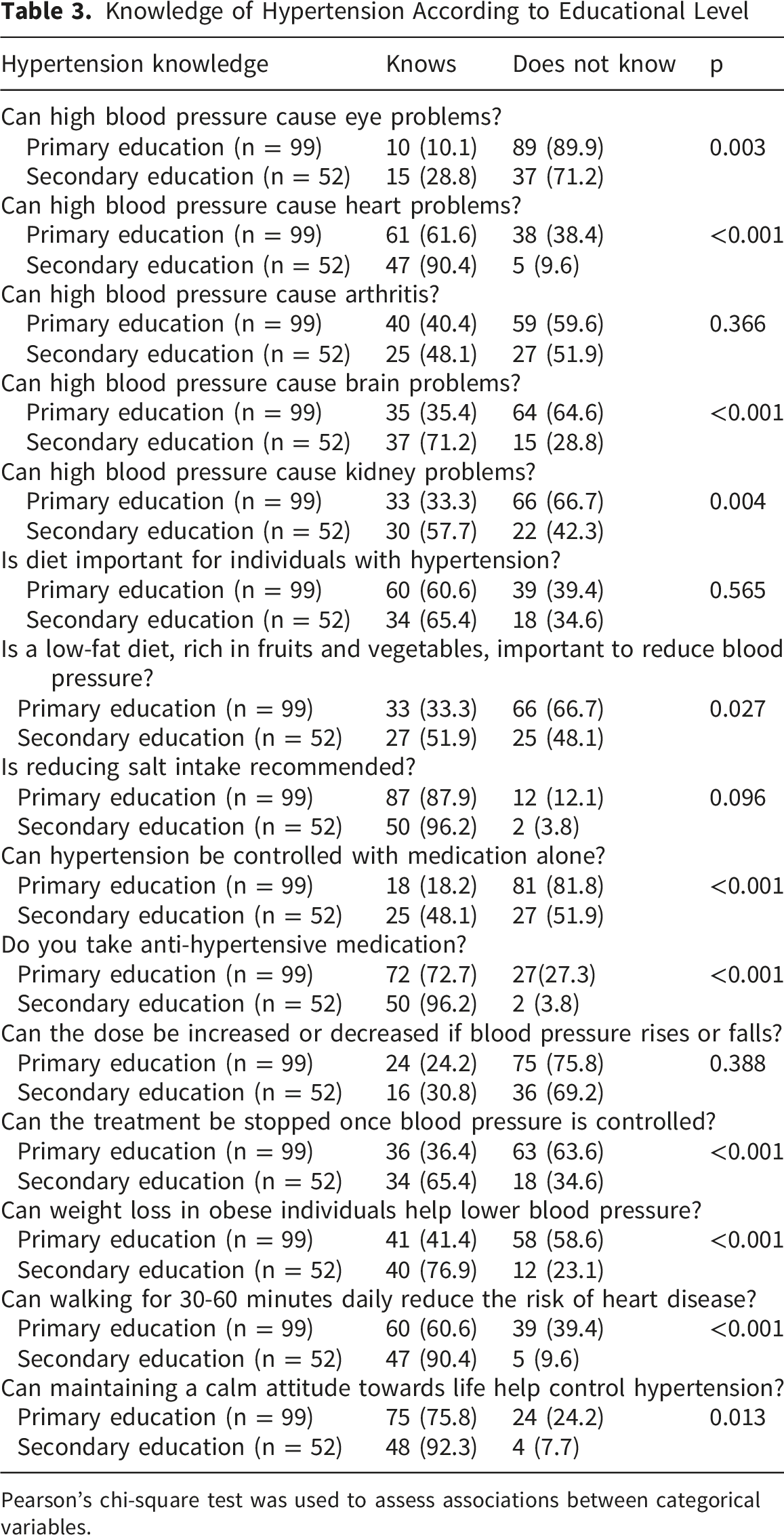
Pearson’s chi-square test was used to assess associations between categorical variables.
Discussion
This study analysed disease-related knowledge in individuals diagnosed with hypertension. The sample included 151 participants, mostly men, with a mean age of 73 years. This age distribution may be explained by the fact that hypertension becomes increasingly prevalent with age; several studies indicate that blood pressure progressively rises over the lifespan, and approximately 70% of individuals over 60 years of age have hypertension. 27 The higher proportion of men observed in our study has also been reported in other publications. 28 These differences may partly be attributed to genetic and hormonal factors, 29 with men exhibiting a higher prevalence of hypertension from adolescence. 30 However, these sex differences diminish after the sixth decade of life as the relative protective effect in women decreases and hypertension prevalence tends to equalize between sexes. 31 Nevertheless, men continue to present a slightly higher risk of developing hypertension. 32
All the participants in this study, in addition to hypertension, had chronic kidney disease, and more than half had cardiovascular disease. These comorbidities may be related to hypertension, which is considered a major risk factor for the development and progression of these conditions. 33 The coexistence of hypertension, kidney disease, and cardiovascular involvement is common given that these conditions share pathophysiological mechanisms that mutually reinforce each other. 27
Despite being diagnosed with hypertension, 94% of participants did not achieve adequate control of diastolic blood pressure, which could be related to poor treatment adherence, inappropriate medication prescription, 34 the presence of associated comorbidities – particularly chronic kidney disease, 35 lifestyle factors, and limited disease-related knowledge. 36
In relation to disease control, this study observed that women had better diastolic blood pressure control compared with men, consistent with the results reported by Leung et al (2020). 37 However, other studies have shown divergent results by sex. 38
In terms of disease-specific knowledge, significant differences were found depending on the educational level of the participants. Individuals with secondary education demonstrated greater proficiency and skills in self-blood pressure measurement, better understanding and recognition of potential complications, and more accurate identification of preventive measures and lifestyle habits for hypertension management, compared with those with primary education. In this regard, the systematic review by Mourouti et al (2022) 21 showed that individuals with higher health literacy had better blood pressure control. However, knowledge level did not necessarily explain effective hypertension control: although participants with higher education demonstrated greater disease knowledge, this did not result in better blood pressure control.
The fact that no differences were observed in blood pressure control associated with the level of knowledge, but the presence of differences according to sex, may be attributed to better treatment adherence and greater adoption of healthy lifestyle behaviours among women. 37 This phenomenon may be partly explained by sex-related differences in blood pressure regulation described in the literature, including physiological, hormonal, and behavioural factors. However, given the age profile of our sample, this potential advantage is likely reduced, although it could partly contribute to observed differences. 29
Overall, this study provides novel insights into hypertension knowledge and self-measurement practices in a Spanish primary care population, an underrepresented context, and adds methodological value by incorporating direct observation of blood pressure self-measurement, allowing for a more accurate assessment of patient competencies beyond self-reported data.
Strengths and Limitations
One of the strengths of this study is that a validated instrument is used to identify knowledge about hypertension among individuals with this condition. In addition, blood pressure self-monitoring skills were assessed through direct observation, which is a practice that is rarely described in the literature and which provides a much more comprehensive view of participants’ actual level of knowledge, competencies, and skills. This combination of methods allowed us to detect specific training needs and reinforce the validity of the results obtained. Furthermore, situating the findings within the Spanish healthcare context, aligned with European guidelines, enhances their international interpretability.
However, the study has some limitations. First, its cross-sectional design does not allow causal relationships to be established between the variables studied. Furthermore, the presence of comorbidities associated with hypertension, particularly chronic kidney disease, may have influenced our finding that their was insufficient blood pressure control.
Conclusion
Most participants with hypertension and chronic kidney disease do not achieve adequate blood pressure control. Sex and educational level influence knowledge and disease management. These findings highlight the need to adapt health education programmes to the characteristics of the population, explore how female sex may affect diastolic blood pressure control in individuals over 60 years of age, and define personalized follow-up strategies that promote treatment adherence, healthy lifestyle habits, and effective hypertension control.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki, was approved by the relevant Ethics Committee, and complied with current data protection regulations.
Consent to Participate
Informed consent was obtained from all participants included in the study.
Author Contributions
All authors contributed to the preparation and review of the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Use of AI
No artificial intelligence tools were used for the writing, analysis, and content generation of this manuscript.