
Abstract
Elderly people with chronic diseases are at risk for having severe COVID-19 disease. We were interested whether the drugs prescribed for the chronic diseases are associated with lower mortality in COVID-19 patients.
We used Finnish national registry data for analysis of potential associations of 73 prescription drugs to mortality among 6082 adult COVID-19 patients between 1.1.2020 and 30.6.2020, before COVID-19 vaccinations were available. Adjusted odds ratios (aORs) with 95 percent confidence intervals (95% CIs) for different medications are presented.
The use of three cardiovascular drugs was associated with lower 30 days all-cause mortality rate: candesartan (aOR 0.34, 95% CI 0.16-0.72, p=0.005), metoprolol (aOR 0.37, 95% CI 0.16-0.88, p=0.024) and rosuvastatin (aOR 0.44, 95% CI 0.21-0.94, p=0.034).
In conclusion, COVID-19 patients who used cardiovascular drugs candesartan, metoprolol or rosuvastatin have lower 30 days all-cause mortality than other COVID-19 patients.
Introduction
The SARS-CoV-2 is a single-stranded RNA virus, which have a strong tendency to develop new mutations in each replication cycle. 1 Due to the tendency of the SARS-CoV-2 to develop new variants as well as the fact that the virus can infect several animal species in addition to humans, 2 the eradication of the SARS-CoV-2 virus seems unlikely. Intensive research and development of vaccines as well as drugs to treat severe COVID-19 has occurred.3-5 In addition, repurposing of the existing drugs to treat, prevent or mitigate COVID-19 disease has been in the focus of the research.3,4 Important improvements for the treatment of severe COVID-19 infection have been made. In the USA, the Centers for Disease Control and Prevention recommends considering COVID-19 treatment in patients with mild or moderate COVID-19 who have one or more risk factors for severe COVID-19 to reduce progression to hospitalization and/or death. There are several possibilities for the treatment of COVID-19 infection, which vary depending on the severity of the disease. 5 These include, for example, ritonavir-boosted nirmatrelvir, intravenous remdesivir, or in selected cases dexamethasone as well as pre- and post-exposure prophylaxis. 6
Old age, male sex as well as several chronic diseases are associated to severe COVID-19 disease and increased mortality. Diseases associated to higher COVID-19 mortality include cardiovascular diseases, hypertension, diabetes, COPD, malignancy, cerebrovascular diseases and chronic kidney diseases. 7 Also, immunocompromised patients, those with chronic liver disease, psychotic disease, epilepsy or neurologic disease affecting breathing, severe chronic lung disease, sleep apnoea and severe obesity are associated with severe COVID-19 disease.8-11 Whilst the immunity of population against COVID-19 has generally improved due to vaccination programs and acquired COVID-19 infections, especially elderly people with chronic diseases are still at risk to have severe COVID-19 disease. These people are often using multiple drugs, and we do not know much on the effects of these drugs on the course of COVID-19 infection. According to previous studies, some of the common prescription drugs could have potential to lower the risk of severe COVID-19 disease and related mortality. Particularly, angiotensin-converting enzyme inhibitors and angiotensin receptor blockers have been studied for their potential to reduce COVID-19 mortality. A large study from Spain analysed these drugs in a real-world setting and found that candesartan and enalapril could reduce severity of COVID-19 disease as well as related mortality. 12
The present study was designed to evaluate the potential associations of different prescription drugs to lower COVID-19 mortality in Finnish population before introduction of COVID-19 vaccinations.
Methods
This register study is based on data extracted from the Finnish National Infectious Diseases Register upheld by the Finnish Institute of Health and Welfare and the Register of Reimbursed Drug Purchases upheld by the Finnish Social Insurance Institution (Kela). The COVID-19 patients were identified from the Finnish National Infectious Diseases Register, including all PCR-test confirmed COVID-19 cases within the study time frame, 1.1.2020-30.6.2020. The hospitals and other health care units had a statutory reporting obligation. After identifying the patients, the data on their prescription drug purchases was collected from the Register of Reimbursed Drug Purchases and information of the day of death was collected by Statistics Finland. The data on all prescription drug redemptions in Finland are automatically transferred to the national Register of Reimbursed Drug Purchases. The data collection from registers was done by the employees of the register keepers as only they have the access to these registers. The data from different registers was combined for this study by Findata. During the study, the data was stored, and the analyses were carried out in the Findata data user secure environment via remote access connections. As this is a register study and we did not contact the patients, the requirement of patient´s written consent was waived.
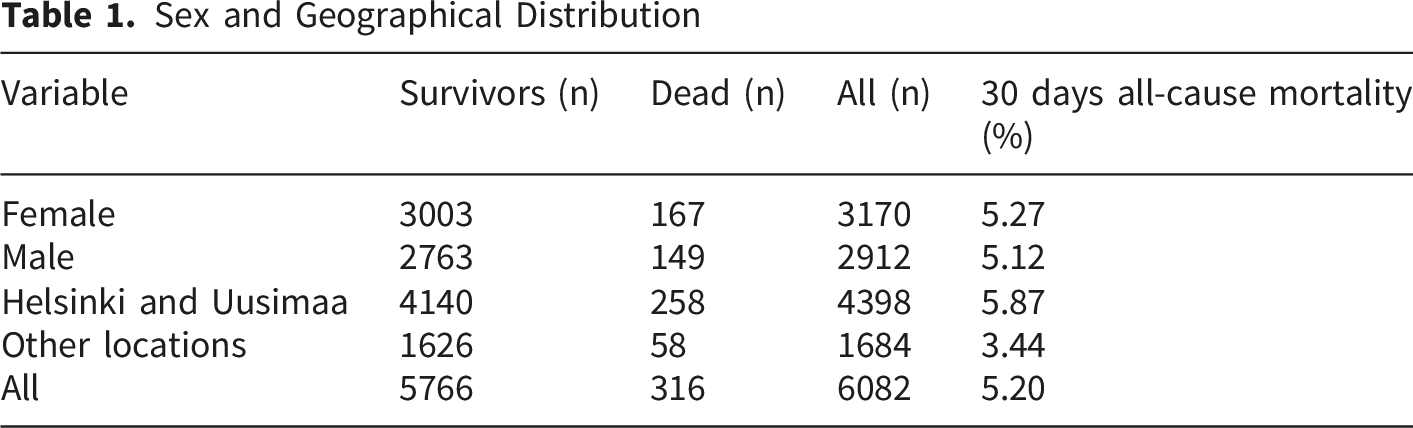
Sex and Geographical Distribution
Statistical Analyses
Data on diagnoses registered as the basis of reimbursement was used for controlling select findings in multivariable models as indicated in Results. For statistical analyses, chi-square and Fisher exact tests were used for comparisons between drug users and non-users. Each drug with unique ATC-code was analysed separately and only drugs with minimum of 50 users in the population were included in the study. Potential associations between the drug use and mortality were analysed in binary logistic regression models, with death as a dependent variable and drug use (purchase before or within 30 days from positive COVID-19 test) as an independent variable. Age at time of positive COVID-19 test and sex were used as controlling variables in all models. SPSS version 27.0 (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp) and R 4.0.3 (R Core Team (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.) softwares were used for analyses.
Results
ATC-Groups and the Number of the Studied Drugs in Each Category

Drugs Included in the Analyses

Three drugs associated with lower 30 days all-cause mortality among adult COVID-19 infected patients (Table 3): candesartan (aOR 0.34, 95% CI 0.16-0.72, p=0.0047), metoprolol (aOR 0.37, 95% CI 0.16-0.88, p=0.024) and rosuvastatin (aOR 0.44, 95% CI 0.21-0.94, p=0.034).
Discussion
The COVID-19 patients who used either candesartan, metoprolol or rosuvastatin, had significantly lower 30-days mortality rate compared with COVID-19 patients not using these drugs.
Candesartan has been in the focus of the scientific research from the very beginning of the COVID-19 pandemic for its’ potential protective effect against severe COVID-19, although there are no recommendations for using candesartan against COVID-19 outside its’ normal cardiovascular indications.14,15 In line with our results, in a Chinese study, candesartan displayed a better effect in treating patients with COVID-19 and cardiovascular diseases than other angiotensin receptor blockers. 15 A recent study from Spain reported that candesartan has a protective effect against COVID-19 mortality when used for its normal cardiovascular indications. 12
Metoprolol is a betablocker that has been proposed to be useful in critically ill COVID-19 patients. 16 In that pilot trial, intravenous metoprolol administration to patients with COVID-19-associated adult respiratory distress syndrome seemed to reduce exacerbated lung inflammation and improve oxygenation, possibly due to its’ capacity to calm down the ongoing cytokine storm.17-19 As far as we are aware, this is the first study, which shows an association between metoprolol and COVID-19 mortality.
Rosuvastatin is used for secondary prevention of cardiovascular disease in patients diagnosed with hypercholesterolemia. 20 Statins are lipid-lowering drugs with pleiotropic antithrombotic, anti-inflammatory and immunomodulatory effects. 21 It has also been hypothesized that statins might have impacts to the course of COVID-19 infection due to their ability to downregulate the receptors for angiotensin converting enzyme 2, potentially leading to decreased virus entry to cells. A study from Hubei province, China, showed reduced mortality amongst the statin-users hospitalized for COVID-19 infection. 22 Previous data reported by Davoudi et al suggests that simvastatin use is associated to less severe COVID-19 illness. They found no correlation between the COVID-19 disease severity and rosuvastatin use, however, the number of rosuvastatin users included in the study was low. 23 However, Sandhu et al and Israel et al have reported protective effect of pre-existing rosuvastatin medication against COVID-19 hospitalization.24,25 In our study, the use of rosuvastatin but not the other statins, was associated with lower 30-days all-cause mortality among COVID-19 patients.
We consider that our study cohort is rather representative because it included all PCR-confirmed COVID-19 cases in adults during the study period, before the COVID-19 vaccines were available. Still, at that time the testing capacity was insufficient, and it is likely that in our study the COVID-19 negative group includes some truly COVID-19 positive cases. At the study time frame, the population in Finland was subjected to relatively strict infection control measures, making extensive and unrecognized spreading of the virus in the population unlikely. Based on serological surveys, 0.5-1% (but not more than 1.5%) of the population became infected in the Helsinki-Uusimaa region (a hot spot for the virus spreading during the first wave) by the beginning of the July 2020. 26 Higher mortality in Helsinki and Uusimaa compared to other regions (Table 1) may be linked to relatively higher healthcare burden as this region was a hot spot for the virus spreading.
In the present study we used prescription drug purchases as an estimate of prescription drug use. It is generally known that not all the patients receiving a prescription for a certain medication are truly using it. Therefore, we selected using the prescription drug purchases, instead of data on prescribed drugs for analyses. We assume that the drug purchases are generally a good estimate for the true prescription drug use. As the data on prescription drug redemptions are automatically transferred to the national register, it will provide a comprehensive data set for the analysis. However, there are some exceptions, like pain-killers paracetamol and ibuprofen, that are commonly purchased without prescription. In case of these drugs, the register data is likely to underestimate their use.
A clear limitation in our study was that the registers used did not include comprehensive data on the other diagnoses except for COVID-19. We were unable to analyse the effects of chronic diseases, such as for example type 2 diabetes, hypertension, cardiovascular disease, COPD, cancer or kidney failure, known to associate to higher COVID-19 mortality, to the results. However, the reported protective associations of cardiovascular drugs candesartan, rosuvastatin and metoprolol upon their use according to their normal cardiovascular indications are unlikely to be biased by this in a clinically significant way. Instead, the present study design reports the protective effects of these three cardiovascular drugs in a real-world population which makes the results better generalizable to other populations. Still, the lack of comprehensive diagnosis data would significantly complicate evaluation of any potential associations of the drugs to increased COVID-19 mortality, as the underlying diseases may bias the results to unknown extent. Notably, two diabetes drugs, sitagliptin and empagliflozin, both previously suggested to have protective effects against COVID-19 mortality, were associated to higher mortality in the present study. Previous data on the effects of two diabetes drugs on COVID-19 mortality is controversial.27-29 Recently, the role of gut-brain axis and effects of microbiome to COVID-19 disease manifestations has gained increasing interest. 30 Several drugs have been shown to interfere with the gut microbiome and thereby to have complex effects to the gut-brain axis and immune system.31,32 The connection between the alimentary tract and nervous system drugs and COVID-19 related mortality may suggest role of gut-brain axis dependent underlying mechanisms and warrants further studies.
Conclusions
In conclusion, the COVID-19 patients who used either candesartan, metoprolol or rosuvastatin had significantly lower 30-days all-cause mortality rate than non-user controls. Further studies are needed to explore the causes of death in the users and non-users of these drugs to better understand the mechanisms of the protective effects. Also, more research is needed to show whether the protective effects of candesartan, metoprolol and rosuvastatin against 30-days mortality among unvaccinated COVID-19 patients will be repeated in vaccinated COVID-19 patients. Favoring these drugs associated with lower mortality over other drug options could help to further reduce COVID-19 associated mortality of patients with cardiovascular diseases in a population level.
Footnotes
Acknowledgements
We thank professor Per Ashorn from Tampere University for his encouragement and help in getting started with this study.
Ethical Considerations
Not applicable, as stated by the regional medical research ethics committee of the Wellbeing Services County of Pirkanmaa. In Finland, the Medical Research Act (no. 488/1999) states that approval from the local ethics committee is not required for register-based surveys that do not process identifiable information.
Consent to Participate
As required by the national legislation, the need for informed consent was waived (as this is a register study and the patients were not contacted) and the use of national registry data was authorized by Finnish Social and Health Data Permit Authority Findata (THL/3112/14.02.00/2020). The study was conducted according to the declaration of Helsinki.
Author Contributions
A.H. and M.H designed the study and analysed the data, all authors contributed to interpretation of data, A.H. and H.S. have drafted the work and all authors substantively revised it.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank two Finnish research foundations, Onni ja Hilja Tuovisen säätiö sr. and Avohoidon tutkimussäätiö, for supporting the study (grants to A.H.).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The research permission does not allow sharing the data outside the research group defined in the permission. If one would like to use the data for research purposes, research permission for this should be applied from the Finnish Social and Health Data Permit Authority Findata.