
Abstract
Objectives
The purposes of this study were to: (1) identify the prevalence of diagnosed and potentially undiagnosed obstructive sleep apnea (OSA) among overweight/obese non-Hispanic Black and Hispanic men ages ≥40 years with ≥1 chronic condition; and (2) examine factors associated with potentially undiagnosed OSA among these men.
Setting
Using an internet-delivered survey, data were analyzed from 942 overweight/obese Black and Hispanic men with chronic conditions.
Methods
Approximately 35% reported an OSA diagnosis; 65% were believed to have potentially undiagnosed OSA because of being overweight/obese, snoring loudly, and/or stopping to breathe while sleeping. A logistic regression was fitted to examine the association with potentially undiagnosed OSA, adjusting for sociodemographics, disease characteristics, health status, social support, and lifestyle behaviors.
Results
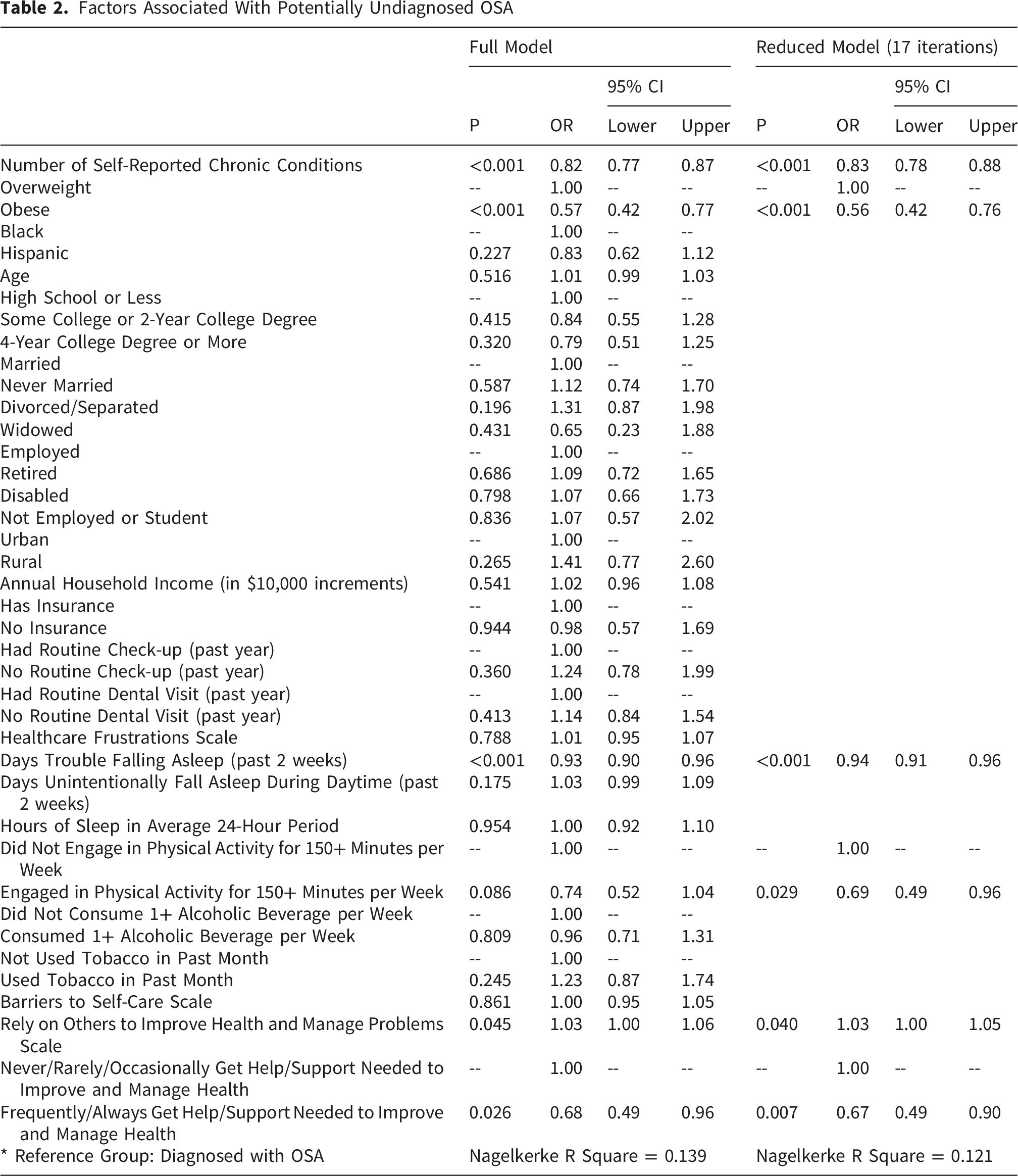
Men with more trouble falling asleep (OR=0.94, P<.001), fewer chronic conditions (OR=0.83, P<.001), obesity (OR=0.56, P<.001), and engaged in ≥150 minutes/week of physical activity (OR=0.69, P=.029) were less likely to have potentially undiagnosed OSA. Greater reliance on others to manage problems predicted higher odds of undiagnosed OSA (OR=1.03, P=.040), whereas frequently receiving needed health-related support were less likely to have potentially undiagnosed OSA (OR=0.67, P=.007).
Conclusions
OSA may remain unrecognized among non-Hispanic Black and Hispanic men with less severe disease profiles and mild disordered breathing symptomatology. Findings highlight the need for routine OSA screening and strategies to reduce disease self-care barriers among men with chronic conditions.
Introduction
Obstructive sleep apnea (OSA) is a common sleep-related breathing disorder characterized by intermittent obstruction of the upper airway during sleep, leading to disrupted airflow and fragmented sleep.1,2 Symptoms typically include loud snoring, gasping, and choking episodes during sleep, accompanied by excessive daytime fatigue.1-4 OSA is particularly prevalent among individuals who are overweight or obese,5,6 as excess fat around the neck area can constrict the airway during sleep.7-10 OSA is linked to numerous chronic health conditions, including hypertension, stroke, coronary artery disease, and heart failure.11-16 It is also associated with mood disorders such as depression, anxiety, and irritability,17,18 erectile dysfunction,19,20 and reduced quality of life. 21
The prevalence of OSA is estimated to be 32.4% (or 83.7 million) among adults in the United States 22 ; however, approximately 80% of this population is undiagnosed or not receiving OSA treatment. 23 Untreated OSA exacerbates these risks by increasing the workload on the heart and contributing to systemic inflammation. 24 While bed partners often report symptoms such as loud snoring or breathing cessations during sleep, 25 OSA diagnosis involves clinical evaluation and objective testing methods such as polysomnography or home sleep apnea tests. 26 Proper detection is essential for patients to receive treatment or management techniques. 27
OSA is particularly concerning for middle-aged and older adults because it can precede and exacerbate several chronic and life-threatening conditions like heart disease, stroke, diabetes, and metabolic syndrome.28,29 Despite its significant health implications, OSA remains underdiagnosed, particularly among Black and Hispanic men.7,8,26,30-32 The purposes of this study were to: (1) identify the prevalence of diagnosed and potentially undiagnosed OSA among overweight/obese non-Hispanic Black and Hispanic men ages ≥40 years with ≥1 chronic condition; and (2) examine factors associated with potentially undiagnosed OSA among these men.
Materials and Methods
Participants and Procedures
This cross-sectional study analyzed data collected using an internet-delivered questionnaire from a nationwide non-probabilistic convenience sample. The survey was conducted between September and October 2019. Participants were recruited from a Qualtrics Online Panel, 33 using a non-probability sampling approach drawing from its managed research panels, based on specific inclusion criteria. For the parent study, 34 all participants were required to be: (a) male; (b) either non-Hispanic Black or Hispanic; (c) age 40 years or older; and (d) self-report having one or more chronic conditions. Qualtrics reached potential participants through their pool of pre-verified adults who opt-in to participate in online surveys. Eligible participants were directed to an internet-based survey link where they were presented with an information sheet approved by the Institutional Review Board at Texas A&M University (IRB ID: 2018-1684). Participants were allowed to complete the online questionnaire only after acknowledging the information sheet. Participants were directly compensated by Qualtrics, not the researchers, for completing the online questionnaire.
As described in detail elsewhere, 34 the questionnaire was purposively constructed to assess healthcare access and utilization, barriers to disease self-care, and health-related lifestyle behaviors and perceptions among non-Hispanic Black or Hispanic men ages 40 years and older with one or more chronic conditions. Items and scales included in the questionnaire were primarily drawn from established and validated sources including the Behavioral Risk Factor Surveillance System,35,36 National Council on Aging Chronic Care Survey, 37 National Study of the Chronic Disease Self-Management Program,38,39 and Brazos Valley Health Status Assessment. 40 Permission to use items and scales were obtained, when required. Additional items created by the research team were also added to the questionnaire. On average, respondents required approximately 30 minutes to complete the instrument.
The total number of men recruited for the study through the Qualtrics Online Panel is unknown. However, 2,029 men met the inclusion criteria and completed the questionnaire. Of those, 47 cases were omitted from analyses due to the low sample size of those reporting being both Black and Hispanic. Of the remaining 1,982 men, a secondary analysis was performed to meet the current study goal of identifying potentially undiagnosed OSA. For these secondary analyses, cases were omitted for those who reported: (a) not being overweight or obese (n=481); (b) not ever being told they snore and/or sleep loudly when sleeping (n=532); and (c) not having information about routine healthcare utilization (n=27). After applying these inclusion criteria, the final analytic sample included 942 non-Hispanic Black and Hispanic men ages 40 years and older who were overweight or obese with one or more chronic conditions and either diagnosed OSA or potentially undiagnosed OSA.
Measures
Dependent Variable
The dependent variable for this study was OSA diagnosis status. Aligned with the aim of this study to identify potentially undiagnosed OSA, we created a definition based on literature. Given the strong association of OSA with weight,41-44 we limited our sample to only include men with body mass index (BMI) scores indicative of overweight and obese status. BMI was calculated as self-reported weight (pounds) divided by height (inches), 2 multiplied by 70345,46 and categorized as overweight (≥25 kg/m2) or obese (≥30 kg/m2). 47
Well-documented signs of OSA are snoring and stopping breathing while sleeping.3,48 As such, the survey asked participants to report “Has anyone ever told you that you snore loudly?” and “Has anyone ever told you that you stop breathing while you sleep?” The response choices for these two items were ‘no’ or ‘yes.’ These categories were combined to create a 4-category variable. After omitting men who reported never being told that they snore loudly or stop breathing while sleeping, we were left with a 3-category OSA symptom variable (i.e., snore only, stop breathing only, both snore and stop breathing). Participants were also asked to self-report if a healthcare provider ever told them they had OSA. Response choices were ‘no’ or ‘yes.’ Based on a combination of these variables, we created a dichotomous variable among all overweight and obese men to identify their OSA diagnosis status (i.e., OSA diagnosis, potentially undiagnosed OSA). OSA diagnosis (scored 0) indicates the participant self-reported an OSA diagnosis, which serves as the reference group for analyses. Potentially undiagnosed OSA (scored 1) is defined as the participant not self-reporting an OSA diagnosis; rather, being told they snored loudly and/or stopped breathing while sleeping, which is highly indicative of undiagnosed OSA.
Sleep Symptoms
Participants were asked to report about two aspects of their sleep quality. Participants were asked to report the number of days in the past two weeks that they had trouble falling asleep (i.e., continuous variable ranging from 0 to 14 days). Participants were also asked to report the number of days in the past two weeks that they unintentionally fell asleep during the daytime (i.e., continuous variable ranging from 0 to 14 days).
Healthcare Utilization and Perceptions
Participants were asked to report if they currently had health insurance, with a response choice of ‘no’ or ‘yes.’ They were also asked how long it had been since their last routine check-up with a healthcare provider and dental visit. Both items had response choices ranging from ‘in the past year’ to ‘five years ago or longer,’ which were dichotomized into ‘in the past year’ (scored 0) and ‘longer than one year ago’ (scored 1). Participants also completed the Healthcare Frustrations Scale,49,50 which is a 6-item scale that assesses whether participants felt frustrations related to interactions such as ‘felt tired of describing their same conditions and problems every time they go to a hospital or doctor’s office,’ ‘left the hospital or doctor’s office and felt confused about what they should do,’ ‘wished their doctor had more time to spend talking with them,’ and ‘felt that their doctor does not realize what it is really like for them at home trying to take care of their health problems.’ Response choices included ‘never,’ ‘occasionally,’ and ‘frequently.’ Items were summed to create a continuous scale ranging from 6 to 18, with higher scores indicating higher healthcare frustrations. The Cronbach’s alpha scale value for the current sample was 0.856.
Health Indicators
Health indicators of interest were self-reported chronic conditions and obesity status. Chronic conditions were self-reported by participants using a ‘check-all-that-apply’ checklist of 17 conditions, including arthritis/rheumatic disease, cancer, chronic pain, diabetes, heart disease, kidney disease, osteoporosis, and thyroid problems. The number of chronic conditions reported were summed to create a continuous variable ranging from 1 to 17 conditions (i.e., as indicated previously, having 1+ chronic conditions was required to be in the parent study).
Health Behaviors
Self-reported lifestyle health behaviors included in analyses were the average number of hours slept within a 24-hour period (i.e., continuous variable ranging from 0 to 24 hours), physical activity engagement for 150 minutes or more in an average week (i.e., no or yes), alcoholic beverage consumption in the past week (i.e., no or yes), and use of tobacco in the past month (i.e., no or yes).
Self-Care and Social Support
Participants completed the Barriers to Self-Care Scale,49,50 which is a 4-item scale that assesses the participants’ perceived challenges to health management such as ‘need help learning what they should be doing to take better care of their health,’ ‘need help learning how to take better care of their health in a way that works for them and their life,’ and ‘not having the money it takes to do things that will improve their health or condition.’ Each item was scored on a 4-point Likert-type scale ranging from ‘strongly disagree’ to ‘strongly agree.’ Items were summed to create a continuous scale ranging from 5 to 20, with higher scores indicating more barriers to self-care. The Cronbach’s alpha for the current sample was 0.839.
Participants were asked to report on the frequency they received the help and support needed to improve their health and manage their health problems.49,50 Response choices for this single item ranged from ‘never’ to ‘always’ on a 5-point Likert-type scale. Based on the frequency distribution, this variable was dichotomized to include the categories of ‘never/rarely/occasionally’ (scored 0) and ‘frequently/always’ (scored 1). Participants also completed the Reliance for Ongoing Help/Support to Improve Health and Manage Health Problems Scale,49,50 an 8-item scale that assesses participants’ reliance on receiving help and support from others to improve their health and manage health problems. The eight sources of support reliance included their spouse/partner, friends/relatives, co-workers, healthcare providers, the internet, community groups, faith-based organizations, and people with similar health problems. Response choices for each item were measured on 5-point Likert-type scales ranging from ‘not at all’ to ‘a great deal.’ Scores were summed to create a composite score ranging from 8 to 40, with higher scores indicating more reliance on others. The Cronbach’s alpha for the current sample was 0.827).
Sociodemographics
Personal characteristics included in analyses were race/ethnicity (i.e., non-Hispanic Black and Hispanic), age (i.e., continuous variable ranging from 40 to 93 years), education status (i.e., high school or less, some college or 2-year college degree, and 4-year college degree or more), marital status (i.e., married, never married, divorced/separated, and widowed), employment status (i.e., employed, retired, disabled, and not employed or student), residential rurality (i.e., urban or rural status based on county-level rural-urban continuum codes, 51 and annual household income (i.e., continuous variable in $10,000 increments ranging from $10,000 to $150,000+).
Data Analyses
All analyses were performed using SPSS 29.0 software (SPSS Inc., Chicago, IL, USA). Descriptive statistics were calculated for all study variables, which were initially compared by OSA diagnosis status. Pearson’s chi-square tests were used to identify proportion differences for categorical variables, and independent sample t-tests were used to identify mean differences for continuous variables. A binary logistic regression model with backward stepwise entry was fitted to identify factors associated with having potentially undiagnosed OSA (i.e., self-reporting an OSA diagnosis served as the reference group). The full model including all variables and the reduced model with the most relevant predictor variables are presented. For this study, statistical significance was identified at P < 0.05 for all analyses.
Results
Sample Characteristics by OSA Diagnosis Status
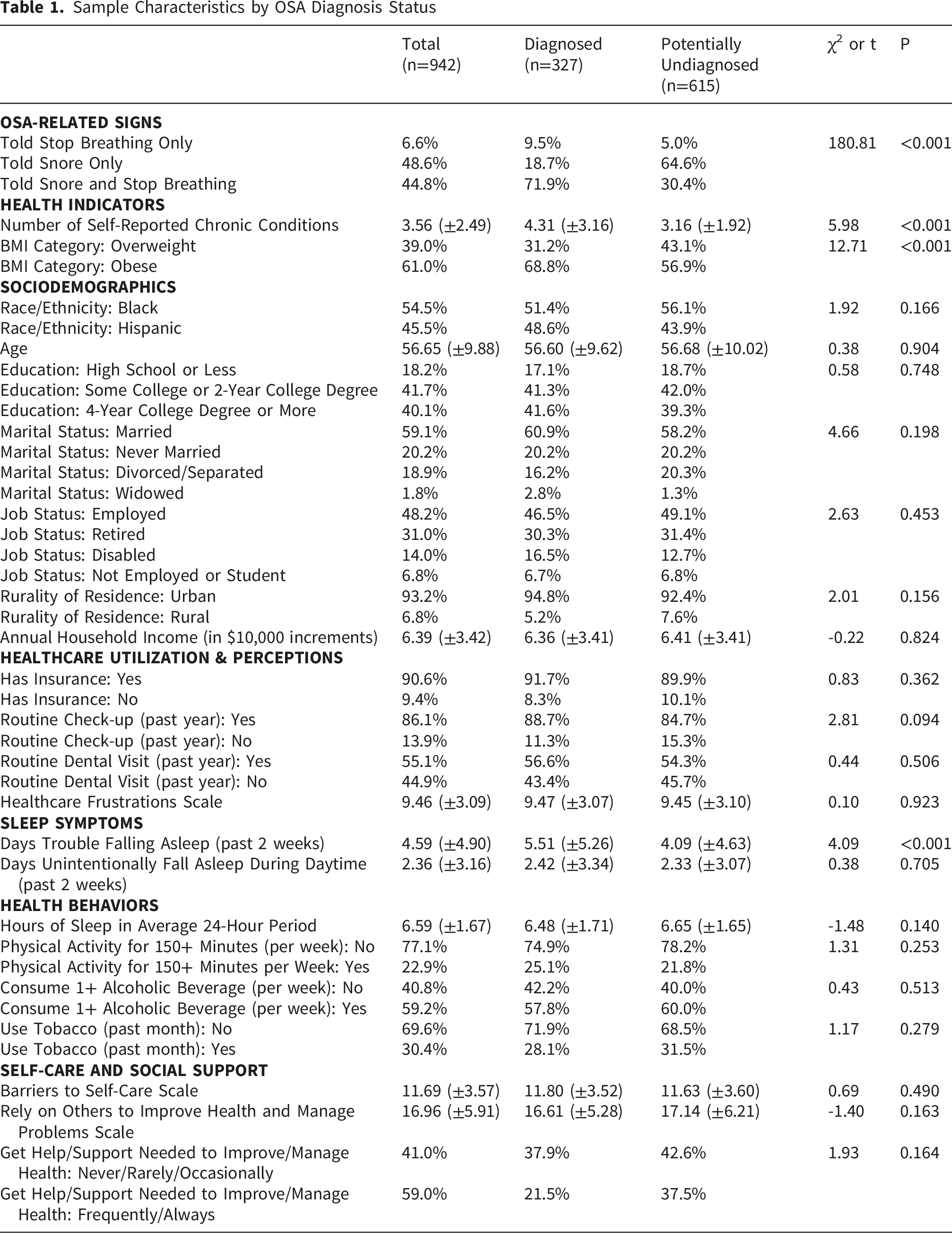
Most participants had either some college education or a 2-year college degree (41.7%) or a 4-year college degree or more (40.1%). Most participants had health insurance (90.6%). In the past 12 months, 13.9% of participants did not have a routine physician visit and 44.9% did not have a routine dental visit. On average in a 24-hour period, participants reported getting 6.59 hours of sleep. On average in the past 2 weeks, participants reported 4.59 days having trouble falling asleep and 2.36 days of unintentionally falling asleep during the daytime. About 23% of participants reported not engaging in physical activity for 150 or more minutes each week, 59.2% consumed one or more alcoholic beverage a week, and 30.4% used tobacco in the past month.
When comparing sample characteristics by OSA diagnosis status, a larger proportion of men with diagnosed OSA reported being told they both snore and stop breathing while sleeping, whereas a larger proportion of men with potentially undiagnosed OSA reported being told they snore only (χ2=180.81, P<0.001). On average, relative to those with potentially undiagnosed OSA, men with diagnosed OSA reported more chronic conditions (t=5.98, P<0.001) and more days having trouble falling asleep (t=4.09, P<0.001). A significantly larger proportion of men with diagnosed OSA were obese relative to men with potentially undiagnosed OSA (χ2=12.71, P<0.001).
Factors Associated With Potentially Undiagnosed OSA
Discussion
This study examined the prevalence of OSA and potentially undiagnosed OSA among overweight or obese non-Hispanic Black and Hispanic men with chronic diseases. The findings underscore critical gaps in diagnosis and highlight actional strategies to address these disparities. The study findings suggest that OSA frequently remains undiagnosed among men with less severe disease profiles. Specifically, men with fewer chronic conditions and those who were overweight rather than obese were more likely to have undiagnosed OSA. This association may reflect the fact that individuals with more severe health conditions, who experience more pronounced and frequent OSA symptoms, are more likely to seek medical care, prompting OSA screening and subsequent diagnosis. 52 Conversely, delays in accessing healthcare for those with milder conditions may exacerbate the underdiagnosis of OSA in this population. 10 These findings emphasize the importance of targeted screening efforts for individuals who may not present with severe health conditions but remain at high risk for OSA. 31
Our findings suggested an inverse association between trouble falling asleep and the likelihood of receiving an OSA diagnosis. This finding may be explained by the fact that men who are diagnosed with OSA are often already receiving treatment interventions using Oral Appliance Therapy (OAT) or Continuous Positive Airway Pressure (CPAP), which are known to improve sleep quality in OSA patients and mitigate symptoms such as difficulty falling asleep.53,54 Furthermore, difficulty falling asleep is not a key symptom of OSA compared to excessive daytime sleepiness or loud snoring, which are more commonly recognized as diagnostic indicators, 55 which may explain potential undiagnosed OSA. Relative to men diagnosed with OSA, those with potentially undiagnosed OSA were less likely to engage in recommended physical activity levels. This finding aligns with previous research indicating that sedentary lifestyles is prevalent among individuals with undiagnosed OSA.56-58 These findings may suggest that receiving an OSA diagnosis can be an adverse event that prompts men to adopt healthier behaviors to manage OSA and its symptomatology, making early diagnosis even more important.
Men who frequently received support in managing their health problems were more likely to be diagnosed with OSA. This is consistent with Kong and colleagues 59 who reported that social support enhances self-efficacy in OSA patients, making them more likely to seek screening and adhere to treatment. Social support systems may therefore play a critical role in helping to bridge the gap in OSA diagnosis. 60 Conversely, potentially undiagnosed men were more likely to rely on others to help manage their health. This reliance on others may suggest low personal agency to receive screenings and/or self-manage their health conditions. 61
The findings highlight the urgent need for routine OSA screening and interventions to reduce barriers to disease self-management among non-Hispanic Black and Hispanic men with chronic conditions. A previous study has demonstrated that populations, such as non-Hispanic Black and Hispanic men, are disproportionately affected by these conditions and face unique challenges when it comes to both the identification and management of OSA. 30 These disparities emphasize the importance of early detection and intervention, which could mitigate the long-term consequences of OSA, including cardiovascular events and cognitive decline. Routine screening for OSA by medical professionals such as primary care physicians (PCPs) and dentists can be critical in improving early diagnosis, especially for high-risk populations. Dentists, for example, can look for physical signs such as enlarged tonsils or a small airway, while PCPs can assess sleep-related symptoms like excessive daytime sleepiness and snoring. 62 Since these professionals, who have frequent interactions with patients, are in an ideal position to identify potential signs of sleep apnea during routine exams, training these professionals to recognize the symptoms of OSA and implement screening during routine visits can lead to more timely referrals and interventions.62,63 Training these professionals to recognize potential signs of OSA and implement screening during routine visits could significantly improve early detection rates.62,63 Other actionable strategies to increase OSA detection in clinical settings may be to routinely integrate OSA screening into care pathways (e.g., specialty physicians seeing and treating patients for hypertension, cardiovascular disease, diabetes, metabolomic syndrome) and incorporating OSA prompt alerts into electronic medical records for patients with multiple chronic conditions. Addressing systemic barriers such as limited access to healthcare and health insurance coverage will be essential for reducing OSA diagnostic disparities in non-Hispanic Black and Hispanic male populations.64-66
Limitations
The current study had several limitations that must be acknowledged. First, the parent study focused on non-Hispanic Black and Hispanic men with chronic health conditions. While this purposive sampling approach was essential to address the study questions, it omitted inclusion of women and men from other racial and ethnic groups, which may limit opportunities for broader comparisons and insights. Second, the cross-sectional nature of the dataset restricts the ability to infer causal relationships. Third, all data were self-reported, which may have introduced reporting bias. Fourth, despite creating an instrument from established and validated sources, the newly formed questionnaire was not pre-piloted with the target population prior to grand-scale dissemination. Fifth, data collection relied exclusively on a Qualtrics Online Panel, which may have limited the sample’s representativeness of all non-Hispanic Black and Hispanic men living with chronic health conditions. Collecting data using only online methods may have limited participation from men without internet access, of less affluence, and in rural communities. Sixth, the definition pertaining to OSA diagnosis status may have either over- or under-estimated OSA prevalence. As mentioned, data were based on self-report that were not objectively confirmed with polysomnography or other clinical sleep tests. While potentially undiagnosed OSA was defined by a combination of BMI category (i.e., overweight, obese) and OSA-related symptoms (i.e., snoring loudly, stopping breathing while sleeping), which are consistent with clinical literature, 67 such criteria does not guarantee that OSA was present and undiagnosed among these men. Finally, a component of the potentially undiagnosed OSA definition was reporting one or both OSA-related signs (i.e., snoring loudly, stopping breathing while sleeping). It is possible that these symptoms were underreported due to contextual factors, such as lack of a bed partner, partners sleeping in separate rooms, deep-sleeping bed partners), thus limiting the identification of participants with potentially undiagnosed OSA.
Conclusion
This study provides important insights into the critical need for routine screening and intervention for OSA among non-Hispanic Black and Hispanic men who are overweight/obese and with chronic conditions, as these individuals face disproportionately high risks of being undiagnosed. The study emphasizes the pivotal role of healthcare professionals, particularly primary care physicians and dentists, in proactively identifying at-risk individuals, facilitating timely diagnoses, and ensuring appropriate treatment. It also underscores the necessity to address systemic barriers such as limited healthcare access, low awareness of OSA symptoms, and modifiable lifestyle factors such as obesity and physical inactivity to mitigate risk factors for OSA in this population.
Supplemental Material
Supplemental material - Potentially Undiagnosed Obstructive Sleep Apnea Among Non-Hispanic Black and Hispanic Men in the United States
Supplemental material for Potentially Undiagnosed Obstructive Sleep Apnea Among Non-Hispanic Black and Hispanic Men in the United States by Matthew Lee Smith, Jeong-Hui Park, Abigail Rister, Oluyomi Oloruntoba, Ledric D. Sherman, Harold A. Smith, Ashley L. Merianos and Caroline D. Bergeron in Journal of Primary Care & Community Health.
Consent for Publication
The informed consent document signed by all participants explicitly stated that the study findings would be disseminated through publication. In addition, all authors have provided consent for publication of the final manuscript and the associated data.
Footnotes
Ethical Considerations
This research was approved by the Institutional Review Board at Texas A&M University (IRB ID: 2018-1684).
Consent to Participate
All participants provided written consent to participate.
Author Contributions
Conceptualization: MLS, HAS; Methodology: MLS; Formal Analysis: MLS; Investigation: MLS, LDS; Result Interpretation: MLS, JHP, AR, OO, LDS, HAS, ALM, CDB; Writing - Original Draft: MLS, JHP, AR, CDB; Writing -Review & Editing: MLS, JHP, AR, OO, LDS, HAS, ALM, CDG; Funding Acquisition: MLS, LDS
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Texas A&M University through their Texas A&M Triads for Transformation (T3) initiative.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon request to the corresponding author;
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.