
Abstract
Background
Prolapse following birth is common. Between 33-79% of postnatal women will have a prolapse on examination, and 43% of these women report severe symptoms. Postnatal women with a prolapse struggle to fulfil parental caring responsibilities and are five times more likely to have postnatal depression. This study aims to investigate the barriers and facilitators for postnatal women accessing services for postnatal prolapse in the UK.
Methods
We undertook semi-structured qualitative interviews with postnatal women with pelvic organ prolapse symptoms, pelvic health physiotherapists, primary and secondary care nurses and general practitioners. Participants were purposefully sampled. Reflective thematic analysis was used to analyse the data.
Results
From eight interviews, five themes were generated in relation to the barriers and facilitators for postnatal women accessing services for postnatal prolapse. These were: the screening process after birth; cultural approach to symptoms; the ideal care pathway, clinical pathways and health literacy for women. Suggested improvements included standardising screening appointments with routine vaginal examinations, improved clinician training to improve treatment choices and approach to symptoms, educating women about normal vaginal anatomy after birth, alongside the implementation of dedicated services for postnatal women with prolapse.
Conclusion
This research suggests a need for a dedicated service and a review of existing clinical pathways for postnatal women with prolapse. The optimal service model should take screening and health literacy into consideration. Future research in this area should evaluate effective treatments for postnatal prolapse and the changes needed to standardise approaches to care for postnatal prolapse symptoms.
Introduction
Pelvic organ prolapse is a common, stigmatising condition, severely impacting quality of life (QOL) in women. The International Continence Society defines prolapse as ‘the descent of one or more of the anterior vaginal wall, posterior vaginal wall, the uterus or the apex of the vagina. 1 ’ Prolapse symptoms include bulge or heaviness in the vagina, which may stop women continuing with activities of daily living. Globally, childbirth is one of the biggest risk factors of women developing a prolapse.2-6 A large cohort study of 1,100 women in the United States found vaginal birth increases the likelihood of developing pelvic organ prolapse five-fold compared with caesarean delivery. 7 Pregnancy has also been established as a risk factor for prolapse.8,9 A cohort study based in China, found 33-79% of postnatal women have prolapse on examination up to one year after giving birth, 10 and up to 43% of women report severe symptoms. 11 In addition to physical symptoms, qualitative research in Sweden indicates that prolapse can have notable psychological effects on women during the postnatal period. 12 Postnatal women report not being able to fulfil their parental caring responsibilities, are less like to exercise, will adapt activities of daily living and are less likely to return to work.12-15 This has a large economic and social burden on society.
There is an increasing focus on treating prolapse with conservative management. 16 The National Institute for Health and Care Excellence (NICE) suggests pelvic floor muscle exercises, pessary or surgery as treatments for prolapse. 17 Conservative treatments are particularly important for younger women, as surgery is not only not a suitable option for women who have not completed their family, but younger women are more likely to experience prolapse reoccurrence after surgery. 18 Additionally, using mesh in prolapse surgery has been suspended in some countries, 16 as such, conservative treatments are becoming the first line treatment.
Current services and pathways for postnatal prolapse in the UK are varied. 19 In secondary care, the service is usually delivered in a gynaecology department within a service for all ages of women, often with long waiting lists. 20 Alternatively, some perinatal services are delivered by pelvic health physiotherapists and offer pelvic floor muscle exercises but not always a pessary, and some GPs or nurses in primary care can offer pessary management. Services for women’s health are fragmented and difficult to access. 21
There has been limited research on women’s and clinicians’ perspectives of the barriers and facilitators to postnatal women accessing treatment for prolapse in the context of this varied practice. To address this knowledge gap, we sought to explore the perceived barriers and facilitators of accessing conservative treatment for prolapse for postnatal women.
Materials and Methods
Qualitative semi-structured interviews were conducted with clinicians treating postnatal prolapse in the UK and women from Cambridge University Hospitals NHS Foundation Trust and national online support groups. The Consolidated Reporting of Qualitative Research (COREQ) checklist 22 was used to report findings (Appendix 1). Ethical approval was granted by Liverpool Central Research Ethics Committee (24/NW/0016).
Design and Setting
Women at an acute hospital trust in the UK, who birthed a baby in the past 2-years and were over the age of 18-years with prolapse symptoms were invited to take part in the study. Prolapse diagnosis was self-reported as a heaviness, bulge or something coming down in the vagina. There was no restriction by mode of birth. Women were invited to take part through a letter of invitation in clinics and via an online invitation within the support groups.
UK clinicians treating postnatal women with over two years’ experience were also invited to take part. We recruited participants through social media posts for clinician specialist interest groups (Royal College of Nursing, Pelvic Obstetric and Gynaecological Physiotherapy, and General Practitioners with Specialist Interests in Women’s Health). An advert was posted on the social media platforms inviting clinicians to take part in the research and to contact the research physiotherapist. Interviews were conducted with nurses, physiotherapists and GPs, working in private clinics, and primary or secondary care. Purposive sampling was used with the aim of recruiting two women who received private or NHS treatment, and two participants in each profession. Eight to ten interviews were planned based on previous literature depending on when theoretical data saturation was achieved. 23 The research team met regularly to reflect on emergent themes and to ensure interviews generated meaningful data, rather than repetitive data.
A patient and public involvement and engagement (PPIE) steering group was formed for this research. PPIE members were recruited from clinics, listening events and from women who independently approached the research team. In total, 12 women with lived experiences of postnatal prolapse were part of this group. Two semi-structed interview prompt guides were finalised by the PPIE steering group (Appendix 2). The clinician guide included prompts on accessing treatment, suitable treatment options and determinants of treatment options. The interview guide for women included prompts for accessing suitable treatments. Questions were open ended, and participants were encouraged to explore their thoughts relevant to the questions and had an opportunity to ask about the research.
Data Collection and Analysis
An experienced pelvic health and research physiotherapist (CB) conducted the interviews in English. Participants were given the option of in person or virtual interviews. All participants chose virtual interviews and these were conducted using Microsoft Teams. Interviews were audio recorded and professionally transcribed. The transcribing company was compliant with General Data Protection Regulation policies and confidentiality agreements.
Reflective thematic analysis was used to analyse the data. 24 This is a qualitative research method used to develop, analyse and interpret patterns within the interviews. This method was chosen to explore multiple perspectives of a complex condition. The research team agreed theoretical saturation was reached at the eighth interview for the whole data set as no new themes emerged. An initial coding framework and initial themes were generated by the research physiotherapist with a background in pelvic health. An inductive approach was used, consistent with reflexive thematic analysis. The transcripts were read immediately for data immersion and familiarity. Codes were then grouped into broader patterns of meaning. Major themes were rechecked against initial coding and the raw data. To ensure rigor, a second reviewer (JM) with expertise in qualitative analysis checked the raw data against themes and these were refined. In line with reflexive thematic analysis, the research team engaged in ongoing reflexive discussions and reflexive journaling to consider how professional backgrounds influenced interpretation. The steering group was invited to review the coding framework and generated themes. One member (CZD) participated in this process and provided feedback on the analysis and manuscript.
Results
Demographics
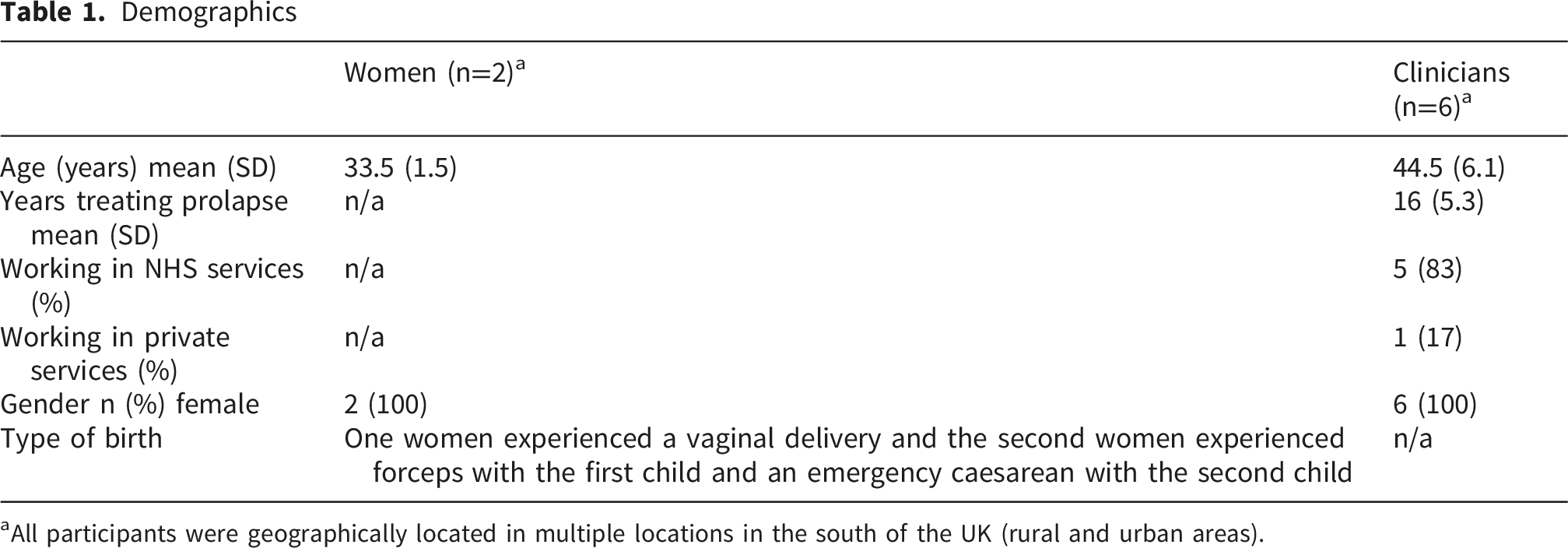
aAll participants were geographically located in multiple locations in the south of the UK (rural and urban areas).
Supplementary Quotes to Support Overarching Themes

The Screening Process
Women and clinicians identified barriers with the current screening processes for diagnosing postnatal prolapse. Women and clinicians both highlighted that the GP postnatal appointment at 6-8 weeks is baby focused, and the health of the woman came second, as such, this shows the health needs of women were often not addressed and are less important than the baby’s health. The practicalities of having a joint appointment with the woman and baby led to pelvic floor issues not being discussed. Women and clinicians highlighted a vaginal examination is not always offered at the screening appointment. This will impact on the ability to diagnose a prolapse leaving many women undiagnosed and untreated.
‘…when we do the postnatal baby checks, we do it as a joint appointment with the mum and the baby and often the focus really is just on the baby…’ (GP 1)
Indirect questioning was seen as a barrier to diagnosing a postnatal prolapse. Clinicians reflected that it is often the expectation (by a clinician) that a women will request a vaginal examination if needed. The gender of the examining GP was also thought to why women did not ask for an examination. This could lead to women not being examined due to relational vulnerability and gender dynamics.
‘…often women have to ask to be assessed, and I think that’s a really difficult conversation, it’s really hard, especially if it’s a male doctor…’ (physiotherapist 7)
Consequently, direct questioning of pelvic health conditions was discussed as a facilitator for screening for a postnatal prolapse.
‘…we need to ask [women] directly, it ought to be one of the postnatal questions when they’re doing the postnatal checks. Are you experiencing any incontinence? Are you feeling any bulging? Do you feel like your insides are dropping out?’ (nurse 3)
Other facilitators for accessing care were described as improvements to the screening process. Women discussed the need for standardisation. Women commented on comparing their screening appointment with friends and found discrepancies.
‘…I think we need to have a sort of consistency between districts really about what happens at the appointment, because things were missed…. (woman 5)
Other improvements to the screening process suggested by clinicians included using opportunities at other appointments to ask direct pelvic floor health related questions, only offering face-to-face appointments, tailoring screening appointment depending on women’s needs and identifying high risk women.
‘…last time I went for a smear test they asked me about domestic violence, like that’s one of their screening questions…. if we can ask about domestic violence, can’t we say, have you got any symptoms.’ (physiotherapist 6)
These quotes demonstrate a clinician’s awareness of the value of asking direct questions, however restricted time within screening appointments may limit the clinicians’ ability to do so. Women also are aware of the lack of standardisation of questioning around pelvic floor conditions. This highlights a broader pattern of inconsistency across care pathways.
Cultural approach to symptoms
Women and clinicians both discussed that clinicians might dismiss the symptoms of a postnatal prolapse. This was due to a combination of women not being listened to and symptoms not being acknowledged.
‘…the GP didn’t even consider it to be a problem, an issue, it was just like, you know, that’s what you are stuck with now, almost get on with it, carry on.’ (woman 2)
Due to dismissal, women and clinicians reported frustration and a delay to accessing treatment.
‘…so it’s taken [the woman] like three years, so her baby’s…, so nearly four years and yeah that’s a shame really. And she’s quite nonchalant about it, she accepts the way things are but that’s been a frustrating process for me, because you see them again, you think oh gosh you are in the same situation really and you’ve seen three consultants.’ (physiotherapist 7)
This demonstrates a recurring pattern of how symptom dismissal postpones diagnosis and leads women to internalise their symptoms as something to put up with.
Women discussed a lack of ongoing care for postnatal prolapse symptoms and resorted to treatment in the private sector. Requests from women for referral to a specialist was declined. Clinicians discussed not all conservative treatments are offered to postnatal women as a vaginal pessary was thought to be offered only to older women.
‘…they won’t necessarily be offered a pessary because I think that people, that GPs still unfortunately, don’t consider pessaries for younger women, they think they’re an old woman thing.’ (nurse 8)
This quote highlights how clinicians’ norms and assumptions determine the choice of treatment options for women.
Sometimes clinicians justified dismissal of symptoms as this was thought to normalise and help women cope with their symptoms.
‘…sometimes I just give a lot of reassurance to women, that you know, “this will get better, you’ll feel better soon, it’s the early stages…’ (GP 4).
Both women and clinicians discussed a lack of importance given to prolapse symptoms in the context of women’s health and postnatal care. This resulted in women not receiving the correct care.
‘…but then the referral was kind of shoved under the carpet and again I’m still expecting a letter to come through to say oh you’re going to start some physio, but I’ve done it myself [self-referral] (woman 5)
The ideal care pathway
Women discussed the importance of receiving care with clinicians with expert knowledge and experience. However, a barrier perceived by clinicians involved in these interviews was a lack of training in pelvic health conditions.
‘It’s a shame that there is no formal qualification that more GPs could do to feel more confident with pessary fit, you know and assessing postnatal prolapse symptoms’ (physiotherapist 4).
As a result of this training deficit, women reported frustration at needing to research and read guidelines to request treatments for postnatal prolapse.
‘…I did an eConsult form and it was the usual, “oh I don’t know because you are breastfeeding”…I then went to read the [pessary] guideline and you can have topical oestrogen if your breastfeeding….so then they were fine with that’ (woman 2).
These quotes from women and clinicians show an awareness of inadequate care pathways.
Health literacy and education for women
Women and clinicians frequently discussed health literacy and education for women. Some clinicians generally felt the ability to find, understand and use information about prolapse was poor and this impacted on women’s ability to make healthcare decisions and access timely treatment.
‘…and there is a separate amount of women who probably don’t know they have a problem or don’t seek help as they don’t know it’s a thing’ (physiotherapist 6).
Both women and clinicians commented on the poor quality of pelvic health education. This was thought of as a barrier to accessing care due to a lack of knowledge on available treatment.
‘…there’s my pessary this and that and the other group when they’ve got a prolapse. I follow a few groups just out of interest to see what the chat is….I just think some of their comments are rubbish and I just think oh I’m not too sure about that’ (nurse 8).
Suggestions for improvements to health literacy and education for women included both clinician and women-led activities. The suggestions for clinician-led education included professional networks, monitored social media and education around correct vaginal anatomy after birth.
‘…maybe we need to have that conversation, you know, it [the vagina] might look wider, as long as you can still squeeze and the length will be the same and it does all this brilliant work and look what it has done, maybe that’s the expectation of it’s not going to be the same, but it should feel ok and it should still work’ (physiotherapist 6).
Other facilitators suggested by women to improve women’s health literacy included seeking information from peers and an aspiration for informal in person group forums to discuss symptoms.
‘I went to this toddler group…and then everyone was talking about it, there were eight women in that room with prolapses and they all felt amazing talking about it…there needs to be more knowledge, open discussions about it is common but not normal and we can do something about it’ (woman 2).
These extracts demonstrate a patterned need for extra knowledge, however the clinician perspective shows a gap of knowledge around normal vaginal anatomy, while women identified a lack of shared narratives and peer support to understand their own postnatal experiences.
Clinical pathways
There were several barriers from a clinicians perspective relating to clinical pathways. Barriers were discussed in primary and secondary care pathways.
Primary Care
Barriers for women accessing care included a lack of incentive for GP surgeries to fit pessaries. Often clinicians discussed this led to a referral to secondary care and therefore delayed accessing treatment.
‘…I said I’d be happy to do some training and support all that sort of stuff but the information that came back was that GPs do it [pessary management] if they want to do it, but they are not obliged to…’ (nurse 8).
Across the interviews it was highlighted that the provision of necessary equipment in primary care was lacking, leading to more secondary care referrals and further delays in accessing treatment as the prolapse could be managed in the community.
‘…there wasn’t anything I could do, I said “we could try a ring pessary but it’s not really going to stay up there, …I think you just need to go [to gynaecology] and that was before they had a 2-year waiting list’ (nurse 3).
Secondary Care
Many clinicians discussed that current clinical pathways in secondary care were not designed for younger women with prolapse. Waiting lists in secondary care were reported to be long with no fast-track option. Moreover, doctors offering pessary management did not have time to teach pessary self-management. This often led to multiple appointments with different clinicians.
‘… so, I had this lady I was telling you about, who’s seen three consultants, she was given a cube [type of pessary] in the bag, in the sterilised bag to go away with, and she hasn’t got a clue, so we [physiotherapists] taught her to remove and insert and how to manage it…’ (physiotherapist 7).
The geography of secondary care clinics in rural areas was discussed generally as a barrier for women accessing care by both women and clinicians.
‘…we have some clinics in the north because it’s a rural area and they are not bustlingly full like you might think, but we do have two days a week in X but there is still a lot of travelling about. Personally, I’d rather go and see the right person than see someone on your doorstep who wasn’t the right person…’ (physiotherapist 6).
There were many considerations of clinical pathways that facilitated access to safe and effective care. Self-referral, timely appointments, female clinicians, and flexible appointment slots for childcare were thought of as helpful for women accessing care.
‘…I think making sure we have appointments throughout different times of the day, you know, so they are maybe before school pick up or it might be easier to come in the school holidays because they have already organised childcare’ (GP 1).
These quotes highlight systemic constraints in both primary and secondary care, but also demonstrate the facilitators identified by participants are transferable across both settings. This reinforces the broader pattern of inadequacy within existing pathways and links directly to the previous ‘ideal care pathway’ theme.
Discussion
This is the first study investigating the barriers and facilitators for postnatal women accessing treatment with pelvic organ prolapse from a clinicians’ and women’s perspectives. Five themes were generated in relation to the aims of this study: screening, cultural approaches to symptoms, the ideal care pathway, health literacy and education, and clinical pathways.
We found health literacy and education as barriers for women accessing care for prolapse. This is consistent with previous evidence.25-27 This was identified by both clinicians (‘…maybe we need to have that conversation, you know, it [the vagina] might look wider, as long as you can still squeeze and the length will be the same) and women in this study (…and then everyone was talking about it, there were eight women in that room with prolapses and they all felt amazing talking about it), with different solutions. Early identification and intervention for pelvic floor dysfunction is important 14 and hindered by a lack of awareness, as highlighted by clinicians in this study (…and there is a separate amount of women who probably don’t know they have a problem or don’t seek help as they don’t know it’s a thing). Early identification is crucial for postnatal women to prevent deterioration in pelvic floor dysfunction in the future. Suggested improvements from women included the creation of informal forums or groups, and professional network-led social media posts. Women and clinicians both discussed the importance of screening for pelvic health conditions. A vaginal examination is preferable to identify a prolapse, however due to limited GP resources this may not always be possible. Routine direct questioning about the prolapse in the postnatal appointment and using other opportunities at other women’s health appointments (such as smear tests) have been suggested as suitable opportunities for this health promotion. This is consistent with previous literature which has highlighted the potential for pelvic health information being delivered at GP visits, smear tests and community nurse visits. 27
Following the COVID-19 pandemic, like many clinical care pathways in the UK, women with prolapse often experience long waiting times. 28 As a result, many women will delay or alter plans to complete their family as they have ongoing concerns about future pregnancies and birth. 12 This can cause extra psychological burden. Dismissal of symptoms is a recurrent theme in prolapse management.12,14,29 We found further evidence to support this as this was consistent with the women’s reports in this study (the GP didn’t even consider it to be a problem, an issue, it was just like, you know, that’s what you are stuck with now, almost get on with it, carry on). Interestingly, clinicians in this study justified dismissal as a method to normalise symptoms to help women cope with postnatal prolapse. However, a recent study has suggested normalising pelvic health symptoms after childbirth, could negatively impact on women’s health seeking behaviour in the future and adherence to conservative treatments. 30 This greatly impacts the care women receive. Normalising pelvic health conditions after childbirth has a two-fold consequence. Firstly, clinicians will not offer treatment and secondly, women will not return if symptoms do not resolve.
Women in our study highlighted a lack of confidence in the knowledge of primary care clinicians due to lack of training and knowledge around prolapse management. This perception is supported elsewhere in the literature.31,32 Other studies have found a link between untrained clinicians and poor cultural attitudes to prolapse symptoms. Previous literature has also highlighted that untrained or less-knowledgeable clinicians are likely to trivialise symptoms. 33 This clearly has implications for women accessing treatment. This supports the concept younger women with prolapse need to be treated by the ‘ideal clinician’ to improve access to care, but also the importance of woman having positive healthcare seeking behaviours in pelvic health later in life.
Our study has strengths including a robust approach to analysis and the inclusion of multiple perspectives from both service users and professionals. The interpretive nature of reflexive thematic analysis enabled deeper insight and rich descriptions of a complex condition. Although, participants were not sampled according to geography, there was an equal mix of participants in rural (n=4) and urban (n=4) areas. This has provided insight into the barriers women encounter who live in areas with poor links with public transport. This should be taken into consideration in clinical pathway design. We were also able to represent the views of clinicians working in the public and private sector. This has highlighted socioeconomic and equity issues in women’s health and needs to be addressed when designing future clinical pathways. Furthermore, this research has generated insights into the problems postnatal women have accessing care and adds further depth to this narrative. However, there are limitations. Firstly, women who are most bothered by a healthcare experience are more likely to be willing to take part in research. Challenges exist in recruiting postnatal women to research studies. The barriers identified in our study could relate to this challenge (cultural approaches to symptoms and health literacy and education) and future research should consider these. Clinicians are also more likely to take part in research with an interest in women’s health. This study was conducted in a high-income country, 34 and self-referral options were found as a facilitator to accessing treatment. However, self-referral is seen as a barrier for women seeking treatment for prolapse in lower-middle income countries. 35 This suggests a juxtaposition in access and self-referral options, between high and lower to middle income countries which needs careful consideration when interpreting the results of this study. The interview participants included two women and six clinicians. This is an imbalance of service users and professionals and may influence the depth of ‘cultural approach to symptoms’ and ‘health literacy’ themes. All participants were recruited from the south of the UK; therefore the findings may not be generalisable to other locations. Further research is required to determine if the identified barriers and facilitators are consistent across the UK.
Our findings suggest postnatal women experience a lack of treatment options due pessary management being associated with older women. The NICE guidelines for urinary incontinence and prolapse 17 state a vaginal pessary is a treatment choice, however this is not being offered as a treatment option for all women.
This research suggests that a review of existing clinical pathways for postnatal women with prolapse is urgently needed, alongside the development of effective, pro-active care pathways. The findings of this research suggest that future service models should include screening and training for clinicians into consideration.
Conclusions
This study aimed to explore the perceived barriers and facilitators of accessing conservative treatment for prolapse for postnatal women. In relation to this we found five key themes. Our findings suggest cultural approach to symptoms is limiting younger women’s choices in prolapse management. Improvements in health literacy and screening are required. Future work examining optimal pathways of care for this patient group is urgently needed, alongside research into effective treatments for the management of prolapse in postnatal women.
Footnotes
Acknowledgements
We would like to acknowledge The Typing Works transcribing company for their professional service. We would also like to thank the PPIE Steering Study group for generation of the interview prompt guide and the participants who were interviewed for this study.
Ethical Considerations
Ethical approval was granted by Liverpool Central Research Ethics Committee (24/NW/0016).
Consent to Participate
Consent to participate was written.
Consent for Publication
Consent for publication was written and part of the consent procedure. Consent for publication was provided by the participant via consent forms
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was received from Addenbrookes Charitable Trust, grant number 900414 and by the Wellcome Trust, grant number 341539/Z/25/Z.
Declaration of Conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joanne McPeake: JM’s institution receives consultancy fees from Astrazenecca.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author (CB) upon reasonable request.
*Caroline Zwierzchowska-Dod has now moved institutions to Central East ICB, Gemini House, Bartholomew's Walk, Cambridgeshire Business Park, Angel Drove, Ely, Cambridgeshire CB7 4EA.
Appendix 1
Consolidated Criteria for Reporting Qualitative Studies (COREQ) 32-item Checklist
No. Item
Guide questions/description
Reported on page #
Personal Characteristics
1. Inter viewer/facilitator
Which author/s conducted the interview or focus group?
7
2. Credentials
What were the researcher’s credentials? E.g. PhD, MD
1
3. Occupation
What was their occupation at the time of the study?
1
4. Gender
Was the researcher male or female?
1
5. Experience and training
What experience or training did the researcher have?
7
Relationship with participants
6. Relationship established
Was a relationship established prior to study commencement?
n/a
7. Participant knowledge of the interviewer
What did the participants know about the researcher? e.g. personal goals, reasons for doing the research
6
8. Interviewer characteristics
What characteristics were reported about the inter viewer/facilitator? e.g. Bias, assumptions, reasons and interests in the research topic
Not reported
Theoretical framework
9. Methodological orientation and Theory
What methodological orientation was stated to underpin the study? e.g. grounded theory, discourse analysis, ethnography, phenomenology, content analysis
7
Participant selection
10. Sampling
How were participants selected? e.g. purposive, convenience, consecutive, snowball
6
11. Method of approach
How were participants approached? e.g. face-to-face, telephone, mail, email
6
12. Sample size
How many participants were in the study?
7
13. Non-participation
How many people refused to participate or dropped out? Reasons?
n/a
Setting
14. Setting of data collection
Where was the data collected? e.g. home, clinic, workplace
5
15. Presence of non-participants
Was anyone else present besides the participants and researchers?
no
16. Description of sample
What are the important characteristics of the sample? e.g. demographic data, date
Table 1
Data collection
17. Interview guide
Were questions, prompts, guides provided by the authors? Was it pilot tested?
S1
18. Repeat interviews
Were repeat inter views carried out? If yes, how many?
no
19. Audio/visual recording
Did the research use audio or visual recording to collect the data?
7
20. Field notes
Were field notes made during and/or after the inter view or focus group?
no
21. Duration
What was the duration of the inter views or focus group?
7
22. Data saturation
Was data saturation discussed?
7
23. Transcripts returned
Were transcripts returned to participants for comment and/or correction?
no
Data analysis
24. Number of data coders
How many data coders coded the data?
2
25. Description of the coding tree
Did authors provide a description of the coding tree?
no
26. Derivation of themes
Were themes identified in advance or derived from the data?
9
27. Software
What software, if applicable, was used to manage the data?
n/a
28. Participant checking
Did participants provide feedback on the findings?
no
Reporting
29. Quotations presented
Were participant quotations presented to illustrate the themes/findings? Was each quotation identified? e.g. participant number
9-18
30. Data and findings consistent
Was there consistency between the data presented and the findings?
9-18
31. Clarity of major themes
Were major themes clearly presented in the findings?
9-18
32. Clarity of minor themes
Is there a description of diverse cases or discussion of minor themes?
n/a