
Abstract
This is the case of a 67-year-old immunocompetent Hispanic male residing in Mexico who presented with acute right lower back and right lateral thigh pain. Initial imaging was unremarkable. He later developed painful vesicular lesions on the right foot and buttock. He was diagnosed with herpes zoster and initiated acyclovir and gabapentin. Ten days later, he developed foot drop, leg weakness, and urinary incontinence. Magnetic resonance imaging (MRI) showed enhancement of the cauda equina, and electrodiagnostic studies demonstrated right lumbar polyradiculopathy. The patient improved significantly with pain medications and physical therapy. After 8 months of physical therapy, he demonstrated significant clinical improvement. This case highlights the uncommon presentation of motor involvement in herpes zoster and emphasizes the role of imaging and electrophysiology in guiding diagnosis and management.
Keywords
Background
Herpes zoster (HZ) develops in approximately 30% of the United States population. 1 The risk of developing shingles increases with age and with the weakening of the immune system. The clinical manifestations of HZ are typically benign, characterized by a cutaneous vesicular rash and neuropathic pain localized to the affected dermatomes. 2 However, complications of HZ can be debilitating and significantly interfere with daily activities. The most common complications include postherpetic neuralgia, HZ ophthalmicus, HZ oticus, and encephalitis. A less common but clinically significant complication is nerve root involvement, which occurs in 0.5-5% of all shingles cases.3,4 Here, we present an uncommon case of polyradiculopathy secondary to varicella zoster virus reactivation.
Case Presentation
A 67-year-old immunocompetent Hispanic male from Mexico with a past medical history of atrial fibrillation, pericarditis, L3 laminectomy, and ulcerative colitis without active disease and not receiving immunosuppressive therapy, on treatment with apixaban 5 mg twice daily, mesalamine 400 mg three times daily, and rosuvastatin 20 mg daily, who developed right leg pain and weakness 1 month prior to our visit while he was in Mexico, initially starting as low back pain radiating to the right buttock and thigh, that was progressively getting worse. The patient smoked 1-2 packs per day for 5 years during adolescence. He drinks 1-2 alcoholic beverages daily, with no illicit drug use. He was not immunized against HZ. He was evaluated two days after the onset of the symptoms in the emergency department in Mexico, where a lumbar spine MRI was obtained due to severe pain and was unremarkable at that time.
He developed a burning sensation on the arch of the right foot, and painful vesicular lesions on the right plantar surface and buttock, which eventually progressed over the right lateral lower leg and toes. The patient was diagnosed with HZ by a local dermatologist and referred to local neurologist in Mexico who initiated acyclovir 800 mg daily, and gabapentin which he started approximately 1 week after the onset of the burning sensation and the vesicular rash.
Ten days after being diagnosed with HZ, the patient experienced sudden-onset foot drop and right lower extremity weakness with reduced sensation and numbness over the right lateral lower leg, dorsum of the foot, and toes, accompanied by worsening pain, urinary urgency, and incontinence. He received parenteral dexamethasone, which provided relief from the pain. Neurologic evaluation in Mexico did not reveal a clear cause for the acute right lower limb weakness. He was treated with various neuropathic pain medications, including carbamazepine, gabapentin, pregabalin, tramadol, paracetamol, and amitriptyline, without significant improvement of neuropathy. He continued taking acyclovir for 4 weeks after diagnosis of HZ.
On examination at our institution, he had a healing vesicular rash over the right buttock and the plantar surface of the right foot. Neurological examination revealed decreased light touch sensation over the lateral aspect of the distal right lower leg and dorsum of the right foot and toes, mildly reduced hip flexion, thigh abduction, knee flexion, plantar flexion, and toe flexion; and severe dorsiflexion, toe extension, eversion, and inversion weakness, right lower limb areflexia, and a right-sided steppage gait. The patient reported improvement in his urinary symptoms, with no incontinence or urgency over the past week, and the acyclovir was discontinued after 4 weeks, due to no clear benefit to extending therapy for more time.
Laboratory results included a complete blood count, inflammatory markers (C-reactive Protein, erythrocyte sedimentation rate, ferritin), blood glucose, hemoglobin A1c, creatine kinase, antinuclear antibodies, aldolase, vitamin B12, folate, syphilis serology, QuantiFERON TB Gold plus assay, Lyme, and arbovirus serologies, and thyroid-stimulating hormone were all within normal limits. Colorectal biopsies showed benign colonic mucosa without active inflammation, negative for dysplasia.
Lumbar spine MRI demonstrated enhancement of the right cauda equina, most prominently the L4 and L5 nerve roots, with lesser enhancement of other lumbar roots, findings consistent with polyradiculitis and multi-level degenerative changes were also noted (Figure 1). Nerve conduction studies showed low-amplitude fibular motor and superficial fibular sensory responses with slow fibular motor nerve conduction velocity. Needle electromyography (EMG) demonstrated active denervation in the iliopsoas and more severely L5 innervated muscles, no or minimal activation of proximal and distal L5 innervated muscles, and milder findings of reduced recruitment with large motor unit potentials in the iliopsoas and vastus lateralis muscles. Electrodiagnostic studies were consistent with either multiple lumbar radiculopathies or patchy lumbosacral plexopathy. (A) sagittal (T-12 level); (B) sagittal (L-2 level); (C), pre-contrast axial (T-12 level) T1-weigthed compared to (D), axial (T-12 level) T1-weighted post-gadolinium. Fat saturation images show enhancement of the cauda equina nerve roots extending inferiorly (arrows). Findings consistent with polyradiculitis in the cauda equina, involving the right L4 and L5 nerve roots. Degenerative changes are also present. Multilevel disc desiccation is present from L1-L2 through L4-L5 levels. There is intervertebral disc space collapse at L3-L4 and L4-L5 with associated Schmorl’s nodes and Modic type II endplate reactive changes. Minimal retrolisthesis is present at L1-L2, L2-L3, L3-L4, and L4-L5 levels. Mild facet arthropathy is present at L3-L4, and L4-L5 levels. The spinal canal is widely patent throughout the lumbosacral spine
Differential Diagnosis
The initial diagnosis considered at presentation was lumbar radiculopathy, given the prior history of L3 laminectomy in 2016. Alternative causes of possible nonstructural neuropathic conditions, such as inflammatory, metabolic, autoimmune, infections, or demyelinating disorders associated with this presentation, were also considered. Laboratory evaluations included creatine kinase, aldolase, vitamin B12, folate, syphilis serology, QuantiFERON TB Gold plus assay, Lyme, and arbovirus serologies, and thyroid-stimulating hormone levels. Results were all within normal limits.
Outcome and Follow-Up
A diagnosis of HZ-associated polyradiculitis was established. The patient was referred to outpatient physical therapy, which he performed daily, six times per week. At the eight-month follow-up visit, the patient showed marked clinical and radiographic improvement. He can perform daily activities without limitation, although mild residual weakness, sensory loss, and pain persisted. The patient reported no bladder dysfunction or urinary symptoms (Figure 2). Repeat lumbar spine MRI demonstrated near-complete resolution of the previously noted nerve root enhancement. Clinical timeline of herpes zoster (HZ) related polyradiculitis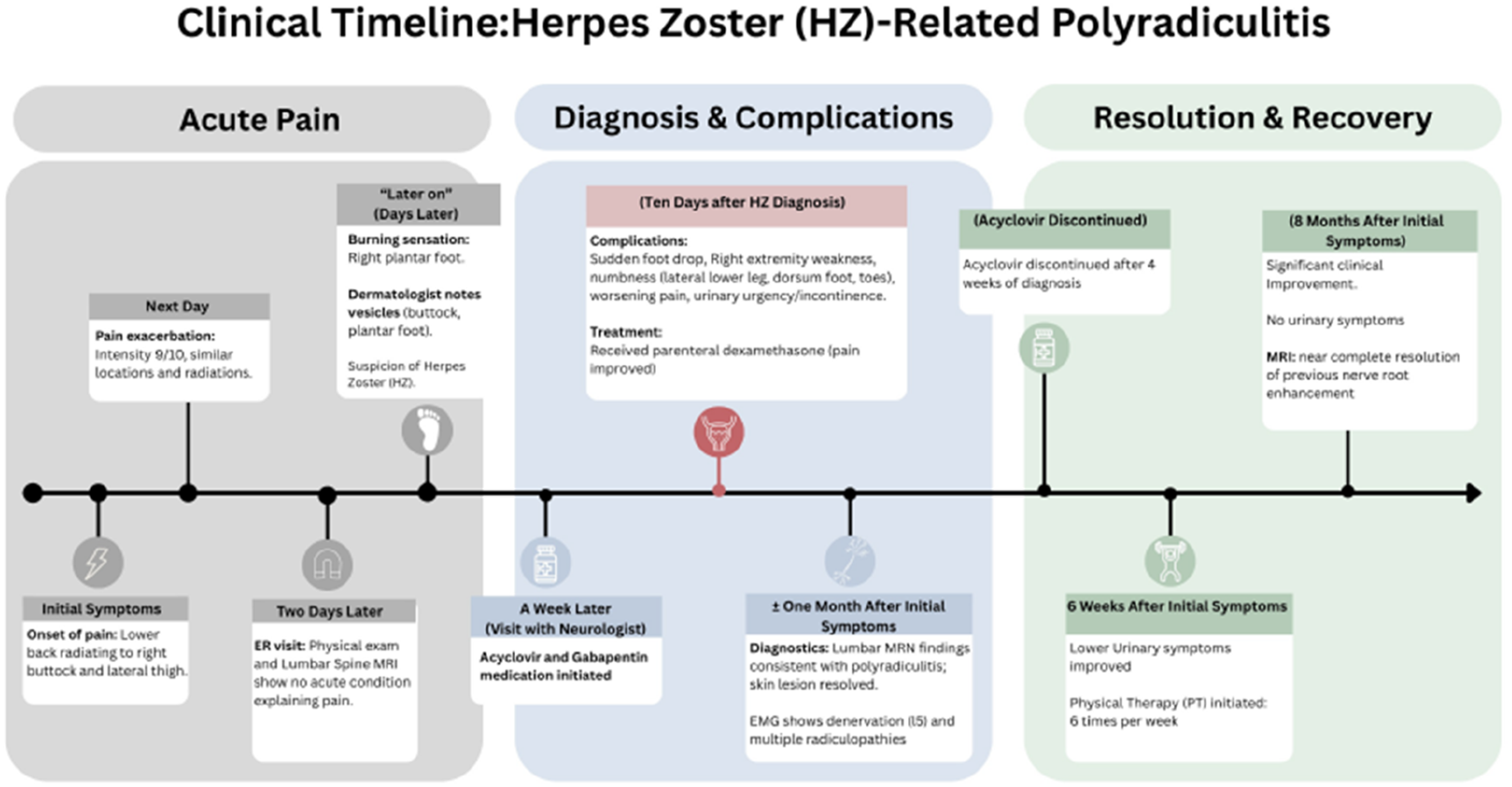
Timeline illustrating the onset of signs and symptoms and the development of complication (red box), including progression to foot drop and urinary incontinence (cauda equina-like symptoms), marking the transition from shingles to polyradiculopathy. The figure also summarizes the diagnostic workup, therapeutic management, and recovery.
Discussion
This case illustrates the diagnostic challenges caused by motor complications of HZ, particularly when initial symptoms mimic those of common structural etiologies. Our patient was diagnosed with HZ-associated polyradiculitis after electrodiagnostic studies showed patchy active and chronic denervation, with no underlying mechanical cause detected on imaging. Notably, nerve root enhancement on MRI was observed 1 month after symptoms began, highlighting the diagnostic challenges posed by the delay in motor and autonomic manifestations of HZ.
After primary infection with varicella zoster virus (VZV), the virus remains latent in the dorsal root ganglia, where it is susceptible to reactivation and subsequent development of HZ (shingles). Reactivation of the VZV is known to result from a decline in cell-mediated immunity, which occurs naturally with aging in otherwise healthy individuals or in immunocompromised individuals.2-4 Prior to the advent of the varicella vaccine, more than 95% of the general population had been exposed to VZV. Following the introduction of the vaccine approximately thirty years ago, the incidence of varicella (chickenpox) has decreased by 80%.2,5 Nonetheless, vaccinated individuals remain at risk of developing shingles. Although HZ is considered a benign condition that manifests as a vesicular rash limited to the affected dermatome, it can lead to significant and sometimes debilitating complications that often require a multidisciplinary approach to manage symptoms and sequelae. 3
Motor deficits in HZ are believed to result from the spread of inflammation from the dorsal root ganglia to the anterior horn cells or ventral roots, disrupting the blood-nerve barrier and affecting motor neuron function. 6 Beyond immunosuppression, it is unclear what predisposing factors put a person at risk for motor complications in HZ. In a Japanese review of 1432 patients with HZ, 12 patients developed motor symptoms within 7 days of the appearance of the cutaneous rash. All affected individuals were older than 60 years, except for one immunosuppressed patient in his forties. This study suggested that muscle weakness related to HZ may be more common than we think. Almost 50% were affected by thoracic dermatomal distribution, in which clinical muscle weakness may be less evident than in regions such as the cervical or lumbar spine. EMG studies have shown denervation of the muscles corresponding to affected myotomes, suggesting the true motor involvement in HZ may be underestimated. 7
Our patient’s lumbar pain was initially mistaken for structural nerve root compression due to the time lag between neuropathic pain and skin manifestations of shingles. These intervals in time are also seen with the appearance of motor symptoms. In our patient, there was a 10-day interval between the onset of cutaneous rash and the subsequent development of right leg weakness. In other cases, reported intervals have ranged from 2 days to 6 weeks.6-8 This might be related to the severity of inflammation in the dorsal root ganglia, involving the ventral roots, with the subsequently spread to the cauda equina resulting in foot drop, urinary urgency, and incontinence. There have been HZ cases in the literature describing the sacral nerve root involvement, causing urinary dysfunction such as urinary retention and incontinence due to detrusor areflexia and hyperreflexia, respectively.9,10
This patient eventually started appropriate therapy with acyclovir; however, treatment could have been initiated after neuronal inflammation, leading to the onset of motor symptoms. While antiviral therapy is initiated within 72 hours of skin lesions, treatment is recommended as early as possible to reduce the severity, duration of disease, and the risk of neurologic complications.11,12The efficacy of oral acyclovir on motor paresis and postherpetic neuralgia was evaluated in a study of 105 patients with HZ. Forty-seven patients were treated with acyclovir for 1 week and later assessed the dermatomes affected by sensory and motor nerve conduction studies and EMG, showing reduced electrophysiologic nerve damage and decreased incidence of motor involvement in patients in the treatment group. In this study, oral acyclovir limited ganglion damage and reduced the possibility of viral spread to the ventral roots and spinal motoneurons, lowering the incidence of segmental motor neuritis. 13
Our patient had not received the shingles vaccine. Although vaccination reduces the incidence and severity of HZ, there is no clear data demonstrating the benefits of the shingles vaccine against motor complications. 14 The administration of glucocorticoids (e.g., prednisone, prednisolone) in the treatment of HZ remains debated. Randomized controlled trials have been associated with reduction of acute pain, improvement of quality of life, and in one study, a shorter time to complete healing, although results are inconsistent. Glucocorticoids should not be used without antiviral therapy because of their immunosuppressive effects.11,15 Notably, the patient had a favorable response to dexamethasone therapy, without clear aggravation of his symptoms, making the possibility of refractory infection lower.
This case highlights the importance of understanding the natural history of diseases, specifically, the significance of the sequence of events in HZ. While imaging is important for ruling out mechanical etiology, electrodiagnostic studies are essential for establishing a diagnosis of HZ-related radiculopathy. It is also worth mentioning that we did not identify any predisposing factors to postherpetic radiculopathy. We recommend further investigations to determine which factors may increase susceptibility to, or protect against, this condition.
Conclusion
Radiculitis secondary to HZ should be considered in the differential diagnosis for patients presenting with radiculopathy. Electrodiagnostic studies may be considered in patients diagnosed with cutaneous HZ to identify potential underlying neuropathic sequelae. Shingles vaccination should be offered for all patients aged 50 years and older who have not been immunized against HZ. Patients should be monitored for radicular involvement, including weakness, as a complication of HZ.
Footnotes
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing does not apply to this article as no new data was created in this study.
Patient Consent
No written consent has been obtained from the patient as no patient-identifiable data was included in this case report.