
Abstract
Background
Access to credible health information is critical for health literacy and informed health behaviors. Although digital platforms are widely used, limited technology access and lower eHealth literacy may constrain online health information seeking in some communities. Black and low-income individuals, in particular, may rely less on internet-based sources and more on in-person channels, including social networks and community-based organizations.
Aims
This study examined community-based sources of health information used by Black individuals living in a low-income, urban area.
Methods
Semi-structured interviews (n = 27) completed 4-weeks post a community education program were transcribed verbatim. Of these, interview transcripts (n = 25) that identified sources of health information or advice were included in the analytic sample. Two coders categorized responses describing sources of health information and advice using inductive content analysis.
Results
Heath information sources that were identified included health care services, community organizations and networks, media, national organizations, commercial pharmacies, and workplaces. Health care services were most frequently cited, with over half of participants naming physicians, clinics, hospitals, insurance carriers, or other providers, followed by community organizations and networks.
Discussion
Black individuals in low-income, urban areas access health information through diverse in-person and media-based sources. Identifying trusted and accessible community channels can inform targeted outreach efforts to improve health literacy and reduce health disparities.
Keywords
Introduction
Access to credible sources of health information is central to health literacy which is linked to better decision making and health outcomes. 1 Individuals are often comfortable using the internet to learn more about general health concerns and how to improve health behaviors.2,3 While those living with chronic illnesses tend to rely more on health care professionals, the internet still serves as a supplementary source of information.4,5 Although searching for and consuming health information has become simple in the digital age, 6 the digital divide still leaves some with inadequate access to online health information. 7 Indeed, socio-demographic factors such as race, socioeconomic status, and age influence internet access and usage to gather health information.7,8 For example, low-income individuals engage in online health seeking behaviors less often, even when reporting consistent access to the internet and technology. 9 Consequently, many people rely on alternative sources of health information.
Health literacy and discernment is of particular importance for Black individuals, defined in this study as individuals who reside in the US and self-identify as Black, including individuals of diverse ethnic and cultural backgrounds within the African diaspora. This is due to the high prevalence of common complex diseases such as heart disease, diabetes, and cancers in this population.10,11 When examining information seeking behaviors among Black Americans, research demonstrates that Black individuals seek health information through more outlets than their white counterparts, including interpersonal connections with friends, family, and coworkers. 12 Charitable and religious organizations are also trusted as sources of health information at higher rates among racial minorities. 13 These findings suggest that established relationships and trust may influence where Black individuals choose to obtain health information.
While gathering health information online may be efficient, seeking out this information through community organizations can be beneficial due to their knowledge of specific local environmental or social barriers that may inhibit access to or understanding of health information. Community sources of health information, such as community health workers and community education programs, may be better suited for some groups because the information can be tailored and presented in a way that fits the needs of the community. 14 By providing health information, community organizations may fill a health knowledge gap potentially supporting the realization of health for all. 15
Given that low-income individuals engage less in online health seeking behaviors, and Black individuals utilize more interpersonal connections as health information sources, this paper sought to qualitatively examine where Black residents of low-income areas acquire health information. Although prior research has identified patterns in how low-income Black individuals seek health information online, little is known about where they access health information within local community-based settings. These geographically bounded spaces-shaped by ongoing relationships, shared resources, and local institutions-may foster in-person connections that support health information exchange. Knowing where individuals in under-resourced areas gather health information enables health professionals and community leaders to more effectively target outreach efforts, which in turn can lead to increased health equity and help individuals make better health decisions.
Methods
Formative Work
The Families SHARE (Sharing Health Assessment and Risk Evaluation) program aims to educate individuals on the importance of Family Health History (FHH) and its use in estimating risk for five common, complex conditions: heart disease, type 2 diabetes, breast cancer, colon cancer, and prostate cancer. Additionally, the Families SHARE program provides information on how individuals can reduce their disease risk through modifiable health behaviors (e.g. diet, physical activity, preventative screenings, etc.). Originally Family SHARE was comprised of an educational workbook and personalized pedigree. 16 Evaluations of the Families SHARE workbook in low-income Black communities found that participants effectively used the workbook to calculate their own risk for disease based on their FHH and had engaged in FHH sharing and gathering behaviors in order to get an accurate representation of their FHH. 17 However, it was also found that many participants had inaccurate beliefs about developing diseases, even after accurately calculating their risk for those diseases. Additionally, the Families SHARE workbook was not successful in increasing participants’ intention to change modifiable health behaviors that would reduce their risk for disease. 17 In response, a community education program was developed to guide participants in using the materials, providing an opportunity to ask question about FHH and the workbook content, and enabled discussion of strategies for effective FHH communications and heath behavior change. The data for the present analysis was derived from this community education program. This study was approved by the Institutional Review Board at the National Institutes of Health (000164).
Participants
Demographic Data of Participants Who Competed the Semi-Structured Interviews
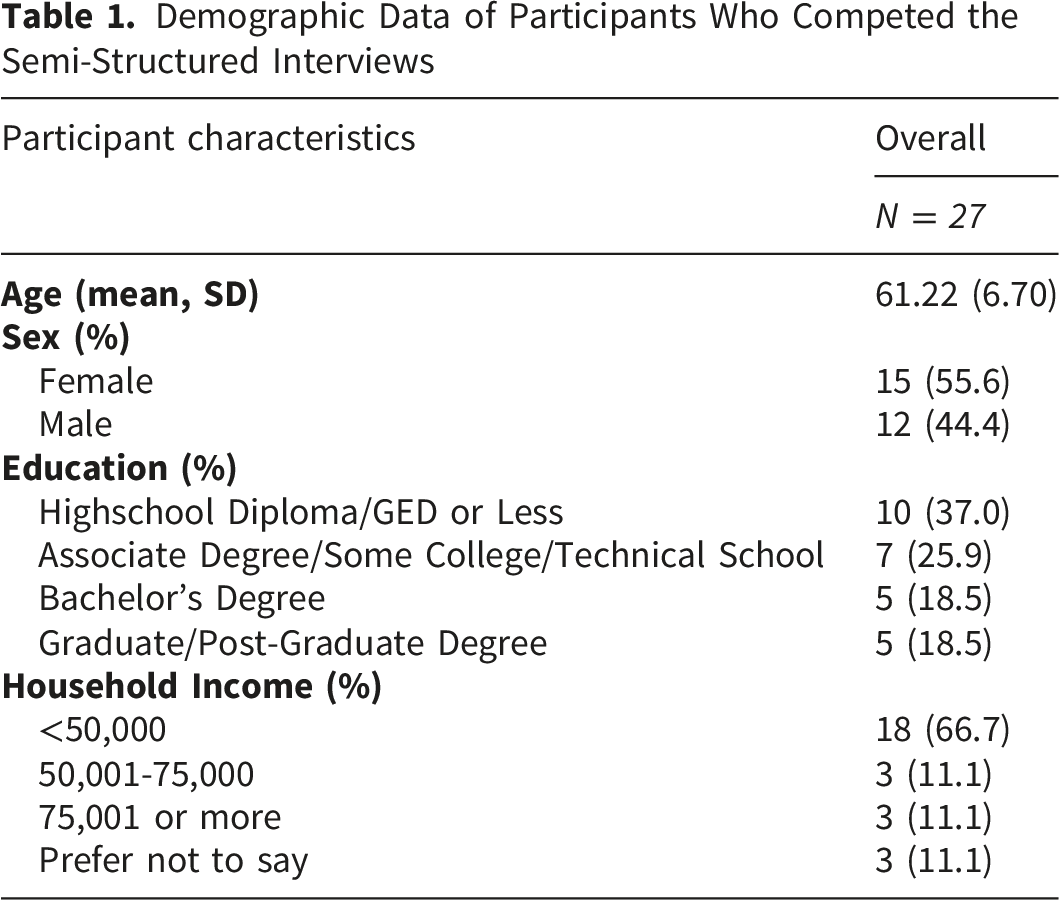
Procedures
During an initial phone call, participants provided verbal informed consent and completed a baseline survey. Participants were then mailed the previously developed Families SHARE workbook and a personalized pedigree created using the baseline data. Participants subsequently attended a virtual community education session. Following the virtual community education session, participants were scheduled to complete a telephone-administered follow-up survey with a study staff member. This survey was completed within four weeks of completing the program. A two-week window for completing the follow-up survey was established to accommodate participant and staff availability. On average, the follow-up survey was completed 23 days after the education session. Participants were then invited to participate in an optional semi-structured interview, which is the basis of this analysis. All study procedures, including the semi-structured interviews, were conducted by a female postdoctoral fellow with an advanced degree in public health. Before each assessment, participants were reminded of the goals of the study.
Measures
Baseline and follow-up surveys were administered by telephone due to concerns that some participants would not have reliable access to computers, smart-devices, or internet. The baseline survey collected socio-demographic information and assessed health behaviors and intentions, familiarity with health-related terms, beliefs about disease risk and development, FHH communication patterns with family and physicians, and concerns about COVID-19, given data collection occurred in 2021. The follow-up survey included items from the baseline survey as well as program evaluation items such as participants’ understanding of the different aspects of the workbook and pedigree, feedback on the community education program, and whether participants shared either the Families SHARE material or their FHH knowledge with family or physicians. With the exception of the COVID-19 related questions, baseline and follow-up surveys were identical to those used in the previous Families SHARE evaluations. 17 Survey responses were entered into Qualtrics by study staff. During the baseline survey, participants also reported their FHH by enumerating their first- and second-degree relatives and if the enumerates had been diagnosed with any of the five diseases of interest. These data were used to generate personalized pedigrees using Progeny software. Community education sessions were conducted via Zoom and audio-recorded to capture participant feedback. Semi-structured interviews were conducted by telephone and audio-recorded. Interviews lasted an average of 25 minutes. For the purposes of this study survey questions were not included in analysis.
Analysis Plan
Audio recordings from the semi-structured interviews were transcribed verbatim and de-identified prior to data analysis. Conventional qualitative content analysis, using an inductive coding approach, outlined by Hsieh and Shannon (2005) 21 was used to analyze participant responses to the semi-structured interview question “Where/who are the main sources of health information or health advice in your community?”. Inductive content analysis is data driven, allowing for open coding, therefore no a priori theory, framework, or coding structure were applied.
Two authors (KJ and RB) independently reviewed all participant responses to become familiar with the data. Using NVivo version 14, each author then conducted open coding of the responses independently, assigning codes to words, phrases, or segments of text that captured distinct concepts of health information sources. After initial coding, the authors compared their codes and discussed code content, code boundaries, and similarities or differences in code definitions and applications. Through this reconciliation process, codes reflecting similar concepts were grouped into broader categories, and subcategories were developed when needed to capture meaningful variation within a category while preserving conceptual distinctions across responses. The coding framework was revised iteratively until consensus was reached on the final set of codes, categories, and subcategories used to characterize participant responses. The semi-structured interview was optional, and therefore the analytic sample consisted of the 27 participants who completed this component. Although data saturation was not formally evaluated, the analysis included the full set of available interview data relevant to the study question.
Results
Categorization and Sub-Categorization of Participant Responses Detailing the Sources of Health Information and Advice Within Their Communities
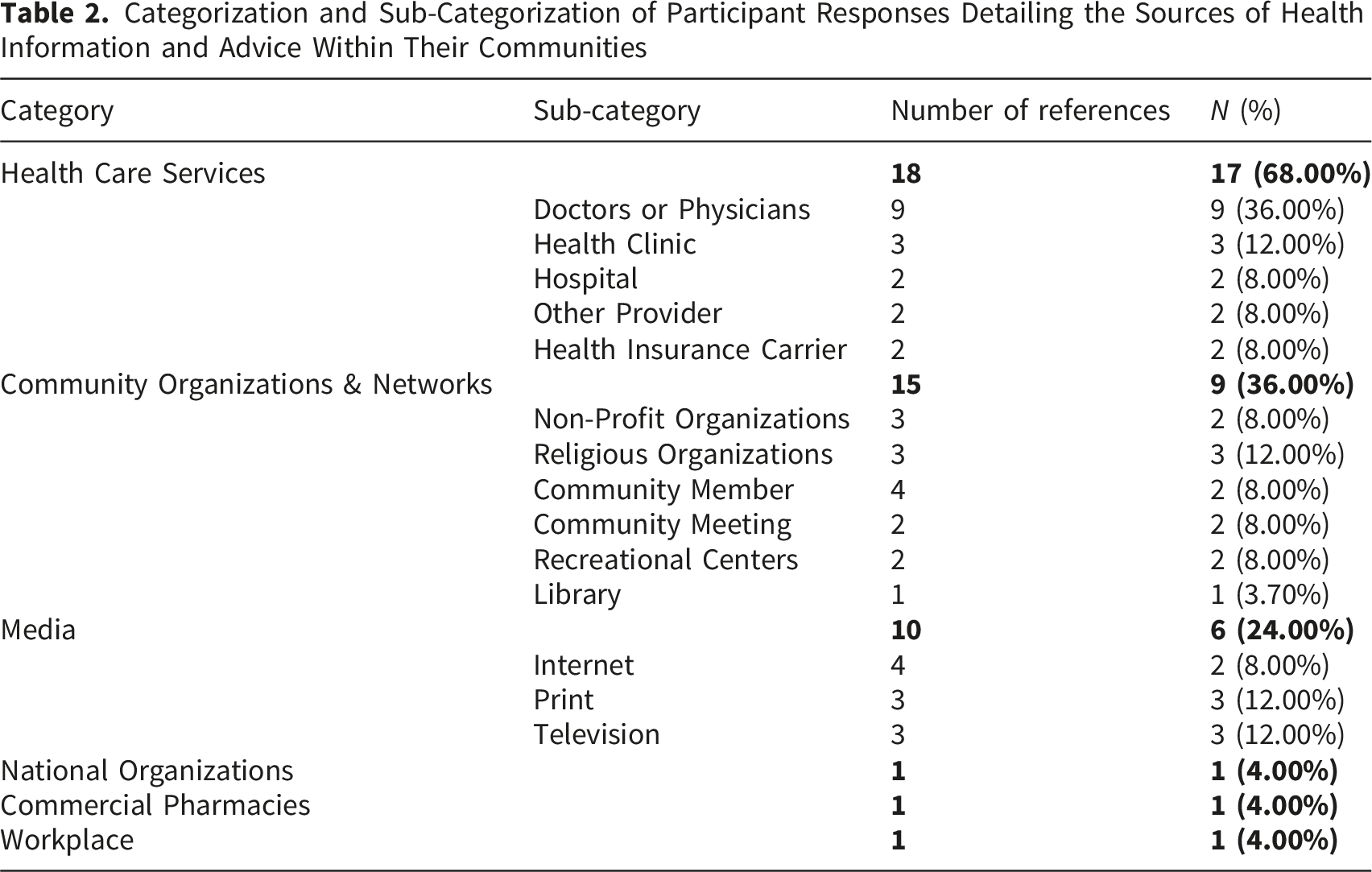
Health Care Services
The category ‘health care services’ was comprised of five subcategories: physicians, health clinics, hospitals, other providers, and health insurance carrier. Health care services were the most referenced sources of health information and health advice in the interview transcripts. Participants utilized these sources of health information when attending health-related appointments, seeking health advice from professionals, and medication access:
“I attend the clinic monthly or whenever I need my prescriptions filled.
Community Organizations and Networks
The category ‘community organizations and networks’ encompassed six subcategories: non-profit organizations, religious organizations, community members, community meetings, recreational centers, and libraries. Participants who sought health information from community organizations used their services for access to healthy food and exercise equipment, health education programs, and health screenings. Regarding community meetings and community members, participants who sought out health information and advice from community meetings often referenced a specific person who was their source of information. In general, the community members were not identified as health professionals; however, they were described as people who advocate for their community, disseminate health information, and host community events: “I actually went through a
Media
The category ‘media’ encompassed three subcategories: internet, print, and television. Although these sources of health information are not embedded in one’s community or neighborhood, participants still referenced them as containing health information and advice. Specific examples of these sources were search engines, brochures and flyers that participants would obtain from community organizations and meetings, the news, and newsletters from academic and scholarly sources: “I do look at
National Organizations, Commercial Pharmacies, and Workplace
Categories that were referenced less frequently were ‘national organizations’, ‘commercial pharmacies’, and ‘workplace’, with one reference in each category. These sources may have been considered community-based by participants because they are embedded in their social networks: “
Discussion
The aim of the current paper was to identify where Black individuals within low-income, urban areas acquire health information and health advice within their defined communities. Understanding local health information access and dissemination can guide community leaders, policy makers, and health professionals on how and where to effectively share important health information within community settings. Findings indicated that Black individuals living in low-income, urban areas may acquire health information from an array of sources, with the majority rooted in health care, community-based organizations and networks, and media.
Health care services were the most frequently cited source of health information, with over half of participants mentioning either health care locations, services, or providers. This commonality in participant responses is likely a reflection of the abundance of health care resources that are available in Washington, DC, and may not be found in areas where health care is less accessible. The reliance on health care services and professionals as a frequent source of health information is encouraging as it suggests community members are receiving accurate health information that is most likely tailored to their specific health needs. Consistent with Hussain et al (2016), participants commonly mentioned hospitals and clinics, highlighting the use of safety-net providers, which may be more accessible for residents without a primary care physician and those needing shorter wait times or broader insurance acceptance. 22
Community organizations and networks also emerged as an important source of health information. The community organizations and networks identified by participants were primarily local to their geographic area and were accessed through in-person interaction. Many of the organizations mentioned offered health-related services in addition to informational support, such as nutrition education and preventive or mental health resources. Although health information dissemination is not the primary mission of many community organizations, community members’ reliance on them highlights their influential role in shaping health knowledge and behaviors. Moreover, the charitable nature of many of these organizations suggests that the services and information provided are often affordable or cost-free. Given well-documented levels of medical mistrust within Black communities, 23 information shared through trusted community institutions and interpersonal networks may be particularly impactful. These findings underscore the importance of strengthening partnerships between health care systems and community organizations to ensure that accurate, culturally relevant health information is disseminated through trusted channels. Future research should further explore how trust, accessibility, and cultural relevance within community settings influence health communication and behavior change.
Media sources—including the internet, television, and print materials—were also frequently cited as avenues for obtaining health information. While these channels can efficiently deliver health information, individuals are more likely to be exposed to misinformation and disinformation through these formats. Although some explicitly mentioned accessing sources that are widely recognized as credible (e.g. CDC, JAMA, Johns Hopkins Newsletter), others more vaguely referenced television, flyers, brochures, and search engines. Given evidence that age and income affect eHealth literacy, 24 there is a growing need to strengthen individual’s capacity to assess the credibility of health content. Enhancing eHealth literacy and reducing the spread of misinformation should be prioritized through coordinated efforts, including community education programs and education courses offered by health care organizations. Such interventions could empower individuals to make better health decisions and reduce the impact of misinformation.
Although the current study primarily discussed in-person community-based sources as those were the sources mentioned most by participants, online communities—including message boards, social media platforms, and chatrooms—are increasingly common in the digital age. Individuals use these online spaces to connect with others who share similar interests or identities, to seek specialized knowledge, and to reach broader audiences. 25 Future research should examine how individuals navigate online communities for health information and how they discern whether health information obtained through these communities is credible.
Limitations
Although the current paper provides important findings on sources of health information within the Black community, there are also several limitations to consider. First, the analysis cannot distinguish whether participants actively sought or passively received health information from the reported sources. In addition, despite having an adequate sample size for qualitative analysis, the sample was homogeneous in nature since all participants were recruited from the same area of Washington DC, limiting generalizability to other geographic and community contexts. Nonetheless, the sample included a relatively high proportion of men, offering insights into health information sources among Black males, a typically hard-to-reach group.
Conclusion
The current paper aimed to identify where Black individuals are acquiring health information within low-income communities of Washington DC. The results revealed that health care services, community organizations and networks, and media were the most frequently cited sources of health information. These findings help give insight into what types of organizations and platforms are reaching the most people, which can better inform community leaders and health workers on where to best engage in community outreach. Leveraging established community organizations and institutions as health information channels could broaden dissemination to a wider audience. Additionally, receiving credible health information from trusted community organizations and members may become increasingly important with the rise of AI-generated information online. Based on these findings, future research should evaluate how individuals prefer to receive health information within community settings, and what types of health information and services are most beneficial to community members.
Supplemental Material
Supplemental material - Health Information Sources Within Low Income Black Communities: A Families SHARE Study
Supplemental material for Health Information Sources Within Low Income Black Communities: A Families SHARE Study by Kristen Judy, Sophia Zuniga, Raegan Bishop, Isabel Cordova Amador, and Laura Koehly in Journal of Primary Care & Community Health.
Footnotes
Acknowledgements
This research was supported by the Division of Intramural Research at the National Human Genome Research Institute, National Institutes of Health (Z01HG20335 to LMK) and through the NIH/NCI Grant P30-CA051008 which supports Georgetown Lombardi Comprehensive Cancer Center’s Community Outreach and Engagement (COE) office. We thank Rhonda Hamilton and Dale Mooney for their recruitment efforts, Dr. Calandra Whitted for her study coordination and data collection efforts, and Dr. Chiranjeev Dash; this study could not have been accomplished without them. We express our gratitude to the participants of this study. This research was supported by the Intramural Research Program of the National Institutes of Health (NIH). The contributions of the NIH authors are considered Works of the United States Government. The findings and conclusions presented in this paper are those of the authors and do not necessarily reflect the views of the NIH or the U.S. Department of Health and Human Services.
Ethical Considerations
The Institutional Review Board (IRB) at the National Institutes of Health (NIH) determined that the study was exempt from full review (IRB study #000164) and approved the informed verbal consent procedures described.
Consent to Participate
Prior to initiating data collection, prospective participants were provided with study information (i.e. procedures, risks, benefits) via a telephone call with a staff member and were given the opportunity to ask questions. After all questions were addressed, participants gave informed verbal consent to participate in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Division of Intramural Research at the National Human Genome Research Institute, National Institutes of Health (Z01HG20335 to LMK) and through the NIH/NCI Grant P30-CA051008 which supports Georgetown Lombardi Comprehensive Cancer Center’s Community Outreach and Engagement (COE) office.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the senior author, LK. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.