
Abstract
Introduction
Correct inhaler technique is of utmost importance in the optimal delivery of therapeutics utilized for respiratory illnesses. Previous research suggests that the ability of both patients and providers to correctly use these inhalers is sub-optimal and is associated with poorer patient outcomes. Further education about inhaler types and technique as part of residency education could serve to correct these trends.
Methods
Family medicine residents were taught correct inhaler technique with an inhaler training device (In-CheckTM DIAL G16) using a didactic lecture with hands-on teaching exercise utilizing pharmacy interprofessional teaching. We assessed pre- and post-intervention comfort and knowledge of correct inhaler technique.
Results
Twenty of twenty-seven eligible family medicine residents attended an interdisciplinary workshop with clinical pharmacists with the purpose of improving inhaler technique comfort level and knowledge. A pre- and post-knowledge test and comfort questionnaire were provided to those participating. Comfort levels with prescribing different inhaler types increased after the intervention and knowledge of different inhalers improved.
Conclusion
Use of an inhaler training device coupled with an interdisciplinary lecture format improved provider knowledge of correct inhaler technique and comfort with prescribing inhalers.
Introduction
Correct inhaler technique is crucial in the management of respiratory diseases. Incorrect technique is common (70-80% of patients) and is associated with increased Emergency Department visits, hospitalizations, and poorer outcomes.1,2 Global Initiative for Asthma (GINA) and Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines note that patients should be instructed on correct inhaler technique when inhalers are prescribed and should be periodically checked.3,4 Despite this recommendation, this is often not performed with one study in a pediatric population indicating that only 10% of providers have patients demonstrate correct technique for pressurized metered-dose inhalers (pMDIs) on prescribing. 5 Moreover, many health care providers lack the knowledge and skill on how to model proper use with a meta-analysis finding only 15.5% of health care providers correctly exhibited inhaler techniques to patients. 6 Various methods have been shown to improve inhalation techniques in patients including face-to-face provider-patient training sessions, video based inhaler technique interventions, and interventions utilizing both clinical pharmacists and well-trained nurses.7-11 Furthermore, training sessions for primary care providers have been shown to improve their knowledge and ability to demonstrate correct inhaler techniques as well as improve patient outcomes.7,12
Prior studies of inhaler technique knowledge among medical trainees has demonstrated association between postgraduate year of training and knowledge of correct inhaler technique, however correct response rates were low across the postgraduate years. 13 Prior investigation has demonstrated that teaching interventions aimed at bolstering medical trainees knowledge of proper inhaler technique in internal medicine residents led to improvement in inhaler knowledge14,15 A prior study demonstrated similar findings in family medicine residents that utilized instruction manuals and devices for home study with a follow-up tutorial session and post-test knowledge assessment. 16
There are various inhalers on the market with pressurized metered-dose inhalers (pMDIs), dry powdered inhalers (DPIs), and soft mist inhalers (SMI) commonly prescribed. These device types differ in regard to patient’s pulmonary effort and inspiration for adequate medication delivery. Use of multiple inhaler types has been predictive of increased errors with use. This suggests that patients are likely not recognizing the need for different administration techniques between inhaler types. 17 Different training tools have been developed to address this. The In-CheckTM DIAL G16 is an adjustable inspiratory flow meter that is able to simulate resistant patterns of different inhaler types. It has been shown to improve patient inhaler technique by informing patient of correct effort needed for different types of inhalers. 18 However, there are limited studies investigating its use as an educational tool. The purpose of this study is to evaluate the change in baseline knowledge of inhaler technique and comfort level among family medicine trainees after a pharmacist-led workshop utilizing a didactic lecture and hands-on teaching session using the inhaler training device, In-CheckTM DIAL G16.
Methods
Family Medicine residents from a single site in postgraduate years (PGY) 1-3 were invited to attend a one hour in-person inhaler training workshop as part of their regular didactic education. Participants were informed that their participation was voluntary and verbal consent was obtained. Pre- and post-surveys were marked with a unique identifier so as to blind investigators from the identity of participants. Education strategies utilized during the workshop included a lecture, which reviewed the characteristics of various inhaler types, followed by demonstration of correct inhalation technique using placebo inhaler devices and the In-CheckTM DIAL G16 inhaler training tool. Participants were then invited to demonstrate correct inhalation technique using the placebo inhaler devices and the In-CheckTM DIAL G16 tool for pMDI, DPI, and SMI and were given verbal feedback from the instructing pharmacist. The In-CheckTM DIAL G16 inhaler training tool is an inspiratory flow meter that is calibrated to mimic the airflow resistance pattern of various types of inhaler devices including pMDI and DPI inhaler devices. 18
Pre- and Post- Workshop Questionnaire
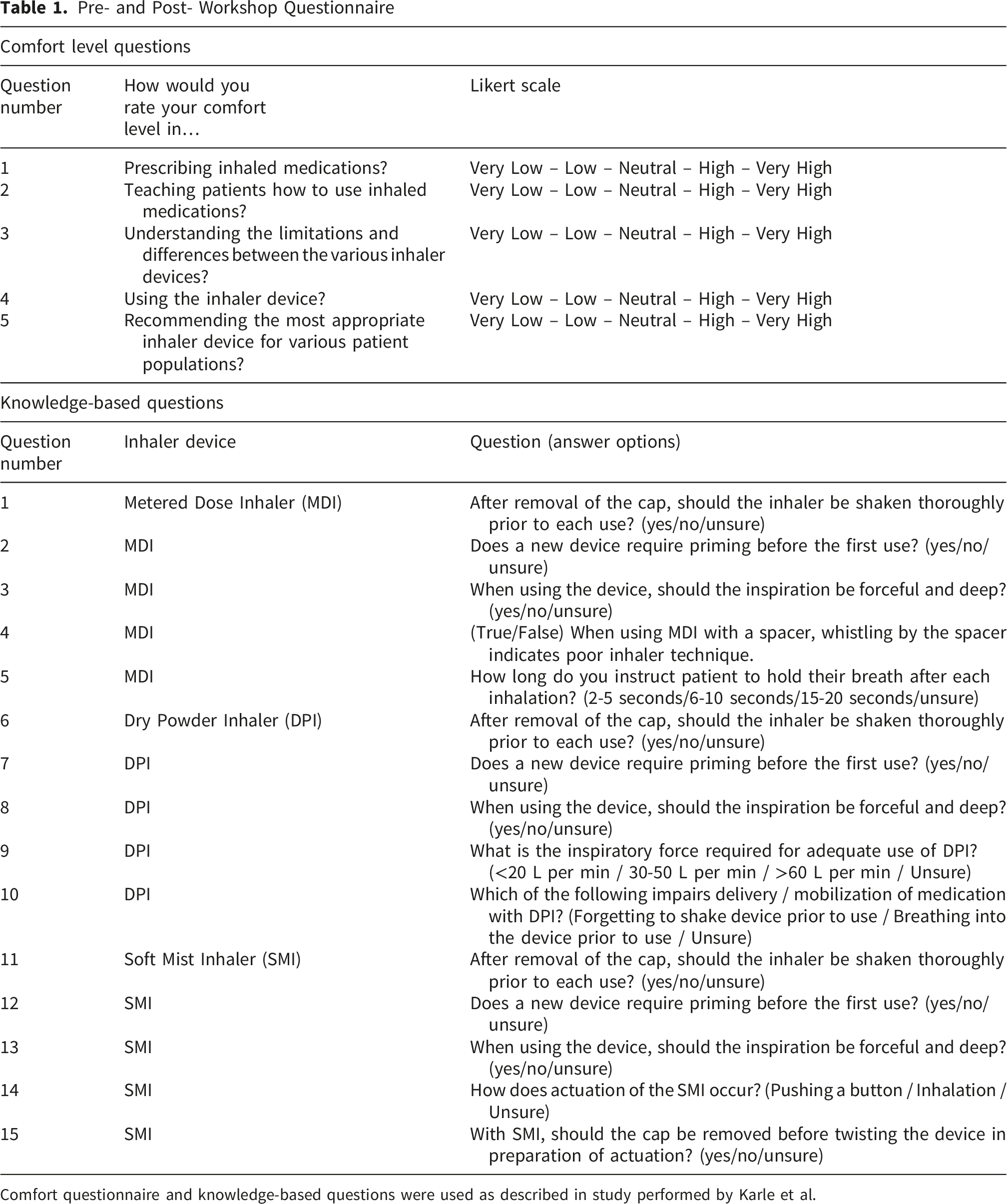
Comfort questionnaire and knowledge-based questions were used as described in study performed by Karle et al.
Statistical analysis was performed on non-parametric data using the Wilcoxon Paired Test to evaluate pre- and post-test comfort scores both cumulatively (PGY1-PGY3) and within each postgraduate year group. Wilcoxon Paired Test was also used to evaluate pre- and post-test change in knowledge-based assessment among individual PGY groups given small sample sizes. Kruskal-Wallis test was utilized to evaluate changes across PGY groups in both pre-intervention and post-intervention comfort scores. The sum of participants knowledge-based questions corresponding with each type of inhaler type (pMDI, DPI, SMI) was obtained and paired t-tests were performed for cumulative knowledge-based pre-tests and post-tests. Statistical analysis with one-way ANOVA was performed to compare pre- and post-test scores across training level. This research project was granted exemption status from our institutional review board.
Results
In the Fall 2022, twenty-seven residents were invited to the described inhaler workshop as part of their regular didactic teaching of which twenty residents attended (74%). Those absent were primarily due to other clinical responsibilities. A total of 17 individuals completed the pre- and post-intervention comfort questionnaires whereas all twenty completed the knowledge-based assessment. The reasoning why 3 individuals did not complete the survey is unknown but all 3 were in post graduate year one (PGY-1). A plurality of participants that completed the knowledge-based assessment (9/20) were PGY-1 of training, six were PGY-2, and 5 PGY-3.
Pre- and Post-Intervention Comfort Questionnaire
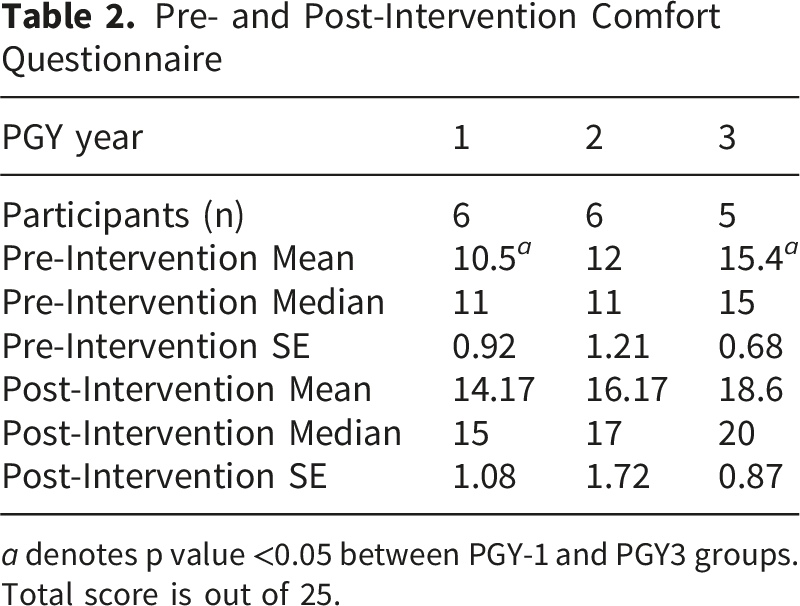
a denotes p value <0.05 between PGY-1 and PGY3 groups. Total score is out of 25.
Pre- and Post-Intervention Knowledge Based Assessment
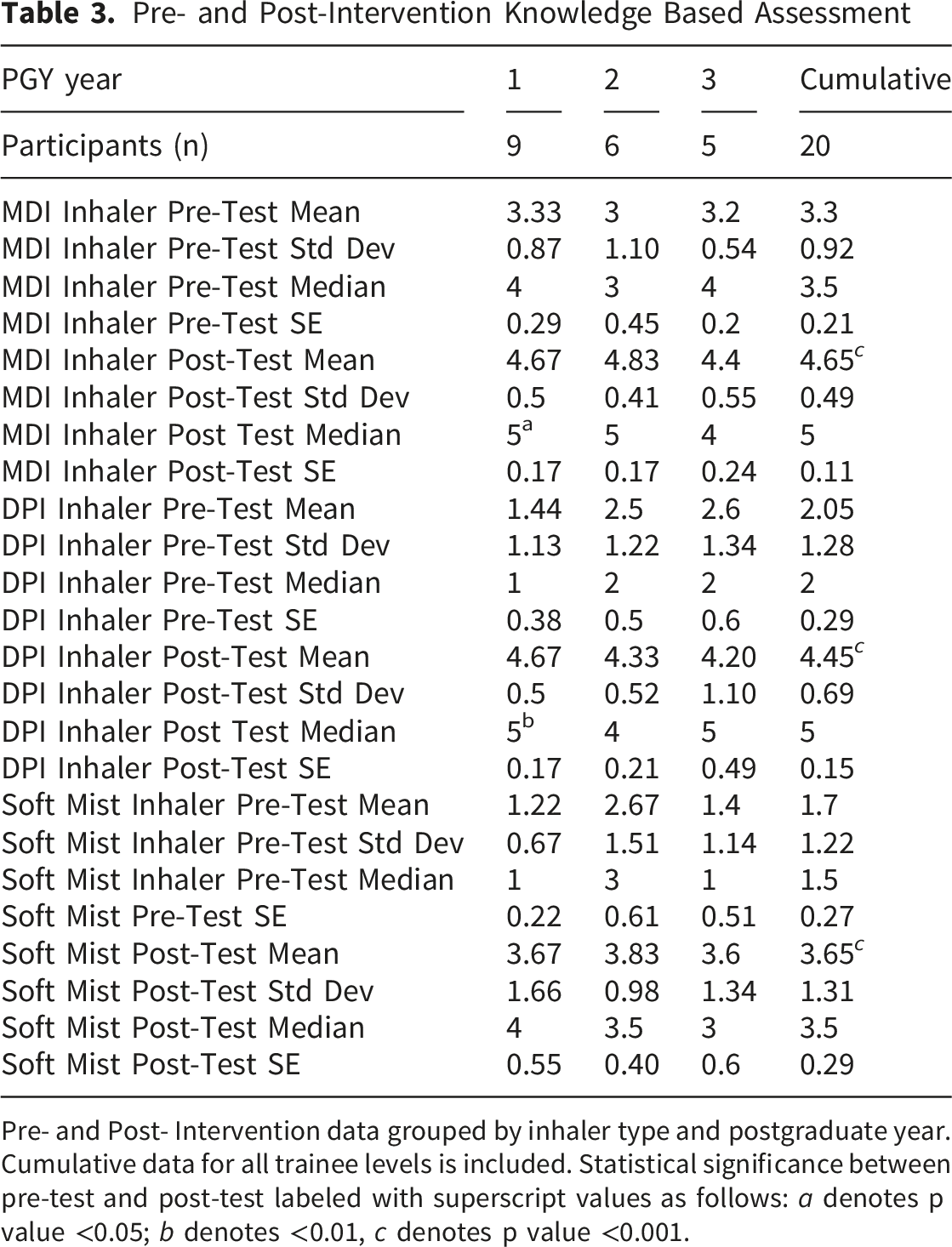
Pre- and Post- Intervention data grouped by inhaler type and postgraduate year. Cumulative data for all trainee levels is included. Statistical significance between pre-test and post-test labeled with superscript values as follows: a denotes p value <0.05; b denotes <0.01, c denotes p value <0.001.
As described above, the In-CheckTM DIAL G16 inhaler training tool is an inspiratory flow meter calibrated to mimic the airflow resistance pattern of various types of inhaler devices including pMDI and DPI. The efficacy of this device as a teaching tool was indirectly evaluated in the comfort level questionnaire (Questions 3 and 5) and in question number 3,5,8, and 13 of the knowledge-based assessment (Table 1). As noted above, comfort level was significantly increased across postgraduate levels after this intervention. The number of learners answering question 3 pertaining to force required for inspiration on pMDI inhalers correctly improved from 6 out of 20 on pre-test to 15 out of 20 on post-test. Most learners were aware of the need for deep inspiration while utilizing DPI (Question 8). Post-intervention, there was improvement in learners correctly identifying the inspiratory force required for DPI inhalers (Question 9) with only one learner identifying the correct response on pre-intervention assessment as compared to 18 out of 20 learners on post-intervention assessment.
Discussion
Management of chronic respiratory illness is an important aspect of primary care practice. Excellence in managing this chronic condition depends on selecting the most appropriate drug and a delivery system best suited for the ability and needs of the patient. While GOLD and GINA guidelines recommend instruction to patients on inhaler technique, many healthcare providers do not practice this and/or lack the skills to complete this important task.3-6 Therefore, education about inhaler delivery systems and technique as part of residency education is of vital importance.
In this pilot study, an interprofessional educational intervention utilizing didactic learning and a novel approach for hands-on learning of inhaler technique using the In-CheckTM DIAL G16 inhaler training tool was demonstrated. The data from this pilot study shows the potential efficacy of this approach with improvement in knowledge base across inhaler types and increased comfort in inhaler prescribing present across postgraduate year of training. These results are consistent with other prior studies that have demonstrated improvement in knowledge of correct inhaler technique.7-12,14,15 Our results suggest that an inhaler training tool could provide learners with increased comfort and knowledge with various inhaler delivery systems.
While the described pilot study demonstrated improvement with this learning intervention, further studies with greater sample sizes and more longitudinal follow-up are clearly warranted. Learning cohorts were admittedly small and homogenous. Including larger sample sizes as well as learners from different institutions could further assess the validity of this intervention. Results from statistical analysis must also be tempered by the small sample sizes (especially with subgroup analysis) and lack of multiple comparison correction. The results of the comfort survey data could also be impacted by the absence of 3 individuals (all in PGY-1 class) that did not complete this survey. While knowledge of correct inhaler technique was tested, individuals were not assessed on their ability to demonstrate correct inhaler technique and inspiratory flow measurements were not objectively captured. The importance of the inclusion of this skill-based assessment cannot be understated as providers may ultimately have to demonstrate technique to patients. In addition, long-term retention of material was not captured in this study and is important for assessing the durability of the learning intervention. Future investigations into the retention of this information, and ability to demonstrate correct technique as individuals progress through their postgraduate years, could be future direction of investigation into this question.
Finally, the impact of this learning on provider inhaler prescribing or patient outcomes was not assessed. However, the impact of improving patient education on correct inhaler technique has been shown in several studies with positive outcomes including improved medication adherence and reduced acute care events 30 days after discharge from the hospital for asthma or COPD.19,20 It would be reasonable to hypothesize that improved health care provider knowledge and comfort level with correct inhaler techniques could translate into better patient education and ultimately to better patient outcomes. This could certainly be an area of worthwhile future study.
Conclusion
An interprofessional workshop with clinical pharmacists and family medicine residents that utilized hands-on teaching devices including placebo inhalers and the novel inhaler training device (In-CheckTM DIAL G16) was effective in improving the knowledge of inhaler technique and comfort level in prescribing inhalers among family medicine residents across postgraduate year. Given the importance of proper inhaler technique, further studies are warranted. Proposed areas of further studies include investigation into durability of inhaler knowledge, demonstration of correct inhaler technique across inhaler types, and whether this improved knowledge base leads to better patient education and outcomes.
Footnotes
Ethical Considerations
Ethics approval was not required for the study described in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.