
Abstract
Background
There is extensive literature on the benefits of Continuity of Care (CoC) with the same General Practitioner (GP), including improved healthcare outcomes, increased satisfaction, and reduced costs. Models such as microteams are being explored to sustain continuity amid rising demand and workforce challenges. However, there is limited evidence describing their implementation or the monitoring of continuity during organisational change.
Aim
To describe a real-world approach to implementing microteams and monitoring CoC, and to explore the association between microteam implementation and CoC within a large Primary Care Network (PCN).
Design and Setting
Observational before-and-after study conducted in a large multi-site PCN serving 46,500 patients across eight sites between March 2022 and March 2024.
Method
CoC was measured using the Usual Provider of Care (UPC) index, representing the proportion of consultations with the same GP or GPs within a microteam. UPC scores before implementation (March 2022–March 2023) were compared with scores after implementation (March 2023–March 2024) using t-tests.
Results
Twelve microteams were implemented across the PCN. Among patients with ≥3 GP appointments, the UPC score increased from 0.034 to 0.358 (p<0.001). Across all patients with GP appointments, the UPC score increased from 0.033 to 0.375 (p<0.001). Excluding urgent care appointments produced similar results (UPC 0.355). Patient satisfaction also improved following implementation, although findings should be interpreted in the context of concurrent organisational changes, including a practice merger.
Conclusion
Microteams can be implemented within a large multi-site PCN, and continuity of care can be monitored using routinely collected data. Implementation was associated with substantially higher UPC scores, suggesting improved team-based continuity. Although causality cannot be inferred from this uncontrolled service evaluation, the model may provide a pragmatic approach to supporting continuity in large multidisciplinary primary care organisations.
How This Fits in
The focus for CoC has been with the individual GP. Less is known about the settings of larger networks with multi site organisations, the design, implementation and effect of using microteams whilst monitoring CoC. This observational pre and post study describes the introduction of microteams with the intention to improve CoC within a large network of general practices covering 46,500 patients. A model for microteams is described along with an approach to the implementation and monitoring of CoC. Results indicate an association with improved continuity, alongside better patient and staff satisfaction following the service change. This model is transferable and may help others in primary care who are considering the introduction of microteams.
Introduction
Continuity of Care (CoC) is defined for this study as the ongoing, co-ordinated management of a patient’s health by a physician or physician-led team, fostering a long-term partnership that enhances patient trust, safety, and cost-effective care through comprehensive support. 1 Continuity can be categorised into relational, managerial, and informational, each addressing different aspects of patient care. 2 The most researched type, relational continuity, looks at the impact of CoC with the same General Practitioner (GP). Research indicates that this CoC type is associated with increased patient satisfaction,3-5 better adherence to treatment plans,6,7 and stronger doctor-patient relationships.8,9 Relational continuity of care with one GP positively impacts the quality of care provided,10,11 reduces the likelihood of emergency department visits,12,13 and decreases hospital admissions. 14 Financially, CoC proves to be cost-effective.15,16 CoC benefits healthcare providers, with GPs reporting higher job satisfaction 17 and perceiving continuity as a safer practice. 18 It has also been linked with a decrease in burnout. 19 Patients demonstrate increased confidence in their caregivers when there is a continuous relationship, 20 factors which together have been linked to lower mortality rates.21-23 Various methods exist to measure CoC, with the most common being the Usual Provider of Care (UPC) index, 24 which measures the proportion of times a patient sees the same person during a specified period.
Despite the consistent evidence on the benefits of CoC, there has been a notable decline in its delivery within the UK. 25 This reduction in continuity appears to align with recent policy shifts that have prioritised GP accessibility. 26 Further contributing factors include an increasing trend of GPs retiring early or reducing their working hours 27 and a limited focus on CoC in medical school education. 28 Some practitioners perceive that CoC is feasible only within small GP practices with GPs working near to full time. However, high levels of continuity can be achieved in larger practices and with job plans that support less than full time working. 29
The formation of microteams, to improve continuity 30 and patient-related outcomes 31 in primary care, is one method of achieving CoC in larger organisations. It is likely that improved co-ordination with a named GP overseeing the patient’s care and communication within a team will provide at least some of the benefits of CoC. There is no strict definition of what constitutes a microteam, with teams free to define their own model which could include any variety and number of professionals, 32 leading to more sustainable healthcare. 33
In this observational study, we describe the introduction of microteams and explore the effect of this model on CoC in a large, multi-site practice. The study setting was a large Primary Care Network (PCN) which operates as a single partnership across eight sites. It is based in Southampton, serving a population of 46,500 patients, in an area with marked health inequalities (Figure 1). Index of deprivation across Southampton and the PCN site location (Source: https://data.cdrc.ac.uk/dataset/index-multiple-deprivation-imd)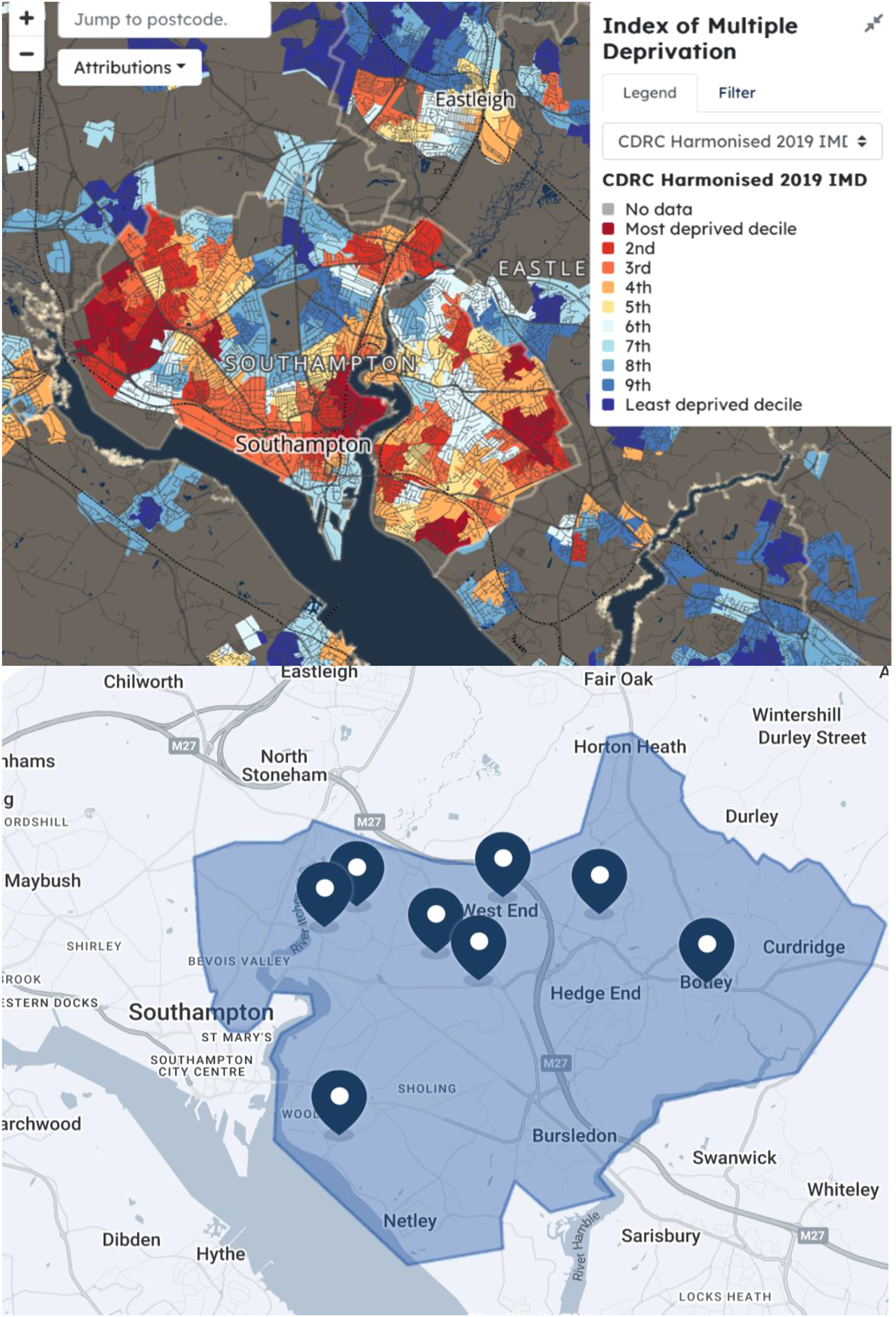
Methods
This was a service evaluation of routinely collected, anonymised data undertaken within local governance arrangements. CoC became a priority due to fragmented care for complex patients, as there was random allocation of appointments to GPs, including locums, resulting in a more transactional and faceless primary care. Many named GPs during pre-implementation were heavily involved with triaging patients and not directly seeing patients face to face. There was cross-site working and no base for the GPs. Named GPs held a formal designation on patient records but this did not translate into preferential booking. This system, while designed to enhance access, structurally precluded the development of relational continuity. There were increasing patient complaints and frustration expressed by staff about the inability to deliver exemplar heathcare. Improving continuity was anticipated to enhance patient satisfaction, trust, and staff retention while enabling better oversight of disease pathways. However, limited GP availability and an increasing patient to GP ratio made one-to-one CoC difficult to achieve. These factors were catalysts for the formation of a microteams model. Weekly multidisciplinary meetings took place over six months, with representation from all sectors of the organisation, to ensure that proposed changes were thoroughly discussed for their impact, potential issues, and concerns before implementation. Key planning steps included detailed action trackers with Red, Amber and Green (RAG) ratings to monitor progress and support the transition. Staff engagement was prioritised through consultations, role transition interviews, and in-house training events. On March 6, 2023, the practice inaugurated microteams to improve CoC.
Patient and Public Involvement
Patients and the public were involved in the design and implementation of the microteams model. Engagement included the PCN’s Patient Participation Group (PPG), patient advocates, social prescribing groups, and patient-facing communications (including practice blogs) to support understanding and acceptability of the change.
Whilst patients participated in the service change described above, this study represents a secondary analysis of routinely collected data.
Implementation
Twelve teams were formed, with a named GP allocated to the patient cohort for that team. The named GP was an experienced GP allocated to provide leadership and hold overall responsibility for patients under the team. Each team had access to around ten GP sessions per week provided by between two or three salaried GPs. This provided over a hundred face-to-face appointments per week, with each GP typically seeing four patients with twenty-minute appointments and six patients with fifteen-minute appointments. Telephone consultations with a GP were set at ten-minutes each, with five minutes for administrative or text-based consultations. Defining the British Medical Association (BMA) contract of appointments in this way allowed flexibility in meeting patient needs while maintaining an efficient workflow.
The patient population was risk-stratified to ensure equitable distribution across the twelve teams, with each team having a balanced mix of high and low-intensity users, as well as residents of care homes. Geographical considerations across the eight sites were also factored in. Each team was responsible for delivering care to around 3875 patients. Depending on space and volume of patients, some sites had either two or three teams. There was cross-cover within the team site (but not across sites) during leave. Care Coordinators (CC) were assigned to each team to facilitate reviews of specific patient groups, such as those undergoing cancer care. The CC role was further supported by CC assistants to help with administrative duties such as referrals and appointment booking. Each site also housed allied healthcare staff including but not limited to phlebotomy, healthcare assistants (HCAs), practice nurses, pharmacy teams, and an urgent care team member. Figure 2 provides an overview of the PCN structure encompassing the microteams model. Structure of the PCN – orange circles represent microteams whereas blue circles each represent one site where clinical work takes place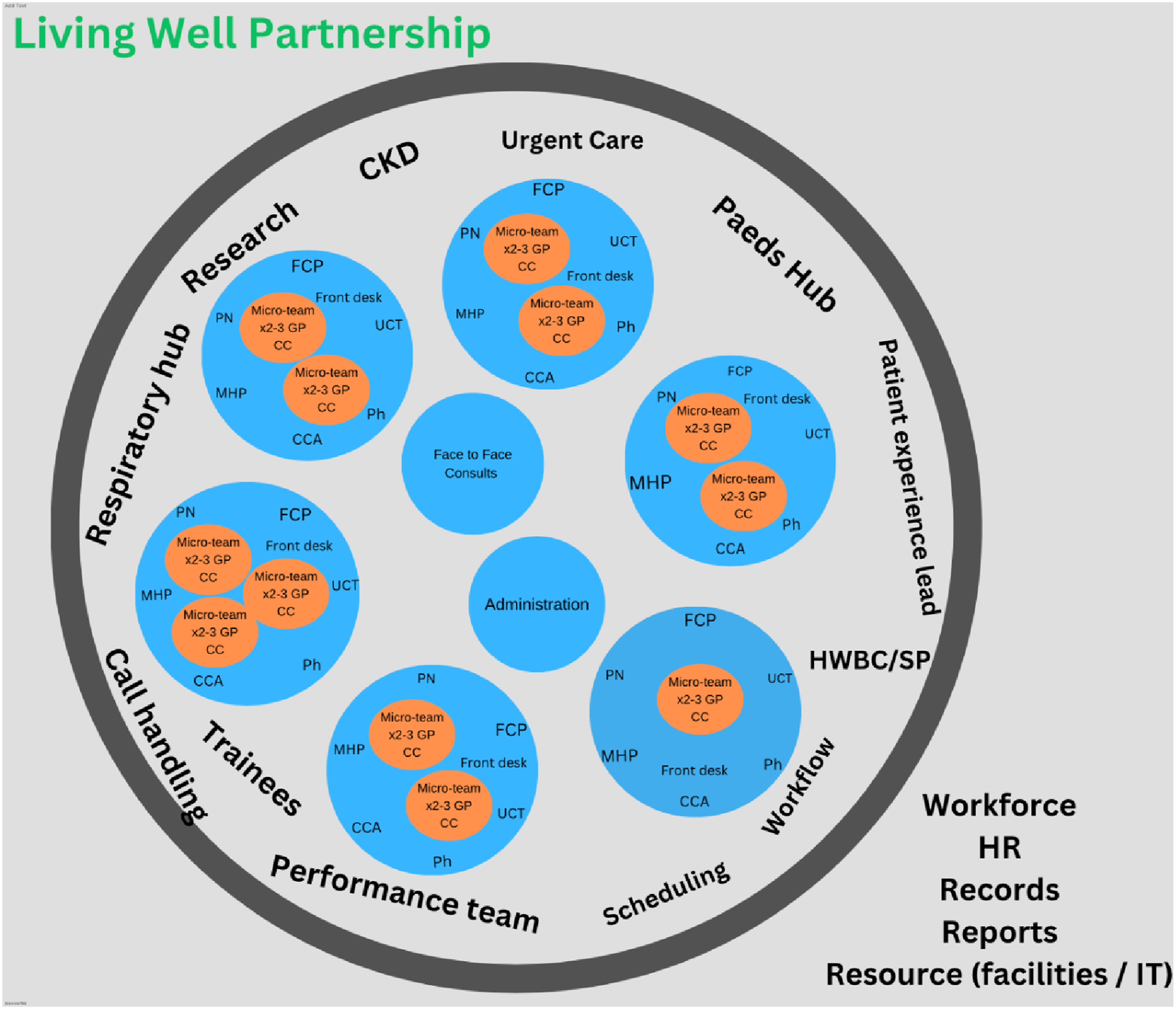
We utilised appointment audit data for the PCN, extracted from the EMIS electronic medical records system, covering two time periods: 6 March 2022 to 5 March 2023, and 6 March 2023 to 5 March 2024. The data sets were analysed for two groups: patients who had at least three appointments over one year, defined as more frequent users within each period, and all patients, regardless of the number of appointments. All patients registered with the practice who met the inclusion criteria, within each defined time period, were included in the analysis. Patients were not individually matched across these two periods, and each time period represented a separate cross-sectional cohort reflective of the practice population at that time. No computation was performed for missing data; with analysis conducted on available complete cases from routine datasets.
Datasets were organised into Microsoft Excel spreadsheets (see supplementary box S1) for both periods: one for each named GP in the pre-microteams period (six spreadsheets) and one for each named GP team lead in the post-microteams period (twelve spreadsheets). Each spreadsheet contained patient identifiers (EMIS numbers), the number of appointments with the named GP or named team of between two or three GPs and the total number of appointments with other GPs. Non-GP appointments were excluded from the analysis. The comparison was therefore between one named GP before the intervention of microteams and two or three GPs working together with a named GP team lead during the intervention period. In the pre-implementation period, urgent care was handled by the regular appointment team, there was no distinct separation between routine and urgent care encounters. On implementation of microteams, the acute care was separated from routine care allowing the UPC for acute care and for routine care to be compared. For the period after the microteams were implemented, the UPC was recalculated with the exclusion of acute and urgent care appointments.
The UPC index used to measure continuity was defined as the ratio of appointments with the named GP or named GP team compared to the total sum of GP appointments used by that patient. The UPC index was chosen as the most pragmatic approach because it is easier to calculate in a large practice with multiple GPs and is commonly applied as a measure of continuity. UPC index values are reported as proportions ranging from 0 to 1 throughout this manuscript, consistent with standard reporting conventions. The UPC index was calculated twice (see supplementary box S2): once for patients with at least three appointments over the one year period and again for all patients attending at least once in the one year period.
Descriptive statistics, including means and standard deviations, were calculated for both periods. An independent sample t-test was conducted to compare the UPC indices before and after the implementation of microteams. The t-test was selected as a pragmatic approach to comparing groups that could be applied by GPs and managers with basic statistical knowledge in this setting. Given that UPC is a bounded proportion and the analysis was not adjusted for confounders, the t-test is only an indicator of the difference occurring by chance and does not indicate cause. Results are reported with 95% confidence intervals where appropriate. All analyses were conducted using IBM SPSS version 29.0.
Results
Over the period from 6 March 2022 to 5 March 2023, a total of 1,024 patients had three or more appointments with a GP. The UPC score for this period was 0.034 (SD = 0.121), indicating a low level of CoC. This low finding was consistent with the transactional care that was observed as being provided by the PCN.
Following the implementation of microteams, from 6 March 2023 to 5 March 2024, a total of 4,070 patients had three or more appointments with a GP. The UPC score for this period improved to 0.358 (SD = 0.355), reflecting an increase in CoC. An independent t-test indicated that this improvement was statistically significant (p < 0.001; 95% CI 0.311 to 0.337).
Further analysis was carried out to include all patients with GP appointments, regardless of the total number they attended, using the same time intervals as in the initial analysis. In the pre-intervention period (6 March 2022 to 5 March 2023), a total of 4,804 patients were included, compared to 15,436 patients in the post-intervention period (6 March 2023 to 5 March 2024). This difference in total patient numbers is addressed in the discussion section and related to a practice merger. The UPC score for all these patients in the pre-intervention period was 0.033 (SD = 0.159), while the post-intervention score increased to 0.375 (SD = 0.437). This improvement was statistically significant (p < 0.001; 95% CI 0.330 to 0.355).
Comparison of Patient Cohorts and UPC Scores Across Pre-intervention (6 March 2022 to 5 March 2023) and Post-intervention (6 March 2023 to 5 March 2024) Periods
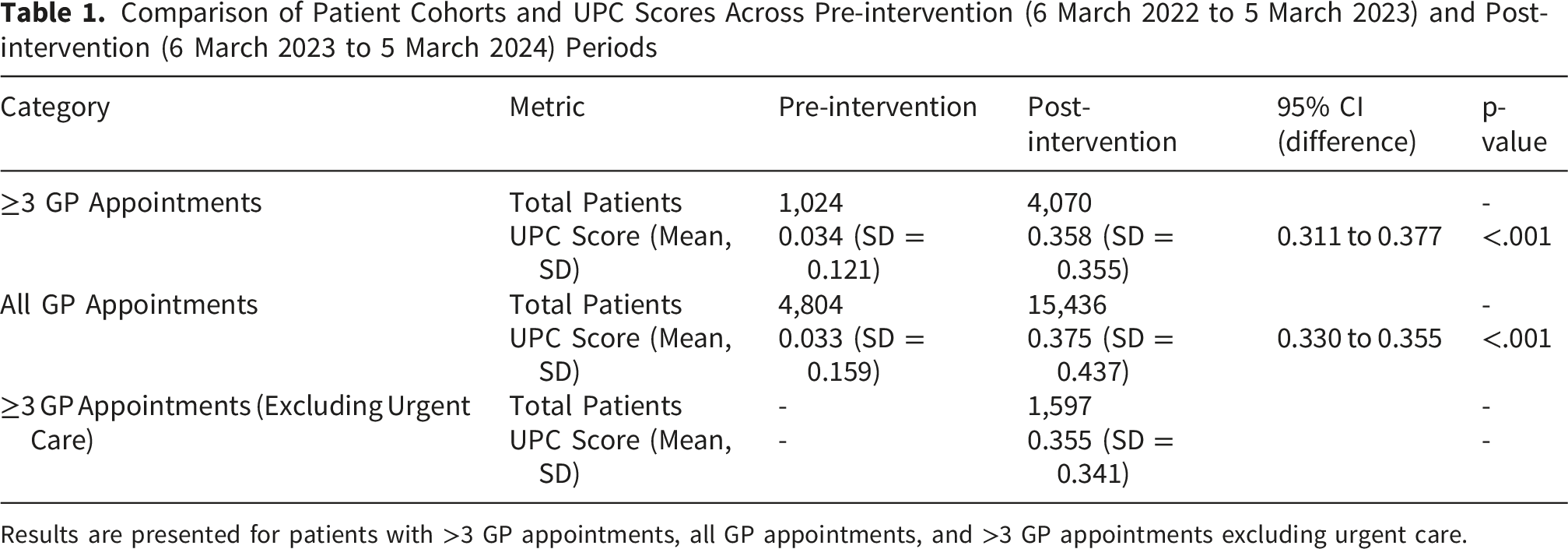
Results are presented for patients with >3 GP appointments, all GP appointments, and >3 GP appointments excluding urgent care.
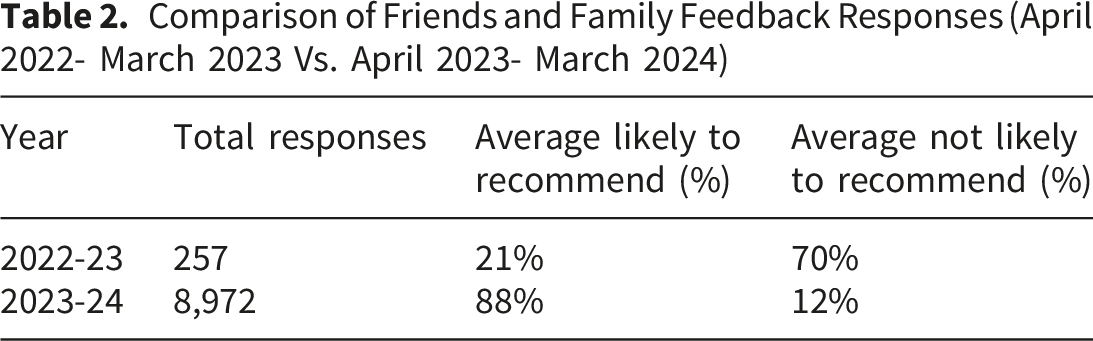
Comparison of Friends and Family Feedback Responses (April 2022- March 2023 Vs. April 2023- March 2024)
Discussion
This observational before and after study examined the introduction of microteams in a large multicentre PCN and indicated an association with improved CoC. This was a pragmatic approach to monitoring change in a real-world setting of merging General Practices where other confounding factors could have contributed to the observed increase in CoC.
There are few examples, and little advice, on how to introduce microteams and monitor continuity in primary care where there is limited time, no readily accessible IT packages, no facilitation and limited local expertise. The other challenge, illustrated in this study, is how to measure continuity when the definition is changing as the patient moves from a relationship with one doctor to a relationship with several doctors within a team of people.
Existing evidence demonstrates the benefits of continuity with the same GP. Microteams represent an alternative model that seeks to maintain continuity through ongoing relationships with a small, consistent team of clinicians rather than a single doctor. While this approach may support relational and organisational continuity, its impact on patient outcomes remains unclear.
Our findings report a significant improvement in the UPC index, from 0.034 to 0.358, following implementation, suggesting that microteams may help sustain continuity in the face of the increasing patient to GP ratios seen across the UK. 35 It is noteworthy that even following implementation, approximately one-third of consultations were conducted with a GP from the patient’s named team, which reflects the complexity of achieving relational continuity in a large multi site organisation. Also, the unusually low pre-intervention UPC score can be described as a consequence of the system design. Continuity occurring with non-named GPs was not captured, meaning the true baseline of relational continuity across the practice may have been somewhat higher.
Continuity was measured in relation to just the patient’s named GP during the pre-implementation period and to all the GPs within the allocated microteam in the post-implementation period. This was a consequence of the microteam model, which also provides continuity through shared team responsibility and communication. This reflects the real world implementation of team-based continuity but may influence numerical comparisons of the UPC measures pre- and post-intervention and is discussed in the limitations below.
In addition to relational continuity, microteams were intended to enhance backstage and organisational continuity through structured handovers and coordinated care. Patient satisfaction, as measured by the Friends and Family (F&F) improved post-intervention, with 88% of approximately 800 monthly respondents recommending the practice, compared to just 21% of 257 respondents in the previous year. This may suggest a positive impact of microteams on patient experience.
GPs reported greater job satisfaction due to reduced administrative burdens and a stronger clinical focus, as evidenced by verbal feedback. Care co-ordinators played a key role in supporting their microteams by managing non-clinical aspects of patient care, particularly for those with complex non-clinical needs. Their involvement in signposting, coordinating care, and addressing social concerns was another factor that may have contributed to reducing GP workload and increased GP satisfaction.
The total number of patients with GP appointments increased significantly post-intervention due to the practice merger, rising from 4,804 to 15,436. The cohorts were constructed separately for each 12-month period using all patients with GP appointments in that period, or just those with three or more appointments. Despite this increase, the proportional distribution between all patients and frequent users with three or more appointments remained similar. The increase in routine GP appointments from 44,459 to 61,353, a 38% rise, may reflect increased demand or improved accessibility through digital and phone consultations. While these findings may be associated with the introduction of microteams, external factors such as post-COVID-19 changes and the practice merger will have influenced appointment patterns and continuity metrics. The reality of GP practices is that they are dynamic environments, where multiple changes can occur simultaneously, each potentially influencing continuity to a degree.
Several limitations of this study should be acknowledged. First, the pre- and post-intervention UPC measures are not directly comparable in a strict methodological sense: pre-intervention UPC reflected consultations with a single designated GP, whilst post-intervention UPC reflected consultations within a designated team of two or three actively practising GPs. The magnitude of the observed improvement should therefore be interpreted as reflecting a shift from a transactional to a team-based model, rather than a precise quantitative measure of change in relational continuity. It should also be acknowledged that continuity occurring with non-named GPs in the pre-intervention period was not captured, meaning the true baseline level of relational continuity may have been somewhat higher than reported. Second, the two study periods represent different underlying patient populations due to the practice merger; patients were not individually matched across periods and the merger itself may have independently influenced appointment patterns. Third, given that UPC is a bounded proportion, the independent samples t-test does not fully satisfy assumptions of normality, and findings should be interpreted with appropriate caution despite the large sample sizes. Fourth, Friends and Family test data should be treated cautiously given unknown response rates, differing respondent numbers, and the possibility of response bias following organisational change. Finally, this study was conducted within a single large urban PCN serving a population with marked health inequalities, and findings may not generalise to smaller, rural, or differently configured practices.
Further research is required to determine whether microteams can match the outcomes of traditional GP continuity, as much of the existing literature focuses on continuity with an individual GP; whereas this study looked at continuity within a team-based model. Direct comparisons between the two are highly limited. Additionally, organisational and informational continuity remain underexplored areas in the literature, despite their potential to improve patient care.
Past initiatives, such as the Valentine Health approach under the Health Foundation CoC program, 36 highlight the need for sustained interventions to maintain continuity gains. Regular team reviews, staff reminders, and patient engagement strategies are essential to prevent regression. While the UPC index at the PCN showed improvement post-intervention, it remains below the expected baseline for microteams continuity seen in other settings.24,37 The unusually low pre-intervention UPC scores (potentially influenced by the merger of practices) are relevant. Practices with higher baseline continuity may respond differently to the microteams model. The starting level of continuity could play a significant role in determining the intervention’s impact. Investigating these dynamics could provide insights for appropriately tailoring the model to diverse practice settings. It is important to recognise that there is no universally defined ‘ideal’ UPC score, and achieving 100% continuity is neither realistic nor necessarily desirable as not all encounters require GP CoC. The average level of GP face-to-face continuity appears to be around 50%, though this is influenced by factors such as practice size and patient demographics. 37
Continuity metrics should be interpreted as part of a broader picture, rather than fixating on numerical targets. The focus should remain on leveraging continuity improvements to enhance the overall patient and provider experience, whilst using the UPC as one of many evaluative tools to support this.
Conclusion
As the primary care landscape evolves, microteams may be a practical and scalable alternative to traditional continuity models, offering a balance of flexibility and patient-centred care. In this service evaluation, the introduction of a microteam model was associated with an increase in the UPC score used to monitor CoC as well as improved feedback from patients and staff. Microteams have other benefits, including the integration of allied health professionals, such as care coordinators, to further support the care model. Further research is needed on the impact and benefits of microteams compared to single GP CoC.
The importance of measuring continuity cannot be overstated. Establishing a routine, standardised assessment of continuity enables practices to monitor and improve their delivery of care. The RCGP Continuity of care Toolkit 38 offers a practical approach for practices to start to evaluate their continuity metrics. Our study proposes a simplified approach to measuring continuity within microteams, which could be adapted and further developed by other practices. National tools linked to the commonly used clinical records systems are required to give simple clear feedback on continuity on a regular basis. We believe that consistently implementing measurements of CoC will be key to improvements in healthcare across both primary and secondary care.
Ethics
This study was conducted as a service evaluation using anonymised routinely collected data so formal ethical approval was not required. All data were handled in accordance with relevant data protection standards.
Supplemental Material
Supplemental Material - Is Adopting a Microteams Model a Solution to Delivering Continuity of Care in Modern Primary Care?
Supplemental Material for Is Adopting a Microteams Model a Solution to Delivering Continuity of Care in Modern Primary Care? by Ioannis Saxionis, Mark Rickenbach, Martine Cross, Harnish P. Patel, Sam White, and Pritti Aggarwal in Journal of Primary Care & Community Health.
Footnotes
Acknowledgements
We are grateful to the staff and patients at the LWP for their involvement in the microteams project, and to the partners of LWP for their support.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: No funding was granted for this study. IS was supported by NIHR as a research fellow for 15 months as part of a pilot in his GP training at the LWP. HPP is supported by the NIHR Southampton Biomedical Research Centre, Nutrition, and the University of Southampton. This report is independent research and the views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. These funding bodies had no role in writing of the manuscript or decision to submit for publication. For the purpose of Open Access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising from this submission.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HPP has received lecture fees from Abbott, Pfizer, and HC-UK conferences outside of the submitted work. All other authors declare that they have no competing interests.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.