
Abstract
Objectives
As the number of individuals with obesity continues to grow in the United States, perspectives from patients on factors that help or hinder a patient’s weight management journey can guide clinical interventions and programs focused on obesity management. This qualitative research study using a social ecological model lens aimed to identify important patient attitudes, beliefs, and mental models relevant to obesity management in primary care among primarily Latino participants.
Methods
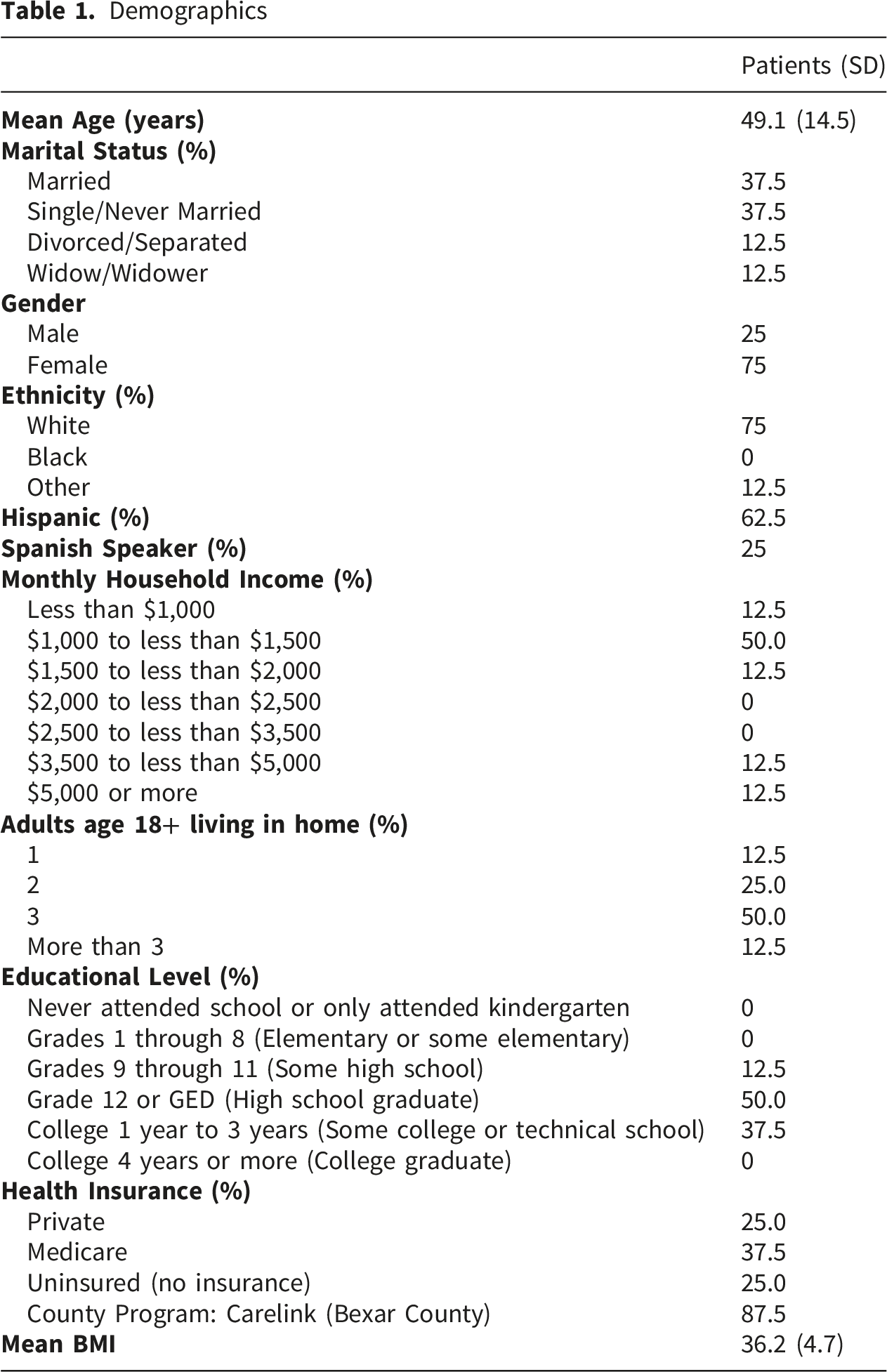
Participants were recruited from a local Family Health Clinic, located in a low-income neighborhood in San Antonio. Patients were selected from a group of patients who had previously implemented lifestyle changes without achieving significant reductions in BMI. Of the patients identified 8 participants completed interviews. Within this cohort, the majority (62.5%) of participants were females, identified as Hispanic (62.5%), making less than $1500 per month (75%), and had a high school education or less (62.5%). Most respondents reported participating in a county health safety net program (87.5%) and had a mean BMI of 36.1 mg/m2. Inclusion criteria was limited to those above 18 years of age, mentally competent to sign consent, English or Spanish speakers, with an established primary care physician, BMI 30 or above with comorbidities or 35 or above without comorbidities, have health insurance or participate in county funded payment plan.
Results
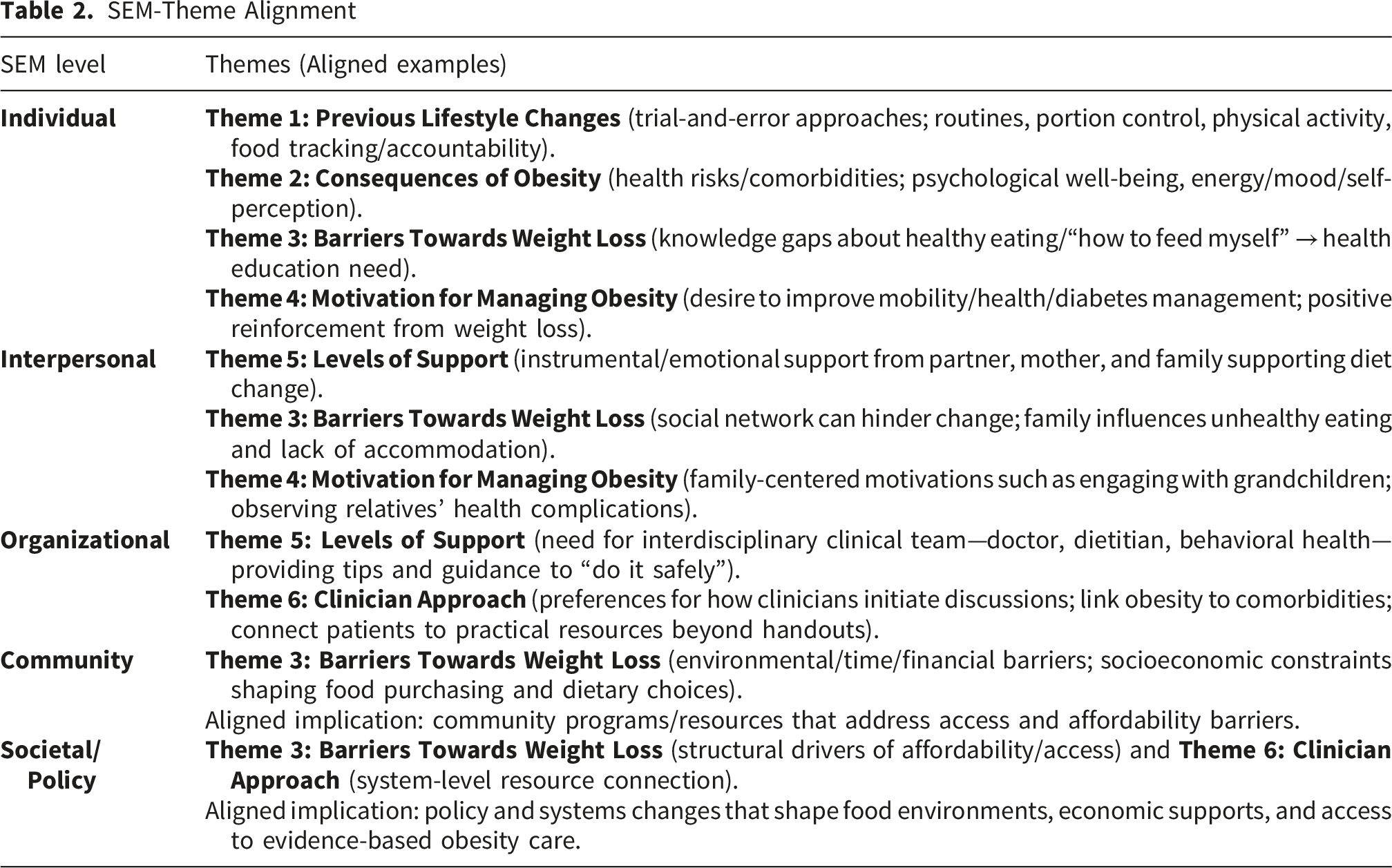
A thematic analysis informed by the SEM was used to analyze the qualitative data. From this, six themes emerged: Barriers Towards Weight Loss, Consequences of Obesity, Previous Lifestyle Changes, Effective Strategies, Motivation for Managing Obesity, and Levels of Support.
Conclusion
The findings highlight that obesity management is shaped by interconnected socioeconomic, cultural, and interpersonal factors. Participants identified several key motivators for change; of which, social support, particularly within family and community networks, emerged as an important facilitator of successful weight management. Additionally, patient-centered communication with health care clinicians, preferring approaches that assess readiness, address obesity-related health risks collaboratively, and provide practical, ongoing support rather than information alone. These findings underscore the need for culturally responsive, multidisciplinary, and resource-oriented interventions.
Introduction
According to World Health Organization, in 2016 more than 1.9 billion (39%) adults, 18 years or above were overweight (72.1%). 1 Additionally, 13% or 650 million (32.6%) were obese. Minoritized groups, particularly Latinos/Hispanics, have an increased prevalence of obesity. For example, severe obesity is prevalent nationally; however, 1 in 13 Hispanic adults have severe obesity in comparison to 1 in 11 non-Hispanic white adults. 2 Increased rates of obesity in Latino populations are due to genetics, lower diet quality, and other socioeconomic factors. In areas such as Bexar County, Texas, where more than half (60.7%) of the population is Hispanic, these patterns are exemplified as almost 71.9% of the population was considered overweight or obese in between 2025-2022.3-6
There is a close association between obesity and cardiometabolic risk factors due to insulin resistance resulting in prediabetes, diabetes, cardiovascular disease, some cancers, etc. 1 There is a sharp increase in diabetes prevalence rates in U.S. and worldwide resulting in significant patient morbidity and mortality and social cost. 1 Medical costs of obesity include direct (i.e.,$190.2 billion) and indirect costs (i.e.,$3.38-$6.38 billion). Studies have shown that only 10% reduction in current weight can significantly decrease morbidity and mortality related to obesity-related illnesses.7,8 The American Medical Association declared obesity a chronic disease in 2013, after voting from house delegates. 7 In 2016, an American Association of Clinical Endocrinologist (AACE) position statement concluded that’s “obesity clearly met criteria for a disease because it is heavily influenced by genetic factors, has identifiable signs and symptoms, involves pathophysiologic processes in tissues (e.g., adipose, hypothalamus), and causes morbidity and mortality. 7
There is vast literature on the influence of positive health behaviors in reducing obesity rates among populations. 9 Increased physical activity, increased fruits and vegetables, and decreasing saturated foods are well established approaches toward obesity and disease management.10,11 However, common barriers include time management, environmental factors including family and cultural influences, cost, and comorbidity diseases that impact health behaviors. 12
The Socio-Ecological Model (SEM) offers a framework for understanding how individual, interpersonal, community and organizational, and policy or societal factors—can either facilitate or hinder health behaviors and ultimately affect health outcomes. 13 According to the SEM, patients require support from each of these levels ranging from family and friends to national policy to facilitate positive healthy lifestyle choices. Despite this understanding, limited qualitative studies have explored experiences of adult obese patients, particularly environmental barriers, facilitators, and need for supportive medical practice, especially among a majority Latino population. The current study explores obesity-related perspectives among a broader adult Latino primary care population and examines multilevel barriers and facilitators influencing obesity management through the lens of the SEM.
Garcia et al. conducted a study with Hispanic men recruited from community organization, local gathering places and health care clinics in Arizona and found insights in general health beliefs, barriers, motivator for change, recruitment strategies amongst this group.
14
Agne et al. explored perceptions of obesity and weight loss among Latina immigrants recruited from a community hospital in Alabama.
15
However, there remains a paucity in the literature of perspectives of obesity and management within general primary care Latino patients. Additionally, prior literature including Khani et al. has emphasized the importance of patient-centered approaches and interventions in improving obesity outcomes, yet many current interventions are developed without substantial patient input, creating a gap between clinical recommendations and real-world implementation challenges.
16
Direct patient feedback on factors that help or hinder weight management can guide future clinical interventions and obesity management programs
Methods
Study Participants
Participants were recruited from the Family Health Clinic, a primary care clinic located in zip code 78207, a low-income neighborhood with majority Latino population, in San Antonio, Texas. This study employed purposive sampling as patients were selected to represent diverse experiences with weight loss. The sample included participants with diverse weight-management experiences: individuals who had previously implemented lifestyle changes without achieving significant reductions in BMI; those who had initially succeeded in losing weight but subsequently experienced weight regain; individuals actively engaged in behavior change with some success; and those who achieved sustained weight loss and maintained it over multiple years. Participants interested in making lifestyle changes but were not actively making changes. Eligibility criteria included patients to be 18 years or above, capable to sign consent, speak English or Spanish, have an established primary care physician, BMI 30 or above with comorbidities or 35 or above without comorbidities, have health insurance or participate in a county funded payment plan.
Procedures
Over an approximately three-month period, the principal investigator (PI), family medicine physician, identified potentially eligible patients through routine monitoring of patient panels. Additionally, during monthly clinic meetings attended by all physicians and staff, the PI delivered brief presentations requesting that physicians assist in identifying patients who met the eligibility criteria. Once potentially eligible patients were identified during a clinical visit, the physician, including the PI, approached the patient to assess their willingness to participate in an interview. Contact information for interested patients was then provided to the Research Coordinator, who followed up either by telephone or in person if the coordinator was present in the clinic. The Research Coordinator subsequently confirmed eligibility and scheduled the interview for a later date or conducted it immediately if both parties were available after the patient’s visit.
Upon enrollment, participants signed a consent form, participated in a brief demographic survey and a 45 minute to 1.5-hour interview, and received a $50 monetary compensation. Data was collected through in-depth semi-structured interviews in a private room at the clinic between September to November 2019. Interview questions were designed to explore patients’ diverse weight management experiences. The semi-structured question (see Appendix A) was created by PI based on clinical experiences and informed by relevant literature.18-20 Following the first two interviews, the guide was reviewed and refined to improve clarity and to expand questions that elicited in-depth patient responses. Interviewers were audio recorded and transcribed verbatim by trained research assistants. A female researcher (PhD) with expertise in qualitative methods trained the female research coordinator (MPH) and a female medical student in interview techniques. The research coordinator conducted interviews in both English and Spanish, while the medical student conducted interviews in English. Interviews were conducted until data saturation was achieved, defined as the point at which no new themes emerged and participant responses became repetitive. 21 This project was approved as an exempt study by the University of Texas Health Science Center at San Antonio’s Institutional IRB (HSC20190372E).
Data Analysis
A thematic analysis informed by the SEM was conducted by the research coordinator J.R., bilingual in English and Spanish with public health background, one female medical student (L.P.), and one male premedical student (S.A.). The team completed the analysis using the Braun and Clarke (2006) Methodological framework.22-24 In the first step, the team spent time becoming familiar with data and documenting observations. In step 2, the team assigned preliminary codes. Thirty percent of the transcripts were coded as a group to ensure initial coding agreement and consistency. The remaining transcripts were analyzed independently using preliminary codebook created. The research team met biweekly to discuss the coding process, ensure consistency, and resolve discrepancies. Both inductive and deductive approaches were employed as codes were generated from the data, while relevant literature related to the SEM was used to refine the coding framework and provide additional insight into emerging patterns at the individual or intrapersonal (e.g., identity), interpersonal (e.g., influence of social networks), and community (e.g., social norms) levels.25,26
In step 3, the research team searched for themes by systematically reviewing codes and organizing them into potential themes and subthemes.
Demographics
In step 5, the research team met to discuss defining and naming themes, along with identifying representative quotes. Themes were also reviewed and refined in relation to the SEM. Finally, in step 6 themes were organized into a report and compared to findings from previous literature. Throughout each phase, the PI reviewed progress, guided refinements, and approved modifications. Qualitative Analysis was conducted using ATLAS.ti and demographic statistics were analyzed using IBM SPSS Statistics v29.0.2.27,28
To address bias, our data methodology involved a reflexive approach to our research. While it is impossible to set aside one’s previous knowledge, the researchers adopted a bridling approach. 29 Bridling acknowledges that both interviewer and interviewee are biased and that our perspectives impact our research but that we are able to “slow down” the process of understanding to allow the experience to be seen with cognitive flexibility.30,31
Results
Demographics
Eight participants completed interviews. Majority (62.5%) of participants were females, identified as white (75%), Hispanic (62.5%), making less than $1500 per month (75%), had high school education or less (62.5%), most respondents reported participating in country health safety net program (87.5%) and had a mean BMI of 36.1. The minimum age was 18 years and the maximum was 68 years with a mean of 49.13 (median = 50) and a standard deviation of 14.5.
SEM-Theme Alignment
Theme 1: Previous Lifestyle Changes
Participants were asked about their experience with weight management and any previous methods used. Many described a long history of experimenting with the various methods that were typically ineffective. Participant 1 below identifies their personal list of previous strategies used to manage their weight.
I tried everything…anything you saw on TV. Uhm, shakes. I did all kinds of, like, the Slim
Fast. I did all those kind of shakes… starved myself. Nothing. Uhm, eat once a day.
Didn’t help. Uhm, took out, like, the breads and stuff like that, it didn’t help.” Patient 1
Other methods included alternative medicine along with commercialized strategies. These varied from B12 injections, “ear tapes” or acupuncture methods that press on outer ear, supplements, Herbalife shakes to replace meals. Patient 2 describes a previous method that he perceives led to health consequences.
That is a method that says zero carbohydrates, but they give you a shake and give you a pill. Every eight days I went and they gave me an injection and that injection they say is for you to burn abdominal fat…. I lost 35 pounds almost in four months…from somewhat 230 or so many pounds to 200 as in four months…. I paid the first date $ 80 and then only paid $ 25 each week. One injection and I went down,…but that was when my arteries clogged up… but I was thin, and I said, “Holy, why now is that I am thin I have the heart problems? Could it be that there was consequences? Were there side effects?”, Patient 2
Effective weight loss strategies reported by participants consisted on accountability and self-control. Strategies included establishing consistent daily routines, prescribed medication adherence, and maintaining regular sleep schedules. Additionally, patients described practices such appropriate portion sizes, avoiding late-night snacking, routine regular physical activity, and tracking food intake through diaries. I hold myself accountable for everything that I put in my mouth and I record it…it really is helpful. And so, I do that at home for myself. And it helps me keep track of what I'm eating so I can see, “This is what I had for breakfast, this is what I had for a snack, this is what I had for lunch, whatever.” But I hold myself completely and totally accountable. I know that if I eat that, that’s going to work against me, so I don't eat it. I just simply don't eat it. – Patient 4
Theme 2: Consequences of Obesity
Patients reported obesity-related health risks, either perceived or confirmed from a health care clinician. Respondents reported comorbidities such as type 2 diabetes, cardiovascular events (e.g. stroke), mobility limitations. Patient 4 describes how obesity contributed to the development of osteoporosis, which has decreased their mobility and led to their upcoming knee surgery.
“I'm facing major surgery. It's painful surgery and I'm not looking forward to…I'm only
48 years old and I'm in a wheelchair. Because- but I blame no one but myself. I'm too young.” Patient 4
Patients discussed how their current health and weight affect their psychological well-being, including their energy levels, mood, and self-perception.
My appearance means a lot to me because I’m a flight attendant and I am aware of our we present ourselves and how they perceive us. It is a big factor for me and some of us that work in the industry. Patient 8
Theme 3: Barriers Towards Weight Loss
Participants reported a variety of environmental, time commitments, physical, social, and financial barriers, they experience when attempting to make lifestyle changes. Due to these barriers, they reported feeling limited in the extent of changes they could make in their daily life. Participant 7 attributed their depression to disruptions in metabolic functioning, reporting that it has limited their ability to observe changes in weight.
…I'm doing pretty good on what I eat. I don't know if it's because I'm so depressed and emotional and everything that it's not letting me lose it… Yesterday I ate so much. I only eat little things, but I feel like my metabolism is not burning enough. I was just keeping it there. Patient 7
Participant 9 reported that their social network, particularly family, influences negative dietary habits through constant exposure to unhealthy foods and not accommodating their dietary choices.
My family….They don't like to eat healthy. [laughs]They're always eating out, eating late, going out to dinner late, you know. And it's like chips and stuff like that… I would drink a lot of water, they're always drinking a lot of soda, constantly…. It was never accommodating and just more or less, it's always a factor, like it's a burden…
Patients also face socioeconomic challenges towards implementing positive health behaviors. Patient 6 describes their feelings of being financially limited to the foods they purchase due to depending on fixed disability payments.
“Because I’m on disability. Some of my friends have regular jobs and they say. this week I’m going to work a few more hours to make a little bit more money. What I get is what I get… There’s only certain [foods] that I can get.” Patient 6
Another concern is the limited or insufficient understanding of what constitutes an effective and healthy weight loss strategy. Patients described gaps in their knowledge of health and in their ability to define healthy eating. Participant 2 shares “Previously, perhaps I did not have a good orientation on how to lose weight…or how to feed myself.”
Theme 4: Motivation for Managing Obesity
Patients identified several personal motivators for managing obesity, with many emphasizing the importance of weight loss to improve mobility, overall health, and the management of chronic conditions. For example, Participant 6 described their primary concern as improving dietary habits to better manage diabetes, noting that “diabetes affects you in a lot of ways.” Some participants also expressed concern about becoming a burden to loved ones if declining mobility limited their independence. Participant 3 shares “Living a life as an inconvenience is not a life…I want to be healthy.”
Observing the experiences of others, particularly within their social networks, emerged as another key motivator. Three participants cited witnessing severe obesity and related health complications among family members as influential in shaping their own weight management efforts. As Participant 7 explained, seeing relatives with significant weight-related health issues prompted their desire to avoid similar outcomes.
Yes, because I had my niece, she's 37 years old and she's big, she's like 500 pounds [who has had health problems]. Our nephew that's like maybe 600 pounds, 500 pounds almost. And to me, I look at myself like this I'm like, “It's time for me to lose weight.” I think that's what kind of makes me say, “I'm not going to gain that much” Patient 7
Additionally, participants reported that observing successful weight loss, either in themselves or other, served as positive reinforcement. Participant 1 reports “when I started noticing the weight loss, that motivated me. Like, I’m like, okay, I can do this. I can do this.”
Socially driven motivations were also prominent. One participant described a strong desire to improve energy and mobility to be able to physically engage with their grandchildren. Participant 4 shared that their granddaughter served as a powerful source of motivation, particularly when their activities were limited by her energy levels.
I have a almost-two-year-old granddaughter and she literally was my drive… When she started walking, she would come over and grab my hand and she wanted me to walk with her and I couldn't walk with her…. I can't let her grow up and I can't walk with her or do anything with her.” When things got tough, I would look at her. I have her picture on my phone and I’d just look at her … My son and his wife just had a baby a few weeks ago, so now I have two granddaughters. So now I have double the motivation. ‘Cause I want to be an involved grandmother. Patient 4
Theme 5: Levels of Support
Patients describe various levels of support from social networks and the health care team to make lifestyle changes. Social support includes instrumental and emotional support. Participant 3 shares their partner is “satisfied” with their diet changes, and in fact “appreciates it.” Patient 5 gives credit to his mother cooking healthier meals for household when he decided to change his diet.
Patients that were successful in managing their obesity reported having health care team members guide appropriate and effective changes.
“I really needed the support. I have my family behind me… I needed to have the support of a doctor and a behavior- dietitian and everybody making sure I do it right. They were able to give me tips and make sure that I was doing everything correctly to do it safely.” Patient 4
Theme 6: Clinician Approach
Participants reported a variety of preferences and responses when asked how health care physicians should approach the topic of obesity with their patients. Some patients preferred directly address the topic with them as they were unaware of the reality and severity. Patient 8 takes the perspective that physicians should be straightforward as they would with any other condition.
Because really, if you were to tell somebody they had cancer, you got to tell them right then and there. I mean, just tell them, “You know what, hey, you're obese.” Why sugarcoat it when eventually, someone's going to be-- It's common sense right there, just like, he's got to tell you. Patient 8
Others mentioned clinicians should wait until patients themselves bring up the topic of weight management when they feel ready to make changes.
[If doctor brought up] I would feel bad…‘cause I feel that when I’m ready, I will tell you when I’m ready. This, to me, is just like, uhm, I felt depressed when they would tell me. It’s like somebody calling other people fat, you know. We know we are because we see ourselves in the mirror every day. We don’t need someone else to tell us. You know? Patient 1
However, many agreed that clinicians should approach the topic by discussing obesity and its connection to potential or current risk of comorbidities (e.g., hypertension, diabetes, etc.) and health consequences. Patient 7 mentions shares “I had pain in my leg, [and the doctor] recommended that it’s good to lose weight because that may be causing the pain I have.” Therefore, the patient was receptive to making changes.
Additionally, some patients emphasized the importance of being actively connected to resources and practical strategies to support their weight management efforts, rather than receiving only passive or general guidance.
Patient 005: I wouldn't care. It wouldn't interest me back then…. [They would bring up] that I'm overweight, that I need to lose weight, that I can get like diabetes and all that so- but I never listened… but they all just gave me like, like paper to read, and like facts and stuff, but not actual help.
Discussion
The outcome of the study reveals several important insights into the experiences of individuals managing obesity and weight-related health issues. Through participant narratives, we identified key challenges, motivations, and support mechanisms that shape their weight management journeys. A significant barrier that participants faced in managing their weight was the combination of environmental, financial, and social factors. Participants reported personal goals as a driving force towards weight loss such as improved mobility, functional status, and overall well-being. Patients also voiced their need for support in all areas of their life including their social network along with their health care team. They recognized the role of their health care clinician in approaching the topic and connecting them with resources needed to guide their journey. While some preferred direct and open discussions about obesity and its associated health risks, others felt uncomfortable with the topic and preferred to address it only when they were ready.
Previous literature has confirmed similar socioeconomic barriers to managing obesity in Latino patients. 32 Participants stated financial constraints and lack of access to healthier foods. Based on the studied population, the dependence on low or fixed incomes limited participants’ ability to make healthier food choices. This emphasizes the need for easily accessible resources such as food assistance programs and food pantries that provide healthy and culturally-relevant food items. 33 Additionally, access to health education is important as study participants reported use of non-evidence based weight management programs and gadgets. Similar to Vitagliano et al., the researchers analyzed national Youth Risk Behavior Surveillance System and found Latino youth had roughly 30-40% higher odds of using over the counter diet medication in the previous 30 days compared to white peers. 34
Social support was also identified as an important factor, as participants who had support from their families were more likely to succeed in their weight loss efforts. 35 Latinos in the United States have reported relying on family ties for social support in comparison to non- Hispanic whites. Marquez and colleagues conducted a study to determine the relationship of social support with treatment adherence and weight management in Latinos with diabetes. 36 Social support increased physical activity, particularly when participating with others, which then enhanced weight loss. Prioritizing weight loss strategies and collective effort among Latino families and social networks are an effective strategy for Latino weight management interventions.36,37 Furthermore, financial and social support systems, along with health education are a vital component when approaching weight management.
Participants expressed varying preferences for how health care clinicians should approach the topic of obesity. While some preferred direct and open discussions about obesity and its associated health risks, others felt uncomfortable with the topic and preferred to address it only when they were ready. The majority preferred that clinicians lead in explaining how obesity is linked to various health conditions, rather than just focusing on weight loss. 38 An example of this approach is described by Sheer and Lo called the “5As model,” which outlines steps for improved patient engagement during visits. 39 This model includes: 1. Ask permission to bring up topic; 2. Assess potential factors contributing to weight changes; 3. Agree on SMART (specific, measurable, achievable, relevant and timely) goals; 4. Advise and educate patients while allowing patients to drive the conversation; and 5. Assist/arrange follow-up with patients regarding referrals to community and clinical resources needed. 39
There was consensus that health care clinicians should not only acknowledge the risks associated with obesity but also actively connect patients with resources and support to help them make lasting changes. As referrals are submitted, it is important they have support to navigate that process to ensure they receive the care and services needed. The response from Patient 005, who reported receiving pamphlets with information but no actionable help, illustrates a common frustration with health care interactions that focus solely on information dissemination without accompanying practical support. Other health care team members (e.g., patient navigator, case manager, community health workers, social workers) can facilitate active referrals to ensure patients do access services needed. This does not only apply to community based resources but also highlights the importance of a collaborative team-based approach while implementing medical weight management strategies. 38 There is a clear need for more active involvement from health care clinicians while assessing patient readiness to discuss obesity related comorbidities and offering educational and clinical resources. Examples include: 1: a dietitian to advise on a low-calorie diet individualized to the patients’ lifestyle and preferences; 2: a pharmacist to advise on medications that are weight loss promoting or weight neutral; and 3: a behavioral health clinician to address weight management treatment engagement and motivation. 38
Limitations
While this study has provided valuable insights into the weight loss experiences, low-income Latino individuals, the study’s small sample size and specific geographic location may limit the generalizability of the results. However, the sample demographics may be useful for areas of the U.S. who have similar population demographics. Factors such as cultural, social, and environmental differences can significantly affect a patient’s experience. Additionally, generational differences related to obesity management needs were not discussed in this paper due to the small sample size. Future research would benefit from a broader, more diverse sample to confirm these findings.
Public Health Significance
Aligned with the SEM, this project reinforces that individuals require support from multiple environmental levels to improve obesity management. 13 At the individual level, individuals require health education on healthy diets and physical activity to manage obesity. At the interpersonal level, participants reported family serving a support system throughout their weight management journal and motivating them to live a long and functional lifestyle. At the organizational level, patients described the need for evidence-based approaches. Clinical team members are appreciated as motivators, including how they approach the patient on the topic of obesity. A positive or negatively perceived approach can dissuade a patient, especially if they do not feel ready to make lifestyle changes.
In addition, integration of multidisciplinary teams to educate and guide their weight management journey was reported as facilitators for effectively making positive changes.13,38 At the community level, participants require support for socioeconomic needs, such as financial limitations that can influence dietary choices Additionally, patients would like a strong active connection between healthcare systems and community organizations as one patient reported they prefer active referrals that provide timely connection to needed resources. At the policy level, increased funding and evaluation for integration of evidence-based approaches, multidisciplinary teams, strong clinical and community connections, and community education can facilitate healthy lifestyle choices.17,38
Footnotes
Acknowledgements
Thank you to Dr. Cruz for your guidance on this paper.
Ethical Considerations
The research study was approved by the University of Texas Health Science Center at San Antonio’s Institutional IRB and provided an exempt Determination (HSC20190372E).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a Texas Academy of Family Physicians (TAFP) grant to the University of Texas Health Sciences Center at San Antonio’s Department of Family & Community Medicine.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.