
Abstract
Objective
To explore how primary and community-based healthcare professionals (HCPs) experience supporting adults with congenital heart disease (ACHD) in generalist healthcare settings.
Methods
A qualitative interpretive study was conducted with 18 UK primary care HCPs, including general practitioners and advanced clinical practitioners. Semi-structured interviews were analysed using reflexive thematic analysis.
Results
An overarching theme, balancing knowledge, care and constraint, captured how HCPs supported adults with ACHD while navigating uncertainty, relational responsibility and fragmented systems. Three interconnected themes were identified: navigating uncertainty, reflecting limited ACHD knowledge and infrequent exposure; sustaining relationships, highlighting the role of continuity and familiarity in maintaining care; and working around the system, describing how participants adapted to unclear pathways, inconsistent communication and organisational constraints. Despite limited condition-specific knowledge, participants described recognising concerns, coordinating care and sustaining continuity across fragmented services.
Conclusion
As increasing numbers of adults with ACHD receive care beyond specialist centres, primary and community-based HCPs play a crucial role in recognising concerns, coordinating care and maintaining continuity. Participants’ accounts highlight the often-unseen relational and coordinating work required to keep patients connected to appropriate care despite uncertainty and organisational constraints. Strengthening ACHD care therefore requires more than condition-specific education; it depends on healthcare systems that facilitate communication, collaboration and shared responsibility across specialist and generalist services.
Introduction
Once associated with high childhood mortality, congenital heart disease (CHD) is now increasingly recognised as a lifelong condition, with advances in medical care contributing to a growing and ageing adult population.1,2 As this population ages, rates of multimorbidity, healthcare use and associated costs continue to rise.3,4 Health systems increasingly seek to manage such long-term conditions in community and primary care settings (first-contact, community-based services within the National Health Service (NHS)), reflecting policy aims to deliver care in “the right place, at the right time, by the right person”. 5
As care increasingly extends beyond specialist centres, healthcare professionals (HCPs) working within community and primary care settings are often the first point of contact for adults with congenital heart disease (ACHD) and play an important role in coordinating access to specialist services. 6 Lifelong specialist follow-up is a central component of ACHD care, yet discontinuity of follow-up remains a recognised challenge and lack of specialist care has been associated with increased morbidity and mortality.6,7 As care increasingly spans specialist and generalist services, primary and community-based HCPs may play an important role in recognising gaps in care, enabling continuity and helping patients remain connected to specialist services.
However, many of these HCPs encounter ACHD infrequently and may have limited condition-specific training or experience. 8 This creates a challenge within generalist practice, where HCPs are required to facilitate care for patients with complex cardiac and non-cardiac needs while navigating unclear referral pathways, fragmented communication and the demands of continuity in long-term care.8-12
While patient and specialist perspectives have been explored, little is known about how primary and community-based HCPs experience caring for adults with CHD. These HCPs occupy a pivotal yet underexamined position within the care continuum, negotiating not only clinical complexity but also uncertainty, responsibility and system pressures. This study addresses this gap by exploring how HCPs in out-of-hospital settings perceive and navigate the challenges of ACHD care, with a focus on how knowledge, relationships and organisational context shape practice when managing an infrequently encountered but clinically complex condition.
Methods
Study Design and Methodological Orientation
This study adopted a qualitative interpretive design to explore how HCPs experience and navigate the provision of care for adults with CHD in primary care. An interpretivist epistemological stance underpinned the study, recognising that participants’ accounts are shaped by social, relational and organisational contexts, and that meaning is co-constructed between researcher and participant.
Reflexive thematic analysis (RTA), as developed by Braun and Clarke (2022), 13 provided the methodological framework for exploring patterns of meaning across participants’ accounts and supported both descriptive and interpretive engagement with the data. This approach was chosen for its suitability in exploring under-researched experiential domains and its capacity to enable both descriptive and interpretive analysis.
Setting and Participants
Participants were HCPs working in United Kingdom (UK) primary care settings and included general practitioners (GPs) and advanced clinical practitioners (ACPs). These roles were selected as they represent key points of contact for adults with CHD outside specialist services.
A purposive sampling strategy was used to capture variation in factors shaping HCPs’ experiences of ACHD care. This included professional role, clinical experience, exposure to ACHD and practice context (including rural or urban setting, socioeconomic deprivation and proximity to specialist services). Participants were also recruited across a range of career stages, enabling exploration of how experience may shape perspectives on ACHD care. These factors were considered because of their potential influence on access to expertise, referral pathways and continuity of care. Recruitment was facilitated through NHS primary care networks representing clusters of general practices and professional contacts. Inclusion criteria were: (1) registered HCPs working in primary care settings, (2) first point of contact for patients.
Eighteen participants were recruited, comprising 11 GPs and 7 ACPs (including nurses, physiotherapists and occupational therapists). Participants had between three months and over 30 years of experience in primary care. Recruitment continued until the dataset was judged to provide sufficient depth, richness and diversity to address the research question. This approach was informed by the principle of information power, 14 whereby sample size is determined by the study aim, sample specificity, quality of dialogue and analytic strategy, rather than by a predetermined numerical target. Consistent with Braun and Clarke’s reflexive thematic analysis, sample adequacy was considered in relation to the generation of rich and meaningful interpretations.
Data Collection
Data were generated through semi-structured interviews conducted between July 2022 and May 2024. Interviews were undertaken virtually via video conferencing to facilitate participation across geographically dispersed sites. Interviews lasted between 30 and 90 minutes.
An interview guide (Appendix 1) was developed through review of the adult congenital heart disease (ACHD), primary care and continuity of care literature, alongside the clinical and lived experience of the research team. The guide was further informed by patient and public involvement (PPI) contributors with lived experience of ACHD, who provided feedback on the relevance, clarity and scope of the topics explored. Questions focused on participants’ experiences of caring for adults with ACHD, perceived challenges, communication with specialist services, care coordination and support needs. The interview guide was tested with primary care healthcare professionals and subsequently refined iteratively throughout the study to improve question clarity, flow and relevance. In line with RTA, the guide was used flexibly to enable participants to introduce issues they considered important to their practice.
All interviews were conducted by the first author (SE). Field notes were recorded following each interview to capture contextual observations, initial interpretations and methodological reflections. Interviews were audio-recorded, transcribed verbatim using transcription software, and checked for accuracy against the original recordings. All transcripts were anonymised prior to analysis.
Data Analysis
Data were analysed using Braun and Clarke’s six-phase reflexive thematic analysis. 13 Transcripts were read repeatedly to facilitate familiarisation with the data before open line-by-line coding was undertaken by SE. Coding was initially semantic, before moving towards more latent and interpretive coding as patterns of meaning were developed. The research team met regularly to explore interpretations, challenge assumptions and facilitate reflexive analytic development. Consistent with RTA, these discussions were intended to deepen interpretation rather than achieve coding consensus.
Coding Framework
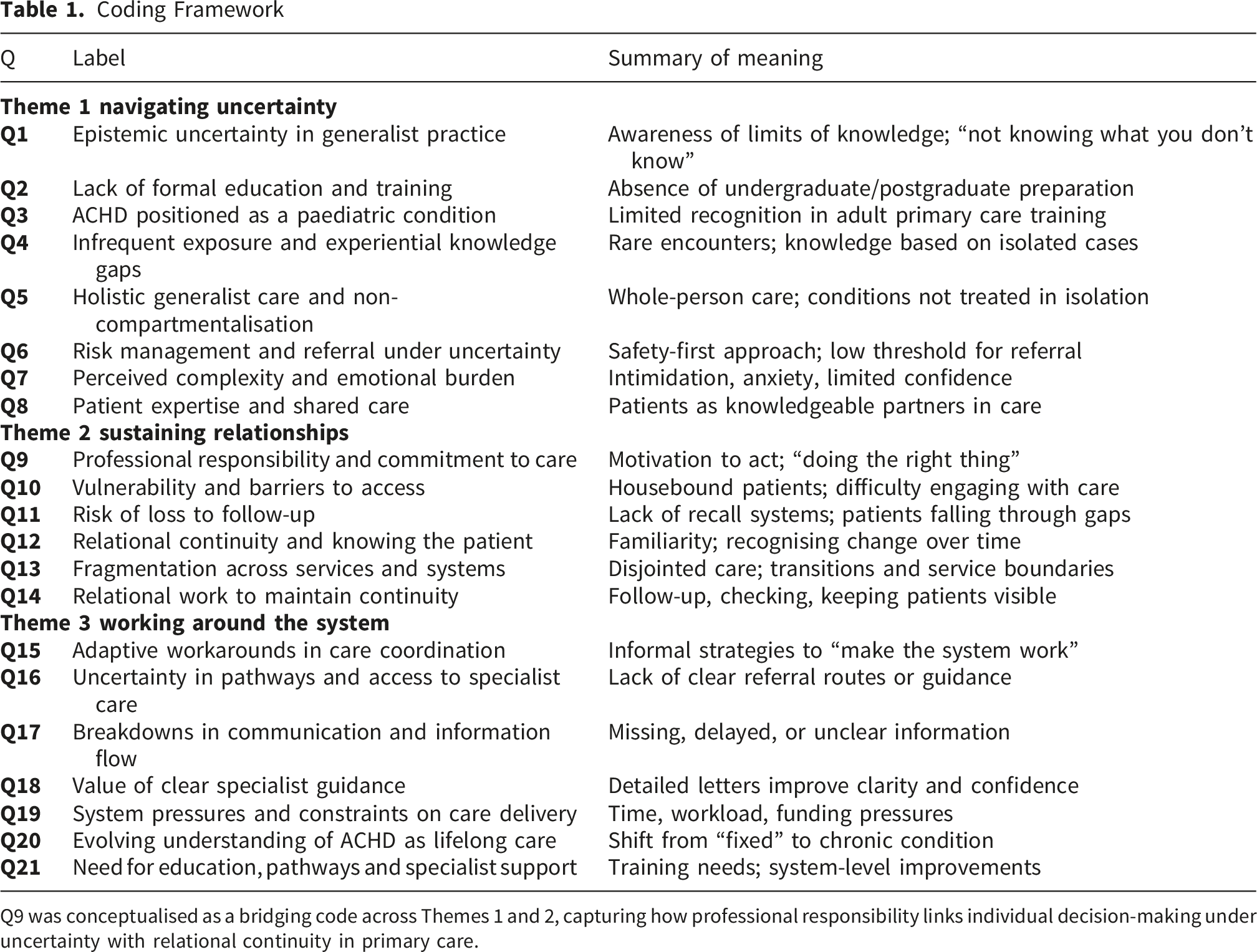
Q9 was conceptualised as a bridging code across Themes 1 and 2, capturing how professional responsibility links individual decision-making under uncertainty with relational continuity in primary care.
Reflexivity and Researcher Positioning
Reflexivity was integral to the study. The lead researcher (SE) is a community-based registered nurse with lived experience of ACHD, which informed engagement with participants and interpretation of the data. Reflective journalling was used throughout the study to support ongoing examination of assumptions and researcher positioning. Participants were provided with information about the study and the researcher’s professional background prior to interview. The researcher’s personal experience of ACHD was not routinely disclosed during interviews.
Rigour and Trustworthiness
Rigour was supported through prolonged engagement with the data, iterative analysis, clear documentation of analytic decisions and the use of rich illustrative quotations. Detailed descriptions of the study context and participants enable readers to assess the transferability of the findings. The study was reported in line with the Consolidated Criteria for Reporting Qualitative Research (COREQ). 15
Ethical Considerations
Ethical approval was obtained from Health and Care Research Wales (REC reference 22/PR/0370). All participants received written information about the study and provided informed consent prior to participation. Confidentiality was maintained through anonymisation of transcripts and removal of identifiable information. Participants were reminded that involvement was voluntary and that they could withdraw at any time without consequence. Given the potential for discussing emotionally challenging experiences, interviews were conducted sensitively, with participants offered the opportunity to pause or stop at any time.
Results
Illustrative Quotations
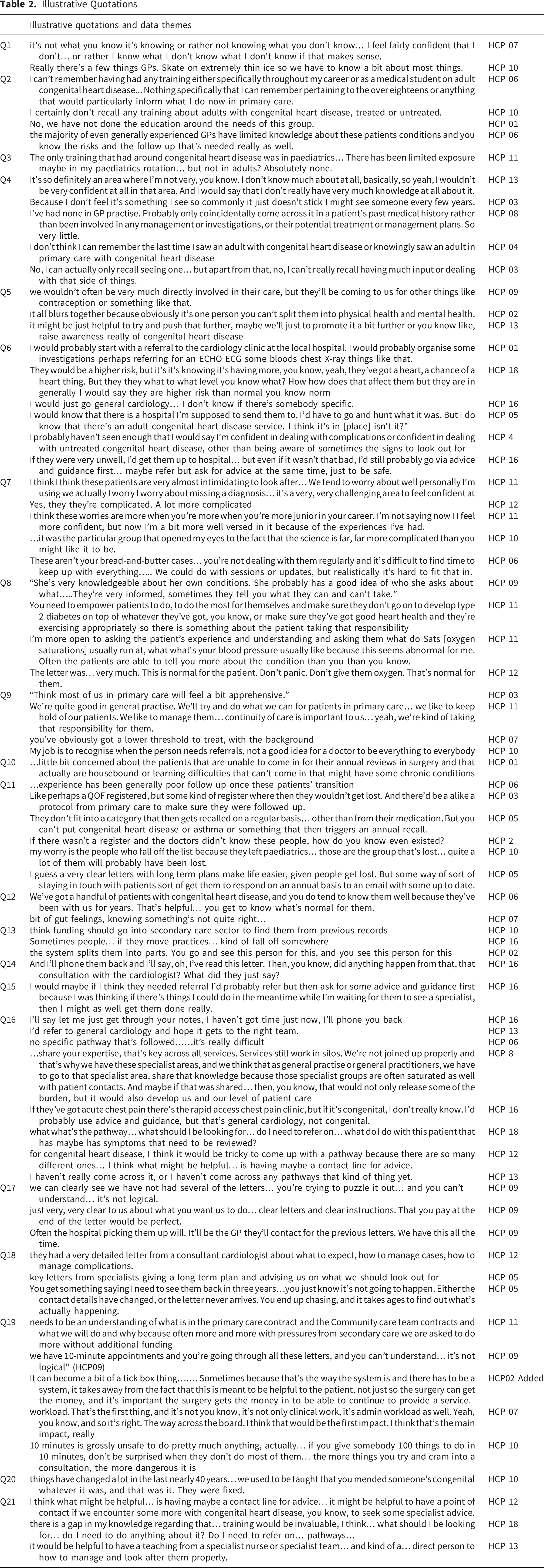
Theme 1: Navigating Uncertainty - You Don’t Know What You Don’t Know Q1
Participants consistently described limited education and clinical exposure to ACHD, shaping both their confidence and emotional experience. Most had received little or no formal training during undergraduate or postgraduate study, learning instead through chance encounters, hospital correspondence or self-directed research (Q2). For many, ACHD was still perceived as a paediatric issue rather than a condition encountered in adult primary care (Q3). Infrequent exposure meant that knowledge often rested on isolated cases, with HCPs relying on analogy rather than structured understanding (Q4). Within this context, participants positioned ACHD within the broader scope of generalist care, describing how patients were often seen for non-cardiac issues and could not be separated into discrete conditions. This reinforced the need for a holistic approach, even when condition-specific knowledge was limited (Q5), highlighting both the complexity of ACHD and their limited confidence in managing it (Q7). Uncertainty carried an emotional toll. Many described feelings of anxiety, guilt and discomfort related to their limited knowledge, alongside concerns about their ability to provide appropriate care (Q7). In response, some HCPs adopted risk-averse approaches, referring more readily for reassurance (Q6), while others demonstrated a form of cautious, proportionate action despite uncertainty. This involved proceeding with initial management or referral while recognising their limits and seeking appropriate support (Q6).
Participants also valued the experiential knowledge that many patients brought, reframing care as a collaborative process (Q8). Drawing on patients’ expertise helped mitigate uncertainty and supported a more collaborative approach to decision-making. Despite these challenges, HCPs described a continued sense of professional responsibility and motivation to act in patients’ best interests, even in unfamiliar situations (Q9). However, managing uncertainty was not solely an individual task, but one embedded within the ongoing relationships that characterise primary care.
Theme 2: Sustaining Relationships – The Glue That Keeps it Together Q14
Participants emphasised their role in maintaining responsibility for patients within primary care, with continuity and familiarity enabling them to recognise changes and support safe clinical decision-making (Q9, Q12). However, many expressed concern that patients could be lost to the system in the absence of recall mechanisms or structured follow-up (Q11). Reliance on patient-initiated follow-up was seen to disadvantage those with additional vulnerabilities, particularly individuals who were housebound or had needs that limited their ability to engage (Q10).
Relational continuity enabled HCPs to build familiarity and recognise change over time (Q12). However, this continuity was increasingly undermined by fragmentation across services and transitions between providers (Q13). These disruptions weakened therapeutic relationships and risked loss of contextual knowledge. Despite these pressures, participants demonstrated persistence and commitment, repeatedly returning to the importance of relationships as the glue that keeps it together through small but significant relational acts that kept patients visible within the system (Q14). These findings suggest that continuity is not simply organisational, but a relational process actively sustained through everyday practice.
Theme 3: Working Around the System - You Just try to Make the System Work/Bending the System Q15
Beyond individual interactions, relational work was shaped and often constrained by wider system factors. At the organisational level, HCPs identified system barriers that constrained coordination and consistency. Many were unsure of referral routes or how to access specialist advice, resulting in variable approaches across practices (Q16).
Communication with secondary care was frequently described as inconsistent, delayed or incomplete (Q17). These gaps left HCPs uncertain about ongoing management and frustrated by the time required to chase missing information. When collaboration worked well, it transformed care, with timely and accessible communication from cardiology improving efficiency and confidence (Q18).
Systemic pressures such as increasing workload, limited consultation time and funding pressures further affected morale and capacity (Q19). Despite these challenges, participants reflected on how approaches to care have changed over time, particularly in how ACHD is understood as a lifelong condition (Q20). Participants offered practical solutions to strengthen confidence and consistency, including clearer referral pathways, concise cardiology summaries and targeted education (Q21). They described bending rigid processes or finding informal routes to specialist advice, adaptive strategies aimed at making the system work for patients (Q15).
Discussion
This study highlights the often-unseen work undertaken by primary and community-based HCPs to support adults with ACHD beyond specialist services, including managing uncertainty, sustaining continuity and coordinating care across systems. Participants described balancing limited familiarity with ACHD against ongoing responsibility for recognising concerns, coordinating care and maintaining continuity within fragmented healthcare systems. The findings suggest that the difficulties experienced by HCPs were not simply the result of limited condition-specific knowledge. Rather, they reflected the demands of sustaining responsibility for patients within systems that were often difficult to navigate and poorly connected across organisational boundaries.
This tension was particularly evident when participants were required to coordinate and sustain care despite limited familiarity with ACHD. Consistent with previous research, ACHD was experienced as an infrequently encountered but clinically complex condition within generalist practice, characterised by limited education and infrequent exposure.8,12 Uncertainty was therefore not simply a gap in knowledge, but an ongoing feature of practice. Participants described concerns about missing important clinical information, uncertainty regarding referral pathways and discomfort when working beyond familiar areas of expertise. These experiences resonate with descriptions of moral distress, in which clinicians are unable to act in accordance with what they believe to be the right course of action because of factors beyond their control. 16
Although participants rarely articulated these experiences in explicitly ethical terms, their accounts reflected concern about whether they were able to provide the care patients needed, particularly when they could not access timely specialist advice, lacked clarity regarding ongoing management or worried that patients might become lost between services despite their efforts to maintain continuity of care. Nevertheless, participants continued to coordinate care, seek solutions and support patients over time, reflecting a form of moral agency expressed through efforts to act in accordance with professional and ethical values despite system constraints. 16 Participants demonstrated this through efforts to coordinate care, advocate for patients and maintain continuity across organisational boundaries. When communication and collaboration supported them, they described confidence and purpose. When relational continuity was disrupted by fragmentation across services and administrative barriers, HCPs described feeling constrained in their ability to act. The findings suggest that moral agency is not simply an individual characteristic but is supported through relationships, communication and organisational structures that enable HCPs to fulfil their responsibilities effectively.17-19 While moral agency highlights how participants sought to act responsibly within existing constraints, their accounts also raised broader questions about where expertise, decision-making and support should sit across primary and specialist services.
Participants described recognising concerns, coordinating care and sustaining continuity while simultaneously relying on specialist expertise when required. Viewed through the lens of subsidiarity, these accounts highlight both the potential and the limitations of locating responsibility within primary care. Subsidiarity proposes that decisions should be made as close as possible to the patient, while higher levels of expertise provide support when needed.20,21 While primary care professionals were often best placed to provide continuity, holistic support and coordination, they frequently described relying on informal routes, personal relationships and individual initiative to bridge gaps in care. These findings suggest that responsibility can be effectively located within primary care only when accompanied by timely access to specialist expertise, clear referral pathways and supportive relationships across organisational boundaries.
Continuity emerged as a key process through which HCPs sustained care despite limited ACHD familiarity and organisational constraints. Familiarity with patients and ongoing therapeutic relationships enabled recognition of change, coordination of care and maintenance of patients’ visibility within complex healthcare systems. Consistent with previous evidence, continuity supported both patient engagement and clinicians’ capacity to act.22-24 However, participants described continuity as dependent on individual effort and informal workarounds, making it vulnerable to disruption.
The findings highlight the interdependence of generalist and specialist expertise in supporting adults with ACHD. Participants valued specialist knowledge but described the greatest benefits when communication was timely, accessible and collaborative. Effective care appeared to depend not only on specialist expertise, but also on the relationships through which knowledge, responsibility and support were shared across services. These findings suggest that opportunities for communication, shared learning and reciprocal exchange between specialist and generalist practitioners may help strengthen coordination and continuity of care.25,26 As increasing numbers of adults with ACHD receive care outside specialist centres, recognising the complementary contributions of both generalist and specialist practitioners will become increasingly important.
Viewed collectively, the findings suggest that the central challenge for primary and community-based HCPs is not simply acquiring specialist knowledge of ACHD but sustaining continuity and responsibility for patients within systems that are often fragmented and difficult to navigate, while keeping patients connected to appropriate care over time.
Implications for Practice
Given growing recognition of ACHD as a lifelong condition associated with increasing multimorbidity and ongoing healthcare needs,9,12 inclusion within established long-term condition frameworks, such as the Quality and Outcomes Framework, could be considered as one potential mechanism to clarify roles, strengthen continuity and better recognise the contribution of primary care to ongoing management. This would support shared accountability across specialist and generalist services rather than shifting responsibility between them. Education should extend beyond clinical knowledge to include reflective and relational approaches that build confidence and support clinicians in navigating uncertainty. System-level improvements should focus on strengthening communication, coordination and opportunities for shared learning. Practical priorities include accessible specialist advice, clear referral pathways, concise care summaries and mechanisms for collaboration between specialist and generalist services, reducing reliance on informal workarounds.25,26 Participants’ accounts suggest that when such structures are absent, continuity becomes dependent on individual relationships rather than established pathways, increasing the risk of fragmentation and loss to follow-up. For cardiovascular nurses, particularly those working in community, outreach or liaison roles, these findings highlight the importance of accessible specialist advice, clear communication pathways and shared care models to support generalist HCPs.
Strengths and Limitations
This study provides novel insight into how primary and community-based HCPs support adults with ACHD, a group underrepresented in existing research. By focusing on generalist practitioners, it captures the realities of managing an infrequently encountered but clinically complex condition at the point of first contact and during ongoing care coordination. The qualitative interpretive design enabled in-depth exploration of how knowledge, relationships and organisational factors shape practice, while reflexive thematic analysis and team-based discussion supported analytic rigour.
Participants were recruited from a single region of England and experiences may differ in areas with alternative service configurations or access to specialist ACHD services. Many reported infrequent exposure to ACHD. However, this reflects routine practice in community settings and was central to the study’s focus on generalist care. The study explored HCP perspectives only, and future research should consider how these experiences align with those of adults living with ACHD.
Conclusion
Primary and community HCPs play a vital role in the lifelong care of adults with ACHD. Their accounts highlighted the often-unseen work involved in navigating uncertainty, sustaining responsibility and preventing patients from becoming lost within fragmented pathways of care. Strengthening this role requires more than condition-specific education alone. It depends on healthcare systems that support communication, collaboration and continuity across organisational boundaries, alongside timely access to specialist expertise. The principle of subsidiarity offers a useful framework for understanding how care can be delivered as close to patients as possible while maintaining appropriate specialist support.
As increasing numbers of adults with ACHD receive care beyond specialist centres, effective care will depend not only on clinical knowledge but also on the relationships, coordination and organisational support that enable continuity over time. Recognising and supporting this work may be essential to developing more integrated, sustainable and person-centred models of care for adults living with ACHD.
Supplemental Material
Supplemental Material - Caring for Adults With Congenital Heart Disease in Primary Care: A Qualitative Study of Generalist Health Care Professionals’ Experiences
Supplemental Material for Caring for Adults With Congenital Heart Disease in Primary Care: A Qualitative Study of Generalist Health Care Professionals’ Experiences by Sarah Ellison, Robyn Lotto, Ian Jones, and Philip Moons in Journal of Primary Care & Community Health.
Supplemental Material
Supplemental Material - Caring for Adults With Congenital Heart Disease in Primary Care: A Qualitative Study of Generalist Health Care Professionals’ Experiences
Supplemental Material for Caring for Adults With Congenital Heart Disease in Primary Care: A Qualitative Study of Generalist Health Care Professionals’ Experiences by Sarah Ellison, Robyn Lotto, Ian Jones, and Philip Moons in Journal of Primary Care & Community Health.
Footnotes
Ethical Considerations
Ethical approval was sought and obtained from Health and Care Research Wales (REC reference 22/PR/0370).
Consent to Participate
All participants provided written informed consent.
Consent for Publication
All authors have consented for publication.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was undertaken as part of a PhD supported by a VC scholarship funded by Liverpool John Moores University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is not available due to risk of identification of participants.
Guarantor
Sarah Ellison.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.