
Abstract
Introduction
Exposure to secondhand smoke (SHS) poses severe health risks, yet private residences remain a primary site of exposure. Community Health Workers (CHWs) and Health Education Specialists (HESs) are uniquely positioned to advocate for voluntary smoke-free home (SFH) rules. This study assessed the current practices, attitudes, and knowledge of these frontline professionals regarding SFH promotion.
Methods
A cross-sectional survey was conducted among 218 Texas-based professionals (179 CHWs; 39 HESs). Participants were evaluated on their SFH intervention practices using the 5A’s framework (Ask, Advise, Assess, Assist, Arrange), attitudes toward environmental health advocacy, and technical knowledge of SHS risks and SFH implementation strategies.
Results
While 94% of participants reported positive attitudes toward SFH promotion, only 33% (n=72) currently deliver these services. A significant “intervention funnel” was observed: among those currently promoting SFHs, 71% provided advice to create a smoke-free environment, but implementation dropped to 43% for technical assistance and 35% for arranging follow-up support. Knowledge gaps were identified; after adjustment for demographic differences, CHWs remained significantly less likely than HESs to identify risk factors associated with SHS exposure (AOR=0.31, p=.04) and specific strategies for establishing a SFH (AOR=0.44, p=.04), though the overall knowledge score difference was no longer significant after adjustment (p=.18). Notably, CHWs were proportionally more likely than HESs to currently deliver SFH services (36% vs. 21%).
Conclusions
A substantial implementation gap exists between positive attitude and technical practice among Texas CHWs and HESs. To effectively protect vulnerable families, future training must shift focus from general SHS risk awareness to actionable skills, prioritizing the “Assist” and “Arrange” components of the 5A’s framework.
Keywords
Introduction
Exposure to secondhand smoke (SHS), even briefly, can cause adverse health effects in both children and adults. 1 Particularly, children exposed to SHS are at increased risk for sudden infant death syndrome (SIDS), severe asthma, slowed lung growth, and acute respiratory infections.1-3 Among non-smoking adults, SHS exposure is known risk factor for coronary heart disease, stroke, and lung cancer.1,2
The implementation of smokefree laws and policies has contributed to the decline in the proportion of non-smokers exposed to SHS in the United States (U.S.) over the years. However, these protections are inconsistent. As of July, 2025, approximately 38% of the U.S. population is not protected by comprehensive smokefree laws at the state or community level. 4 Furthermore, because these laws rarely extend to private residences, the home remains a primary site of SHS exposure.5,6 This disproportionately affects vulnerable populations, particularly children who spend significant time indoors and lack the agency to control their environment.7,8
The harms of SHS are preventable. The voluntary adoption of smoke-free home (SFH) rules—defined as a total prohibition of smoking inside the living space—is a critical strategy for protecting household members, especially where legislative protections are absent. Although public health efforts have historically focused on clinical smoking cessation, environmental management of tobacco smoke in private living spaces is an underutilized yet essential complementary strategy. Evidence-based SHS interventions, such as the Smoke-Free Homes program, 9 have proven effective in helping families establish smoke-free environments in both homes and vehicles.5,9,10 However, widespread adoption is hindered by several barriers, including low risk perception regarding thirdhand smoke residue, cultural norms, and a lack of practical negotiation strategies within the household.10-12
Community Health Workers (CHWs) and Health Education Specialists (HESs) are uniquely positioned to address these barriers. CHWs, as trusted community members, provide culturally grounded interventions and build strong partnerships within underserved neighborhoods.13-15 HESs complement this approach with expertise in health behavior theory and program evaluation, allowing for the design of systematic, evidence-based environmental health strategies. 16 These frontline workers possess the community credibility and regular access required to engage families in sensitive discussions about household behaviors. In Texas, CHWs are certified through the Texas Department of State Health Services (DSHS), which requires demonstration of mastery across eight core competency areas including communication, interpersonal skills, service coordination, advocacy, teaching, and knowledge of specific health issues. 17 CHW certification training is typically shorter (e.g., 160 hours) or based on field experience and more variable in content than formal degree programs, and may not address environmental health topics such as SFH promotion. HESs, by contrast, hold at least a bachelor’s degree in a health-related field and obtain the Certified Health Education Specialist (CHES) or Master Certified Health Education Specialist (MCHES) credential through the National Commission for Health Education Credentialing, Inc. (NCHEC), which requires demonstrated competency across seven areas of health education practice including assessment, planning, implementation, and evaluation. While these professional pathways differ substantially in their educational requirements and scope, both CHWs and HESs operate within overlapping domains of community health promotion and are increasingly called upon to address environmental determinants of health — including household tobacco smoke exposure — within their existing roles.
Despite their potential, the role of CHWs and HESs has historically been limited to supporting smoking cessation. Their capacity to act as environmental health advocates for SFH remains underestimated, even though such activities fall directly within their professional scope of practice. By leveraging their established relationships, these professionals can provide tailored education on non-smokers’ rights, household rule implementation, and the environmental modifications necessary to sustain a smoke-free life. A widely used framework for understanding and structuring health behavior counseling in community and clinical settings is the 5A’s model, originally developed for smoking cessation counseling and subsequently adapted for a range of health behavior interventions. 18 The five components are: Ask (screening clients about relevant behaviors or exposures), Advise (providing clear, personalized recommendations), Assess (evaluating the client’s willingness or readiness to change), Assist (providing practical support, tools, or strategies to facilitate change), and Arrange (scheduling follow-up or connecting clients to additional resources).
Currently, there is a lack of empirical data regarding the baseline knowledge, attitudes, and practice of CHWs and HESs in promoting SFH. A baseline needs assessment is a foundational step in educational design, ensuring that training programs address specific knowledge gaps and skill deficits rather than covering material the workforce has already mastered.19-21 Without understanding these workforce characteristics, training programs may not meet actual learning needs, either covering knowledge workers already possess or failing to address the specific barriers that prevent effective SFH promotion in practice.
The aims of the current study were to 1. Examine the current practices and attitudes of CHWs and HESs regarding the promotion of smoke-free homes as part of their professional role. 2. Assess their knowledge of SHS health effects and practical SFH implementation strategies.
These findings will inform the development of targeted professional training for CHWs and HESs in Texas, ultimately strengthening their capacity to reduce tobacco-related health disparities through the effective promotion of smoke-free environments.
Methods
Participants and Survey Administration
In 2024, a total of 218 participants were recruited, consisting of 179 Community Health Workers (CHWs) and 39 Health Education Specialists (HESs). CHWs were recruited via email through the Texas Department of State Health Services (DSHS). HESs were recruited via a separate email invitation sent to a member list of certified specialists in Texas, purchased from the National Commission for Health Education Credentialing, Inc. (NCHEC). There were around 5,000 CHWs and 800 HESs in Texas at the time of survey, and thus the final sample of 179 CHWs and 39 HESs represents approximately 3% and 5% of the estimated registered CHW and HES workforces in Texas, respectively, at the time of data collection. Potential participants were invited via email to participate in a research study consisting of a baseline survey followed by the opportunity to enroll in a free, optional online smoke-free homes (SFH) training program; completion of the baseline survey was required to access the optional training modules, but participation in the research itself was voluntary. Electronic informed consent was obtained from all participants prior to study initiation, and participants retained the right to decline to have their responses included in the research analysis and to withdraw at any time without penalty. This study was approved by the Texas A&M University Institutional Review Board (IRB Protocol No. 2023-0600M).
Measures
Current Practice in Delivering Smoke-free Homes (SFH) Education and Services
Participants were asked if they currently provide SFH education and services to their clients. Those who reported currently providing SFH education and services to clients completed 10 additional items assessing practices based on the adapted 5 A’s framework. 18 The 5A’s framework has been adapted here from its original clinical cessation context to the SFH context; for example, ‘Ask’ items assess client exposure to secondhand and thirdhand smoke rather than tobacco use status, and ‘Assist’ refers to helping households establish smoke-free rules rather than facilitating cessation. 18 Items were rated on a five-point scale (Always, Often, Sometimes, Rarely, Never) and dichotomized for analysis to reflect whether a participant performed the practice at least “sometimes.”
Attitudes Toward Delivering SFH Education and Services
Attitudes were measured using five questions on a 4-point Likert scale (Strongly Agree to Strongly Disagree). Responses were dichotomized to reflect agreement (Agree or Strongly Agree). See Table 3 for the full list of items.
Current Knowledge About SFH Education and Services
Participants answered nine multiple-choice questions assessing their knowledge of SFH topics, including the definition of a SFH, benefits of policy implementation, maintenance strategies, and the health risks of SHS (see Appendix 1). A total sum score was calculated based on the number of correct responses.
Demographics
Key demographic information including age, gender, education, race/ethnicity, and years they have worked in a professional role were collected.
Data Management and Analysis
Data were analyzed using SAS version 9.4 (Cary, NC). Descriptive statistics grouped by certification type (i.e., CHW or HESs) were performed to describe the participant characteristics, current knowledge and attitudes concerning implementing smoke-free home policies. For participants indicated currently engaged in delivering smoke-free home services, additional questions regarding practices were examined. Group differences were evaluated using the following tests: Chi-square tests were used to compare categorical variables between CHWs and HESs; Fisher’s exact test was used where expected cell frequencies fell below 5; independent samples t-tests were used for normally distributed continuous variables (e.g, age, knowledge score); and Mann-Whitney U tests were used for non-normal distributions. All tests were two-tailed with a significance threshold of α = .05. Adjusted logistic regression models and a General Linear Model (GLM) were subsequently conducted for each of the nine individual knowledge items and sum score, with age, education level, and race/ethnicity included as covariates. Pearson correlations were conducted between the total knowledge score and binary SFH service delivery status among all participants (n=218), and between the total knowledge score and the practice summary score among the subgroup currently delivering SFH services (n=72). A formal a priori power analysis was not conducted, as this study was designed as a descriptive needs assessment intended to characterize the knowledge, attitudes, and practices of the CHW and HES workforce rather than to test a specific a priori hypothesis.
Results
Participant Characteristics
Demographic Characteristics of Participants (N = 218)
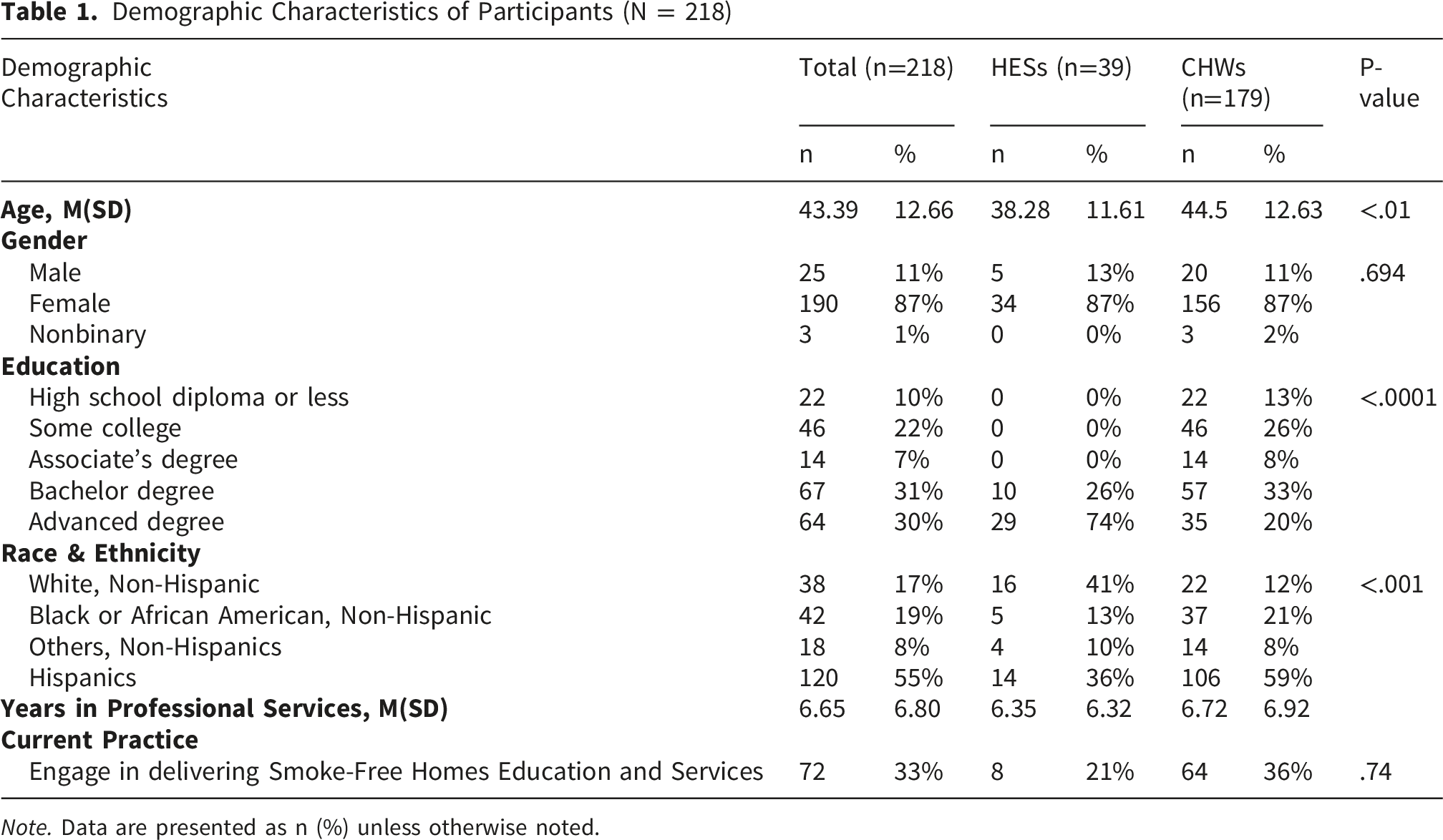
Note. Data are presented as n (%) unless otherwise noted.
Current Practice of Smoke-free Home Education and Services
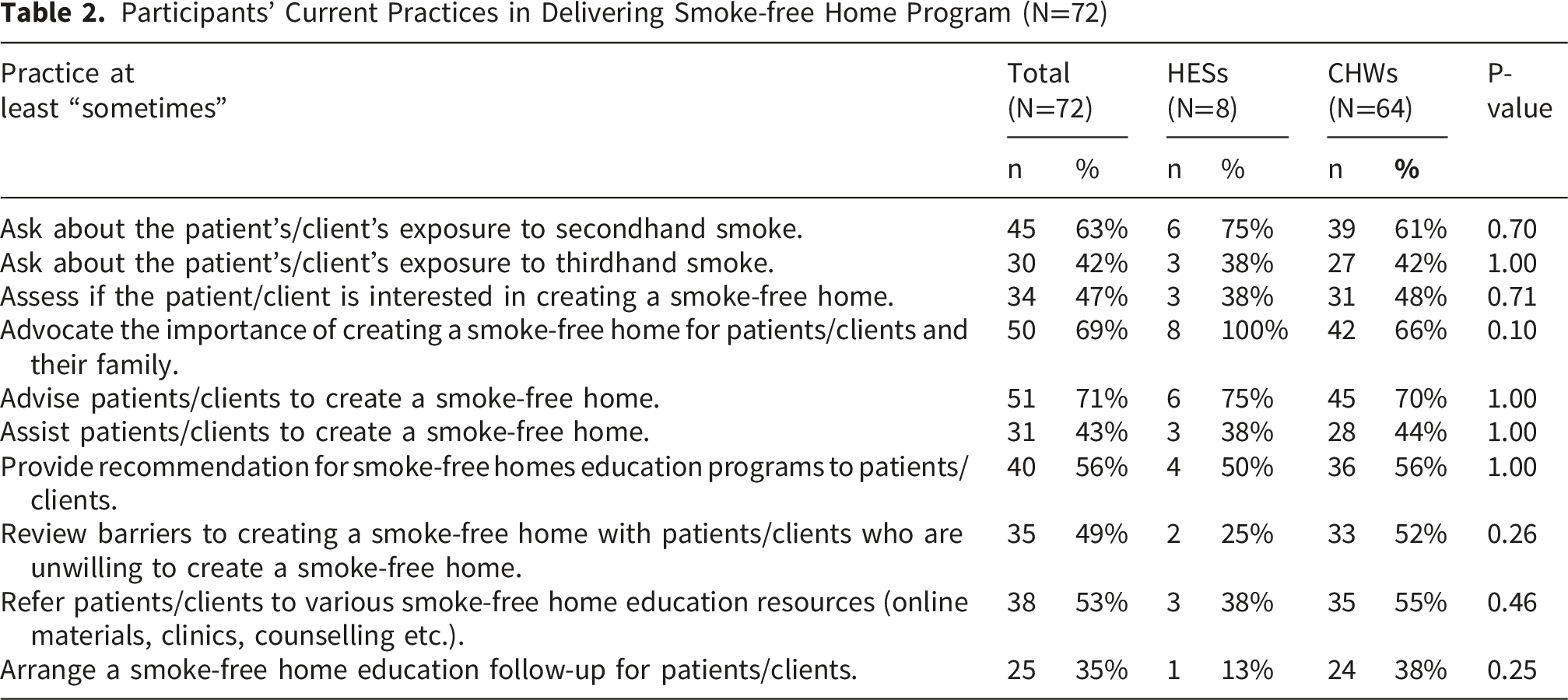
Participants’ Current Practices in Delivering Smoke-free Home Program (N=72)
Current Knowledge and Attitudes Regarding Smoke-free Home Education and Services
Knowledge and Attitude Among Current Community Health Workers and Certified Health Education Specialists in Delivering Smoke-free Home Services (N=218)
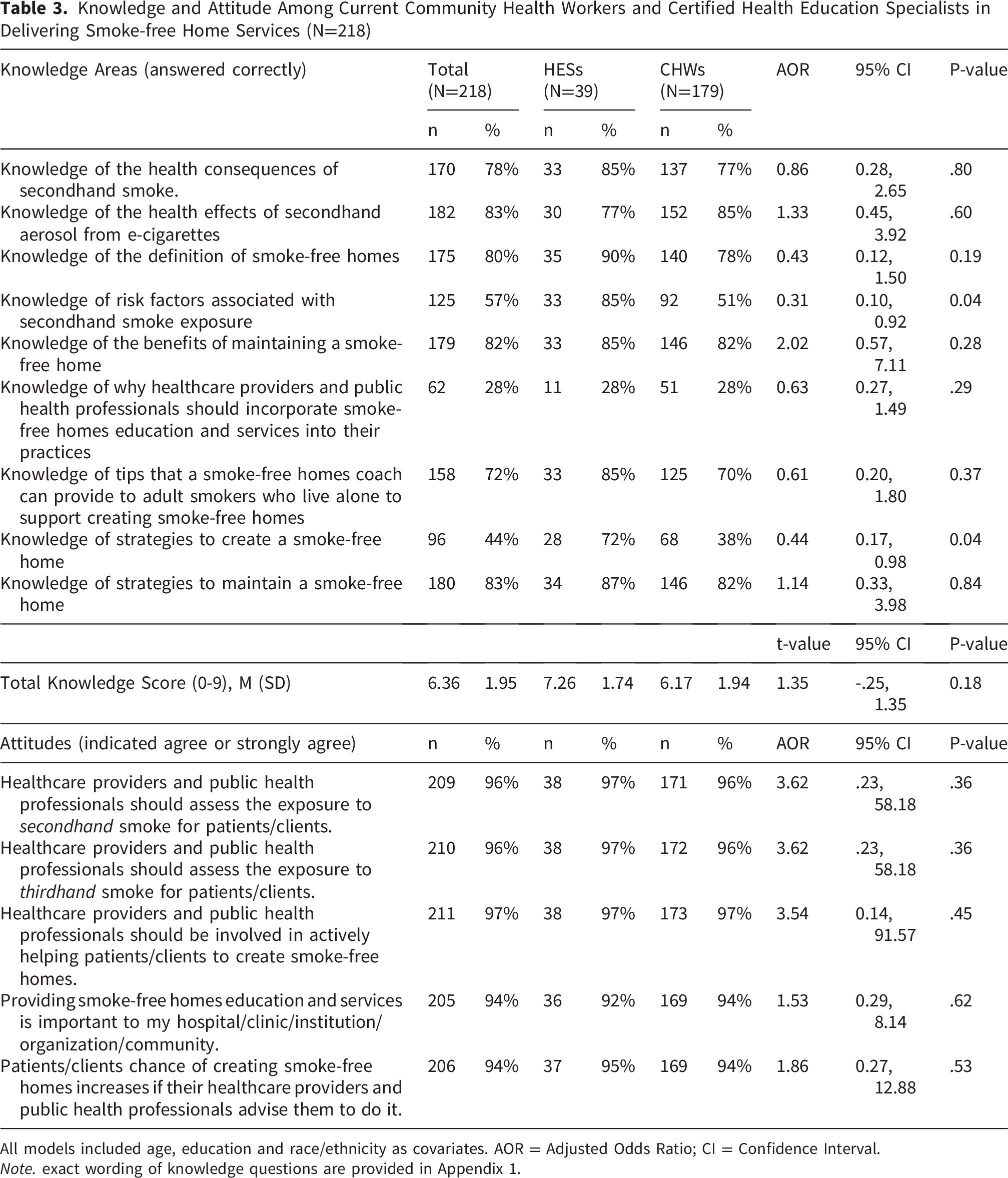
All models included age, education and race/ethnicity as covariates. AOR = Adjusted Odds Ratio; CI = Confidence Interval.
Note. exact wording of knowledge questions are provided in Appendix 1.
In contrast to these positive attitudes, knowledge regarding SFH implementation and risks was mixed, with an overall mean score of 6.36 out of 9 correct answers. Significant knowledge gaps were identified between the two groups. In unadjusted analyses, HESs achieved higher total knowledge scores (M=7.26, SD=1.74) compared to CHWs (M=6.17, SD=1.94, p < .01). However, after adjusting for age, education, and race/ethnicity, this overall difference was no longer statistically significant (t=1.35, 95% CI: -0.25–1.35, p=.18), suggesting that demographic and educational differences between the two groups account for much of the unadjusted gap. In the adjusted logistic regression models, two knowledge items remained significantly different between groups: knowledge of risk factors associated with secondhand smoke exposure (AOR=0.31, 95% CI: 0.10–0.92, p=.04) and knowledge of strategies to create a smoke-free home (AOR=0.44, 95% CI: 0.17–0.98, p=.04), both favoring HESs. Both groups showed a significant lack of knowledge regarding why healthcare providers should incorporate SFH education into their practices, with only 28% of the total sample answering correctly.
To examine the relationship between knowledge and practice, Pearson correlations were conducted between the total knowledge score and SFH service delivery status among all participants (n=218), and between the total knowledge score and a practice summary score — calculated by summing the number of 5A’s items practiced at least sometimes (range 0–10, M=5.27, SD=3.90) — among the subgroup currently delivering SFH services (n=72). Neither correlation was statistically significant (r=0.075, p=0.272 and r=0.064, p=0.595, respectively).
Discussion
This study assessed the knowledge, attitudes, and current practices of Texas-based Community Health Workers (CHWs) and Health Education Specialists (HESs) regarding smoke-free home (SFH) promotion. Our findings reveal a significant implementation gap: despite nearly universal positive attitudes toward secondhand smoke (SHS) protection, only one-third of participants currently deliver these services. This attitude-practice discrepancy suggests that individual attitude is insufficient without structural and educational support for implementation.
The overwhelmingly positive attitude (over 94%) toward the professional responsibility of promoting SFHs is a critical facilitator for future interventions. High levels of perceived responsibility are strong indicators of professional readiness to adopt new practices. 19 However, the fact that only 33% of our sample currently delivers SFH services suggests that motivation alone does not drive behavioral change. This gap aligns with implementation science literature, which demonstrates that individual motivation must be supported by organizational capacity, role clarity, and adequate training.22,23 Several factors may explain this discrepancy. SFH promotion may not be formally integrated into job descriptions, leaving workers without explicit authorization or dedicated time. Furthermore, participants may perceive SFH education as outside their technical competence—particularly if their prior training focused on clinical cessation referrals rather than environmental health counseling. Additionally, competing priorities within already demanding workloads may prevent CHWs and HESs from adding new service components, even those they value. Future research should examine organizational and systemic barriers to SFH integration, including supervisor expectations, workload allocation, and institutional support for environmental health promotion.
Our findings further highlight specific knowledge gaps that hinder the transition from favorable attitudes to effective practice. While participants understood the basic health risks of SHS, they lacked the procedural knowledge required for action—specifically, the “how-to” strategies needed to help families establish and maintain SFHs. Knowledge of implementation strategies is a primary facilitator of successful tobacco control programs. 20
While CHWs demonstrated lower scores on certain knowledge items compared to HESs—particularly regarding SFH implementation strategies (38% vs. 72%)—it is important to note that CHWs were proportionally more likely to be actively delivering SFH services in practice (36% vs. 21%). This suggests that community embeddedness and trusted client relationships, rather than formal knowledge scores alone, are potential key drivers of implementation. The knowledge gaps identified among CHWs therefore represent modifiable training targets rather than fundamental role-based limitations. In Texas, CHWs are the primary bridge to Hispanic and underserved populations—communities that experience disproportionate SHS exposure due to higher smoking prevalence and multigenerational housing arrangements. If CHWs lack comprehensive implementation knowledge, they cannot effectively translate community trust into meaningful SHS reduction. This gap likely reflects differing professional pathways; while HESs often undergo formal academic training in health behavior theory, CHW training is more variable and does not formally require tobacco control or smoke-free home promotion as part of the DSHS-defined core competency framework. 24 This structural omission helps explain why CHWs may achieve lower knowledge to deliver SFH services despite their clear motivation to do so, as evidenced by their higher rate of active service delivery relative to HESs.15,25 Overall, our findings suggest that future training should go beyond teaching what the risks are, but emphasize practical implementation skills, such as negotiating household rules for indoor air quality or addressing resistance from smoking from family members or guests, identifying alternative smoking locations, and problem-solving common barriers to SFH maintenance.
Another key finding is the progressive attrition of intervention intensity across the 5A’s framework. Among participants already promoting SFHs, 71% provided “Advice,” but this dropped to 43% for “Assisting” with technical strategies and only 35% for “Arranging” follow-up. This “funnel effect” indicates that current practices are largely conversational rather than instructional or sustained. This drop-off suggests that workers may feel confident discussing risks but uncertain about providing concrete guidance, or lack systems for structured follow-up. 9 For an environmental intervention to succeed, health educators must provide actionable tools and sustained support rather than one-time advice. Future training should prioritize building competencies in the “assist” and “arrange” components, including developing household action plans, anticipating common barriers, and establishing follow-up protocols that are feasible within existing workflows.26-28
These findings can also be understood through established health behavior frameworks. The Transtheoretical Model (TTM) suggests that behavior change occurs across a continuum of stages — from pre-contemplation through to action and maintenance — and that effective interventions must be matched to a client’s current stage of readiness. 29 SFH promotion may be particularly well-suited to this framework: for smokers not yet ready to quit, a smoke-free home rule offers a meaningful intermediate step that does not require cessation, potentially advancing them along the stages of change by reducing the normalization of indoor smoking. The observation that CHWs and HESs are more confident advising than assisting or arranging follow-up is consistent with TTM-informed practice, where brief advice may shift awareness but sustained support is required to move clients from contemplation to action. The Health Belief Model (HBM) offers a complementary lens, positing that individuals are more likely to act when they perceive a threat as serious, believe the recommended action will reduce it, and feel that benefits outweigh barriers. 30 The knowledge gaps identified in this study — particularly around why providers should incorporate SFH education and how to implement specific strategies — suggest that some CHWs and HESs may lack the confidence and outcome expectations needed to guide clients effectively through these steps. Future training should therefore build not only procedural knowledge but also practitioners’ own confidence in the value and feasibility of SFH promotion. Overall, our findings indicate several priorities for professional training development. Future training should address the identified knowledge gaps in implementation strategies, with particular focus on the “assist” and “arrange” components of the 5A’s framework, including developing household action plans, anticipating barriers, and conducting feasible follow-up Additionally, training should address organizational integration, e.g., helping participants identify how SFH promotion can be incorporated into their existing roles and workflows.
This study has several limitations. The sample of Texas-based professionals recruited through listservs may limit generalizability to other regions. First, reliance on self-reported data may introduce social desirability bias. Additionally, because participants were informed about a potential SFH training program at recruitment, the sample may over-represent individuals already interested in this topic. Furthermore, our sample of 179 CHWs and the 39 HESs represents a small proportion of the workforce practicing in the state. As such, findings should be interpreted as preliminary and hypothesis-generating rather than representative of the broader Texas CHW and HES workforce. Restricting practice questions to only participants who self-identified as currently delivering SFH services may also introduce selection bias. Future studies should administer these items to all participants. The cross-sectional design prevents establishing causal relationships between knowledge and practice. Finally, we did not assess organizational factors, such as supervisor support or institutional priorities, which are critical structural determinants of implementation.
Conclusion
Despite overwhelmingly positive attitudes and strong sense of professional responsibility regarding smoke-free home (SFH) promotion, the majority of Texas-based Community Health Workers (CHWs) and Health Education Specialists (HESs) do not currently provide these services. Among those who do, interventions are primarily limited to brief advice-giving rather than sustained implementation support. Specific knowledge gaps regarding practical implementation strategies represent a significant, yet modifiable, barrier to practice. These findings underscore the necessity of targeted professional training initiatives designed to bridge the gap between “knowing” and “doing.” By equipping these trusted frontline health workers with actionable skills—specifically in the “Assist” and “Arrange” components of the 5A’s framework—we can leverage existing community health infrastructure to reduce secondhand smoke exposure and advance health equity among underserved families in Texas.
Supplemental Material
Supplemental material - From Attitude to Action: Identifying the Knowledge and Practice Gap in Smoke-free Home Promotion Among Texas Community Health Workers and Health Education Specialists
Supplemental material for From Attitude to Action: Identifying the Knowledge and Practice Gap in Smoke-free Home Promotion Among Texas Community Health Workers and Health Education Specialists by Shawn C. Chiang, Ping Ma, PhD, Zihan Zhang, MS, CHW, Lei-Shih Chen in Journal of Primary Care & Community Health
Footnotes
Ethical Considerations
This study was reviewed and approved by the Texas A&M University Institutional Review Board (Approval Number: 2023-0600M).
Consent to Participate
All study participants provided informed consent prior to study enrollment.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this manuscript was supported in part by the Cancer Prevention and Research Institute of Texas (CPRIT) under award number PP200071. The content is solely the responsibility of the authors and does not necessarily represent the official views of CPRIT.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request given appropriate Institutional Review Board’s approval.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.