
Abstract
Introduction
Aboriginal and Torres Strait Islander young people are less likely to utilise health care services, and very little is known about how they engage with and utilise primary health care (PHC) services, particularly in urban areas.
Methods
Descriptive analysis was used to examine health care encounters among Aboriginal and Torres Strait Islander people aged 15-24 years at urban Aboriginal and Torres Strait Islander community-controlled health organisations (ATSICCHOs) in southeast Queensland (SEQ) between 2018 and 2022.
Results
Overall, 12,449 individual young people had at least one encounter at an urban ATSICCHO in SEQ. Utilisation among this population increased from 4,187 in 2018 to 5,314 in 2022. Utilisation of health services were highest among the 15-19-year age group (54%) and higher among girls/women (57%) than among boys/men. There were 127,225 encounters among young people during the study period, increasing from 21,020 in 2018 to 27,029 in 2022. Almost two-thirds of encounters were among girls/women (65%). The median number of encounters for all young people between 2018 and 2022 was 3 (IQR: 1-6); for girls/women, 3 (IQR: 1-6) and for boys/men, 2 (IQR: 1-4). Preventive health (30.7%) and health conditions requiring ongoing management (21.9%) were the two main reasons for encounters; the number of encounters increased over time for all reasons.
Conclusion
Improving utilisation of PHC services remains an ongoing challenge despite increased utilisation and a rise in the number of young people engaging with these services. Models of care within ATSICCHOs, centred on young people, should be funded, trialled, and evaluated to ensure that the health and wellbeing of this population are optimised.
Introduction
Young people aged 15-24 years comprise 19% of the total Aboriginal and Torres Strait Islander population. 1 They are an important group to engage in health care, as they are the future leaders and custodians of Aboriginal and Torres Strait Islander Country, knowledge, culture, language, traditions, and lore. However, there is a generational predicament for primary care providers: how to proactively engage Aboriginal and Torres Strait Islander young people, who, on the whole, are mostly healthy yet experience a higher burden of injury, mental health, and substance use, often leading to acute care and hospitalisations. 2
Accessible, culturally appropriate and quality primary health care (PHC) is essential during this stage of life,3,4 as young people learn to navigate the health system autonomously and identify and address emergent health needs. It also provides opportunities to intervene early and to optimise future and intergenerational health. However, it is known that Aboriginal and Torres Strait Islander young people utilise PHC services less than other age groups within the Aboriginal and Torres Strait Islander population. It is also known that this age group accesses hospitals for care at a higher rate, often double, than their non-Indigenous peers.5,6 The leading causes of hospital admissions among Aboriginal and Torres Strait Islander young people, excluding pregnancy, are injury and poisoning, followed by mental health and behavioural disorders.2,7
PHC typically serves as an initial point of contact with the healthcare system, playing a vital role in addressing health issues early and promoting overall wellbeing. It is estimated that around 80% of excess mortality among Aboriginal and Torres Strait Islander young people is preventable within the existing healthcare system. 8
Aboriginal and Torres Strait Islander Community-Controlled Health Organisations (ATSICCHOs) are PHC services and are a critical component of the Australian healthcare system, providing over three million encounters annually to the Aboriginal and Torres Strait Islander population. 9 ATSICCHOs provide culturally safe, holistic and comprehensive health care predominantly to Aboriginal and Torres Strait Islander communities.10,11 Typically, PHC services are generally designed for the highest users, such as mothers and babies, children, the elderly, and those with chronic or long-term health conditions;5,12 and hence may not be inclusive or appropriate for young people. However, there is increasing recognition of the need for PHC services, including ATSICCHOs, to actively engage young people in health care.13,14
Initiatives such as the Aboriginal and Torres Strait Islander Health Check Medicare Benefits Schedule (MBS) Item 715 are designed to promote access to care for Aboriginal and Torres Strait Islander people. This health check item is funded by Medicare, Australia’s universal health insurance scheme, and encourages regular health checks to improve health and wellbeing.15,16 In 2023, 15.6% of MBS 715 items completed nationally were among people aged 15-24 years, 17 despite this population representing 30% of the total Aboriginal and Torres Strait Islander population. 1 This corresponds to 22.9% of this population having had a health check in 2023, the lowest proportion among any other age group. 17
Adding to the complexity of engaging young people in PHC is that there is limited data available about access and utilisation of ATSICCHOs for Aboriginal and Torres Strait Islander young people.2,8,18 This study addresses this gap by analysing electronic medical record (EMR) data from ATSICCHOs in southeast Queensland (SEQ) to describe Aboriginal and Torres Strait Islander young people’s use of ATSICCHOs between 2018 and 2022.
Methods
This cross-sectional study is grounded in Indigenous research methodologies that prioritise Indigenous knowledges and perspectives while incorporating Western research methods.19-21 The Maiam nayri Wingara Indigenous Data Sovereignty principles were enacted throughout this study. 22 The reporting of our study conforms with the Consolidated criteria for strengthening reporting of health research involving Indigenous peoples (CONSIDER) statement 23 and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline. 24
Positionality
The study was led by SH, a Narungga and Ngarrindjeri man from South Australia, who is a public health researcher and Senior Research Fellow. He has over 10 years of research experience with Aboriginal and Torres Strait Islander communities. JW, a Pitjantjatjara and Narungga man, is an infectious diseases epidemiologist and Director of the UQ Poche Centre, with over 25 years in Indigenous health research. PA is a non-Indigenous adolescent health researcher and head of Adolescent Health and Wellbeing at the Kids Research Institute, working in partnership with Aboriginal and Torres Strait Islander communities across Australia. GM is a non-Indigenous professor in life course epidemiology and women’s health at the University of Queensland, who leads health research initiatives focused on women and non-communicable diseases.
Community Participation and Governance
The study is part of a larger study examining how to strengthen PHC for Aboriginal and Torres Strait Islander young people living in urban SEQ.25-27 Aboriginal and Torres Strait Islander young people’s health and wellbeing, engagement with, and access to and utilisation of health care services, are identified priorities for participating ATSICCHOs.28-30 Approval for the study was obtained from participating ATSICCHOs and their respective research sub-committee, including a waiver of consent to provide EMR data. The study was guided by an Indigenous advisory group comprising Aboriginal and Torres Strait Islander young people. Participating ATSICCHOs were involved in the development of the study and, specifically, in data analysis and interpretation. Approval of the results and final output was sought and provided by the participating ATSICCHOs.
Ethics Approval
Ethics approval was granted by the Human Research Ethics Committees at The University of Queensland (2022/HE001155). The study aligns with the National Health and Medical Research Council’s Ethical conduct in research with Aboriginal and Torres Strait Islander Peoples and communities: Guidelines for researchers and stakeholders. 31
Research Setting
SEQ has the largest urban Indigenous population nationally and one of the fastest-growing Aboriginal and Torres Strait Islander populations. 32 Aboriginal and Torres Strait Islander people aged 15-24 years comprise 19.5% (n=17,737) of the region’s Aboriginal and Torres Strait Islander population. 33 Across SEQ, the Aboriginal and Torres Strait Islander population is serviced by a network of five ATSICCHOs and 19 satellite clinics, all of which bulk-bill under Medicare, so individuals do not incur any out-of-pocket costs. ATSICCHOs in the region were invited to participate in the study, with the following agreeing to be involved: The Institute of Urban Indigenous Health (IUIH), The Aboriginal and Torres Strait Islander Community Health Service Brisbane, Kambu Aboriginal and Torres Strait Islander Corporation for Health, and Moreton Aboriginal and Torres Strait Islander Community Health Service. Participants were Aboriginal and Torres Strait Islander people aged 15-24 years who had at least one encounter, defined as contact with one or more health professionals at the same clinic/service on a single calendar day, at an urban ATSICCHO in SEQ.
Study Design and Data Analysis
Categorised Reasons for Encounters With ATSICCHOs
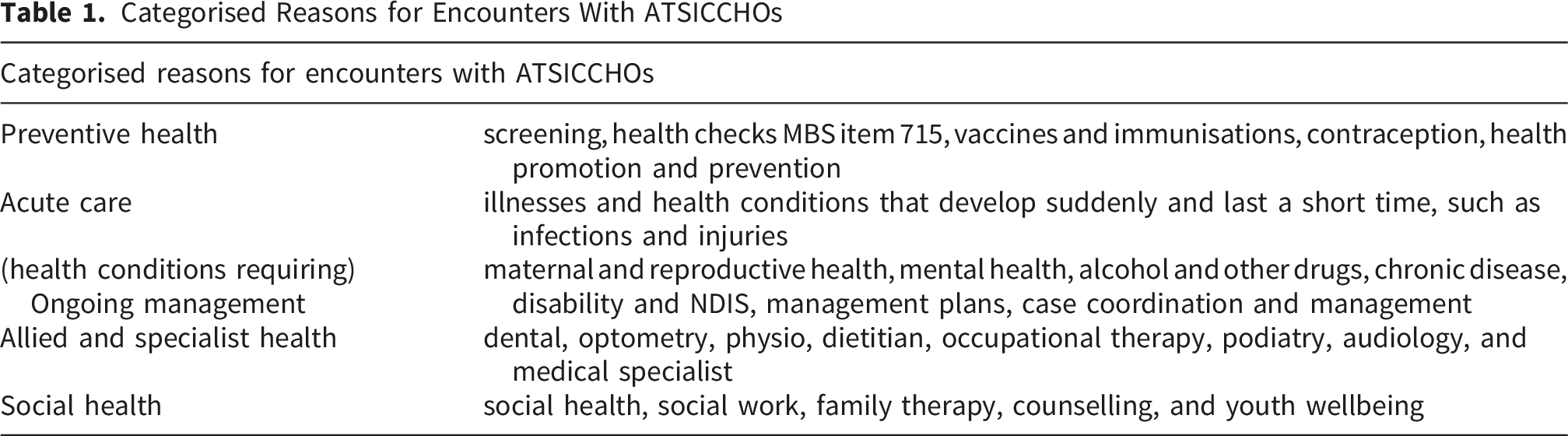
Counts, proportions, and median were calculated for encounters and the reasons for the encounters. Crude rates were also calculated for analysis by age and gender. Counts less than ten are reported as <10 and without a percentage. Data were merged, cleaned and analysed in Stata 18, 34 and graphs were created in Excel.
Total client encounters were calculated using the overall client numbers provided for each service. Population coverage (service utilisation), defined as the proportion of Aboriginal and Torres Strait Islander people aged 15-24 years residing in the catchment areas of participating services who had at least one encounter at the ATSICCHOs in SEQ, was calculated using the estimates from the Australian Bureau of Statistics 2016 and 2021 Census of Population and Housing.33,35 The Aboriginal and Torres Strait Islander population aged 15-24 years was calculated for each service catchment area utilising predefined service catchment postcodes as defined by the service; a linear growth rate was used to estimate populations between Census years, and an age-adjusted undercount was applied. 32
Results
Aboriginal and Torres Strait Islander Young People who used ATSICCHOs in Urban Southeast Queensland
Aboriginal and Torres Strait Islander people aged 15-24 years who accessed ATSICCHOs, southeast Queensland, 2018-2022
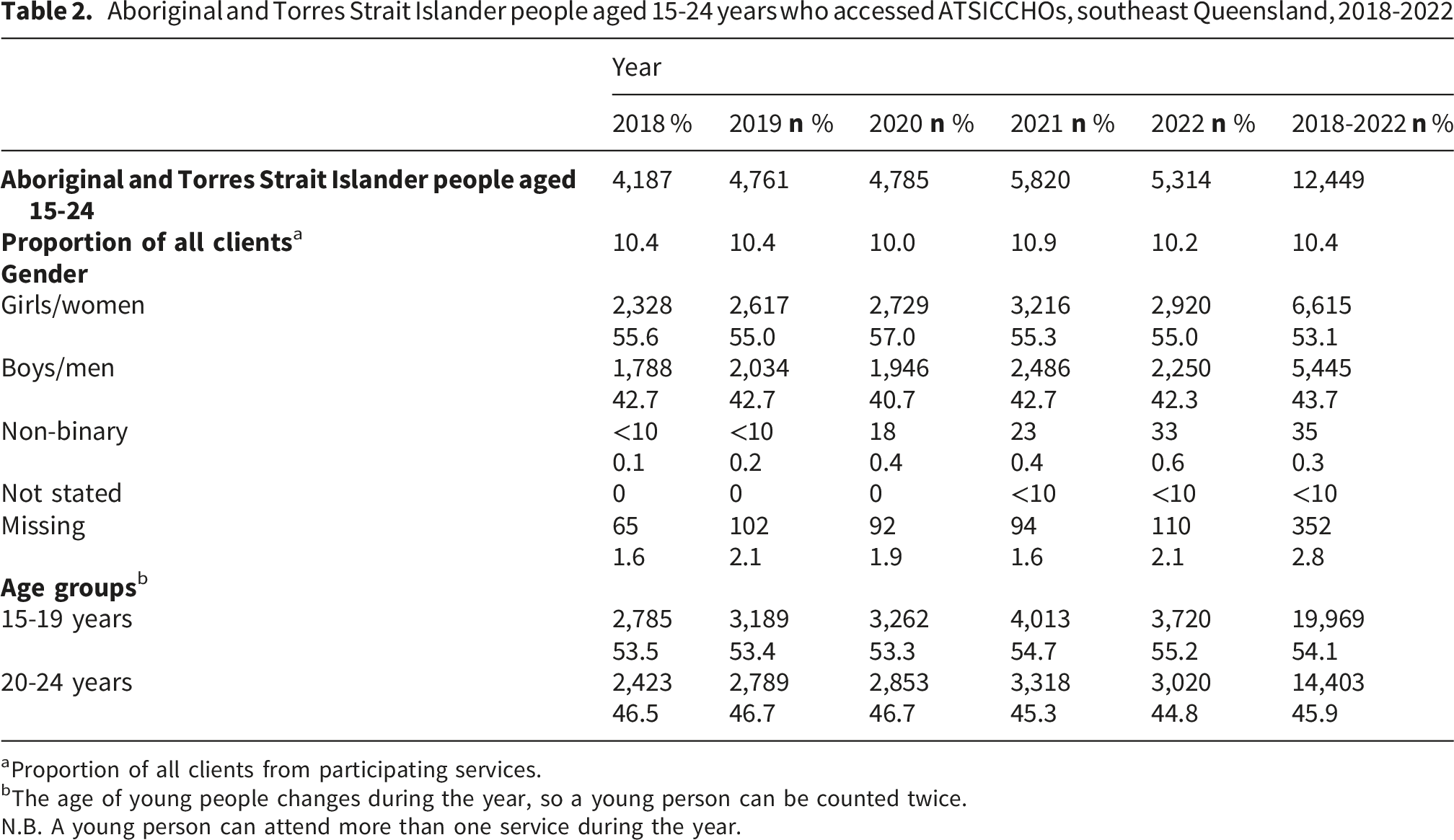
aProportion of all clients from participating services.
bThe age of young people changes during the year, so a young person can be counted twice.
N.B. A young person can attend more than one service during the year.
Aboriginal and Torres Strait Islander Young People by Gender and Age
Over half (56.6%) of the study population who utilised ATSICCHOs were girls/women, with boys/men comprising 43.0% and non-binary 0.4% (Table 2). Young people for whom gender was missing (n=352) were excluded from the gender-based analysis. The number of girls/women and boys/men utilising the services increased over time, resulting in 25.4% and 25.8% increases, respectively, with more individuals attending in 2022 than in 2018. The services also experienced an increase in clients who identified as non-binary, increasing from <10 in 2018 to 33 in 2022 (Table 2). Across all genders, those aged 15 years most commonly utilised services, with utilisation decreasing with increasing age (Supplementary 2). It is worth noting that age changes during the calendar year; therefore, a young person may be counted twice.
Encounters Over Time
Between 2018 and 2022, 127,225 encounters were recorded among the 12,449 individuals in the study population (Supplementary 3). Encounters increased by 28.6% from 21,020 in 2018 to 27,029 in 2022, with 2021 recording the highest number of encounters (Figure 1). The median number of encounters by Aboriginal and Torres Strait Islander young people between 2018 and 2022 was 3 (IQR: 1-6) (Supplementary 4). PHC encounters by Aboriginal and Torres Strait Islander young people aged 15 to 24 years, by year and gender, 2018-2022. N.B. Excludes gender Not Stated as count <10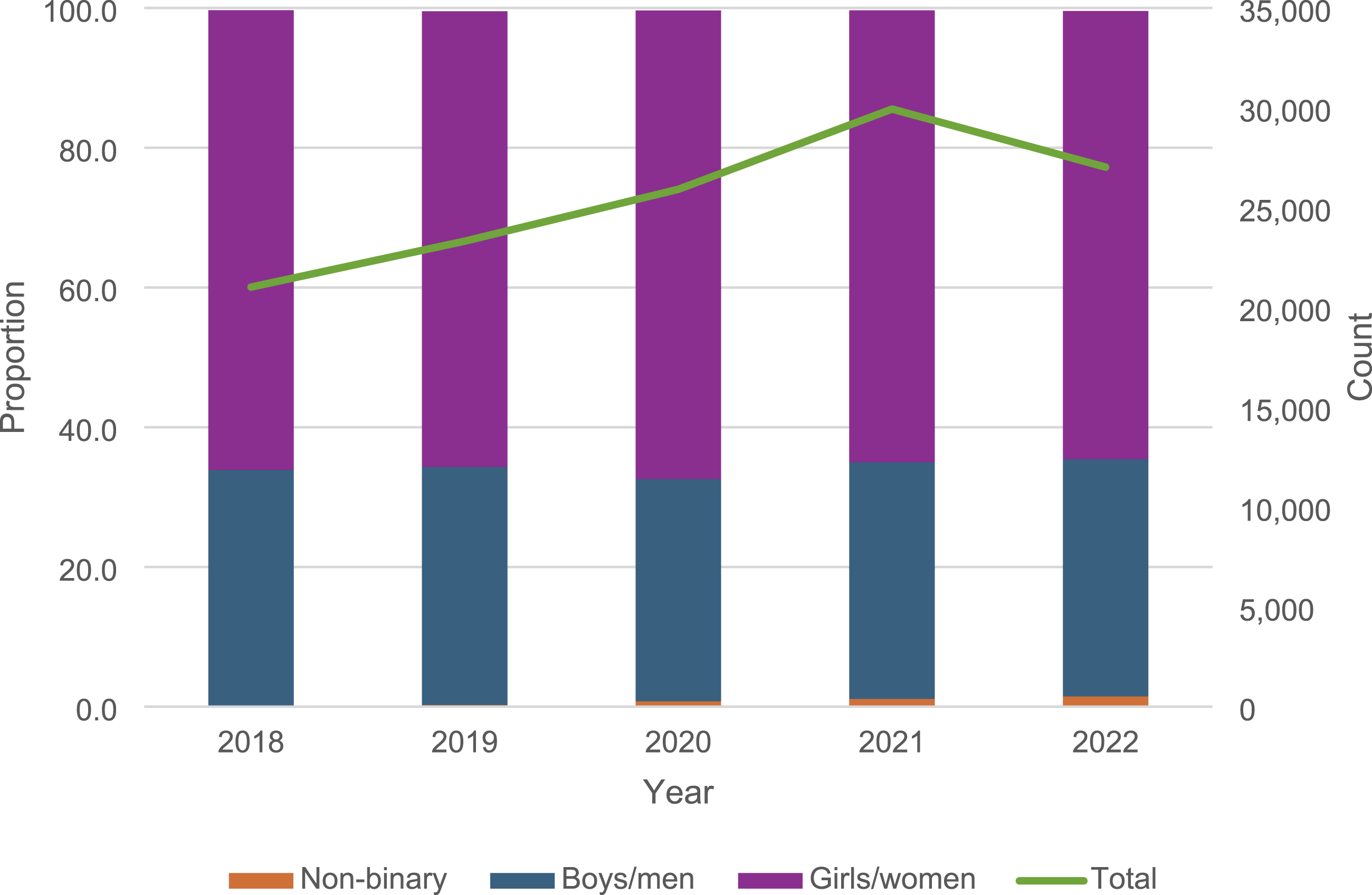
Encounters by Gender and Age
Most encounters were among girls/women (65.3%); however, boys/men comprised 43.7% of the study population but only accounted for 33.5% of encounters (Figure 1). There were similar episodes among 15–19 and 20–24-year-olds, and encounters were highest among 15-year-olds (Supplementary 2). When comparing gender and age, the number of encounters increased with age among girls/women but decreased with age among boys/men (Figure 2). PHC encounters by Aboriginal and Torres Strait Islander young people aged 15 to 24 years, by age and gender, 2018-2022. N.B. Excludes gender Not Stated as count <10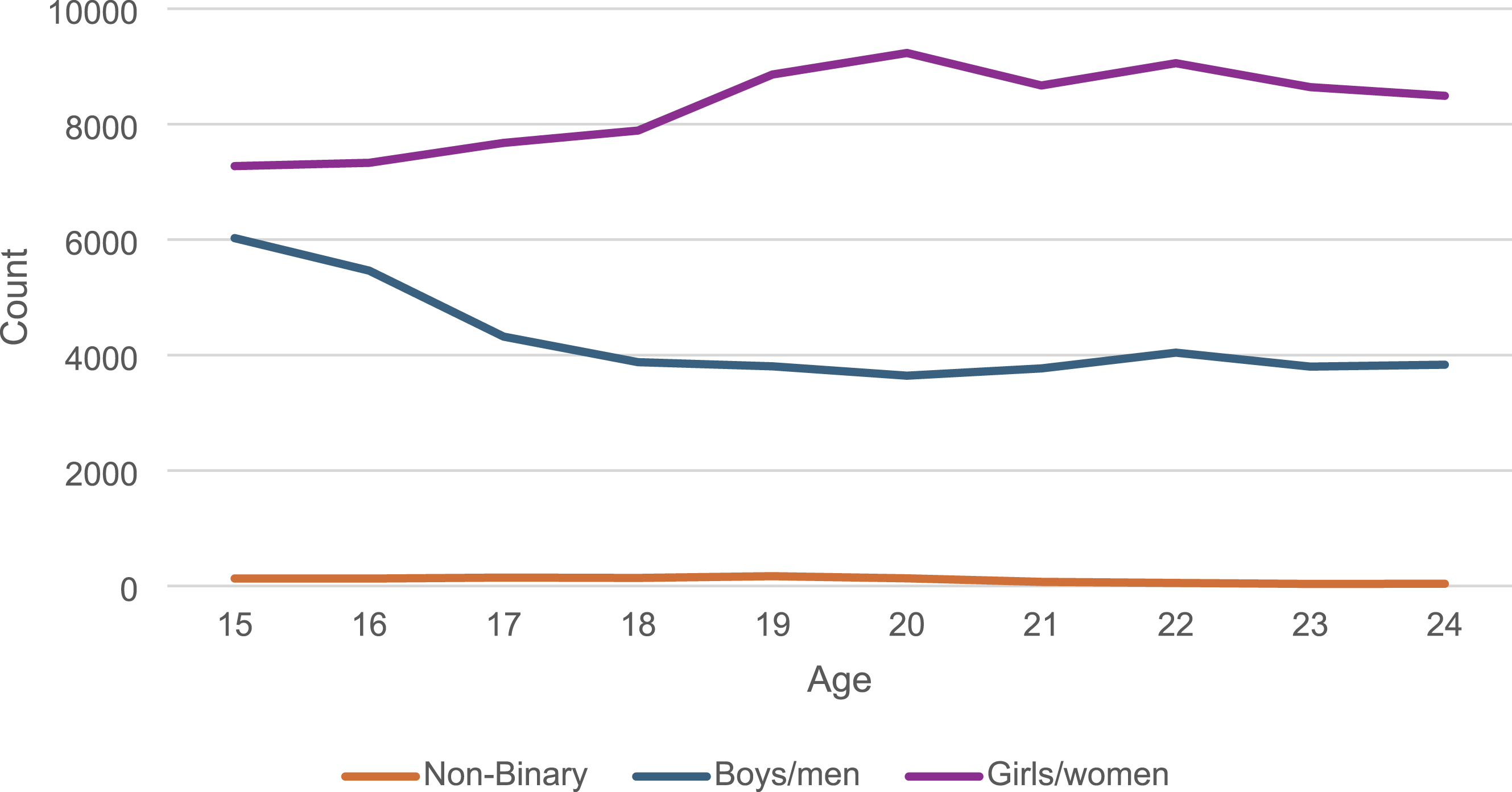
The median number of encounters for girls/women was 3 (IQR: 1-6), compared with 2 (IQR: 1-4) for boys/men and 6 (IQR: 3-15) for non-binary individuals, over the five-year period (Supplementary 3). Variations in the median number of encounters by age and gender over time are shown in Supplementary 4.
Frequency of Encounters
Very few young people (5.9%) utilised an ATSICCHO at least once per year over the five-year period, compared with 8.0% who utilised an ATSICCHO four out of five years, 13.4% who utilised an ATSICCHO three out of five years, and 25.3% who utilised an ATSICCHO two out of five years. Almost half (47.4%) attended an ATSICCHO only once during the five-year study period.
Reasons for Encounters
Overall, preventive health was the main reason for all encounters (30.7% of all encounters), followed by health conditions requiring ongoing management (ongoing management) (21.9%), allied and specialist health (10.3%), acute care (8.2%), and social health (8.2%) (Figure 3). However, these categories do not include pathology, other investigations, and results, which accounted for 7.9% of all encounters. Between 2018 and 2022, all categories of reasons for encounters increased, social health increased by 83.2%, allied and specialist health by 20.1%, acute care by 18.3%, preventive health by 9.3%, and ongoing management by 2.8% (Figure 3). Furthermore, preventive health increased by 46.9% and social health by 34.6% from 2020 to 2021; acute care was the only service that did not increase in 2021. Importantly, there can be more than one reason for an episode of care. PHC encounters by Aboriginal and Torres Strait Islander young people aged 15 to 24 years, by year and reasons for encounter, 2018-2022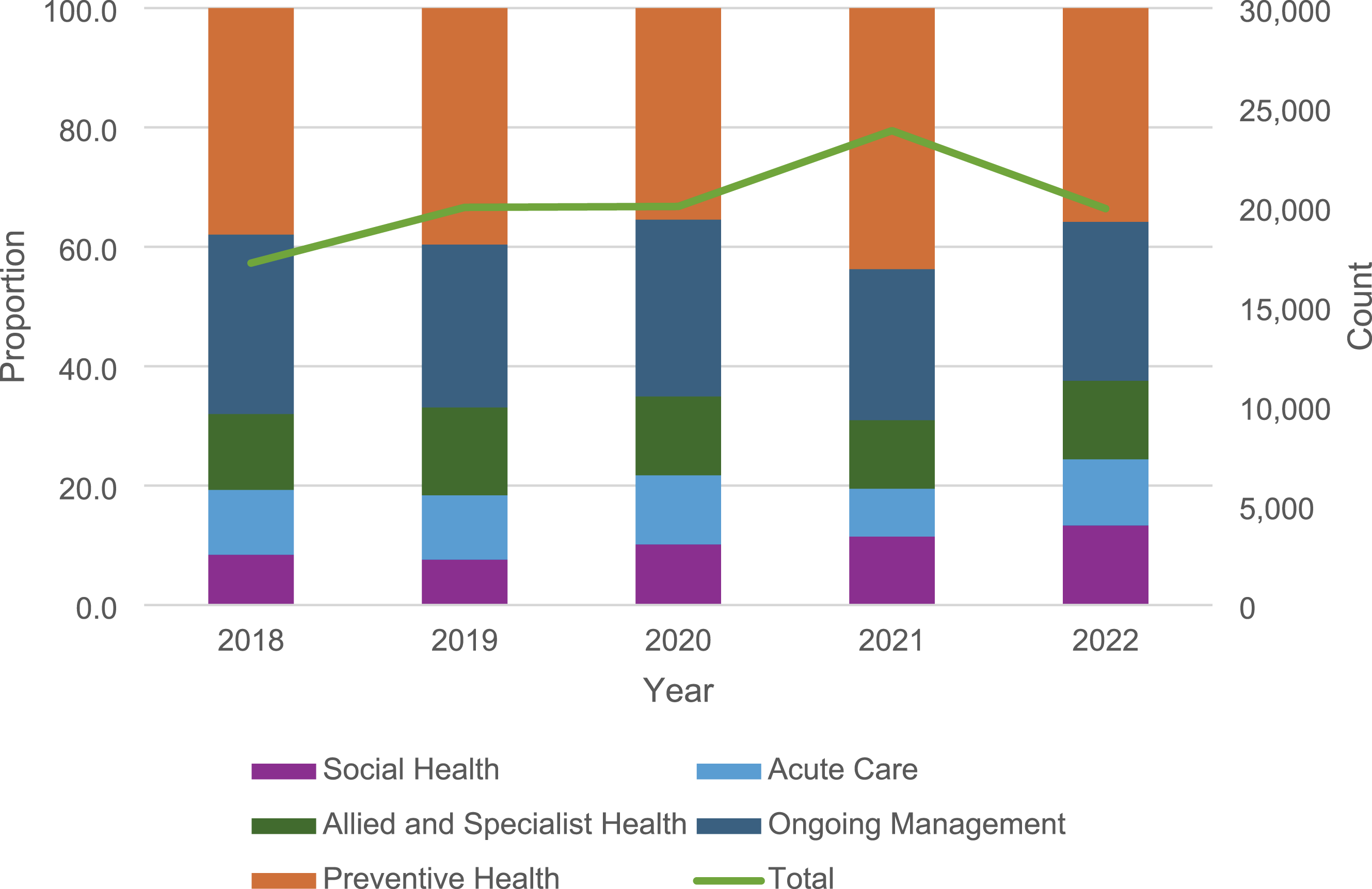
Reasons for Encounters by Gender and Age
Girls/women were three times as likely to have had an encounter related to ongoing management, twice as likely for social health and acute care, and one-and-a-half times more likely to have had preventive health-related reasons for an encounter than boys/men (Figure 4). Over time, all reasons for encounters increased across all genders, except for ongoing management among girls/women, which increased annually until 2021 but decreased in 2022 to below the number of encounters in 2018. PHC encounters by Aboriginal and Torres Strait Islander young people aged 15 to 24 years, by reasons for encounter and gender, 2018-2022. N.B. Excludes gender Not Stated as count <10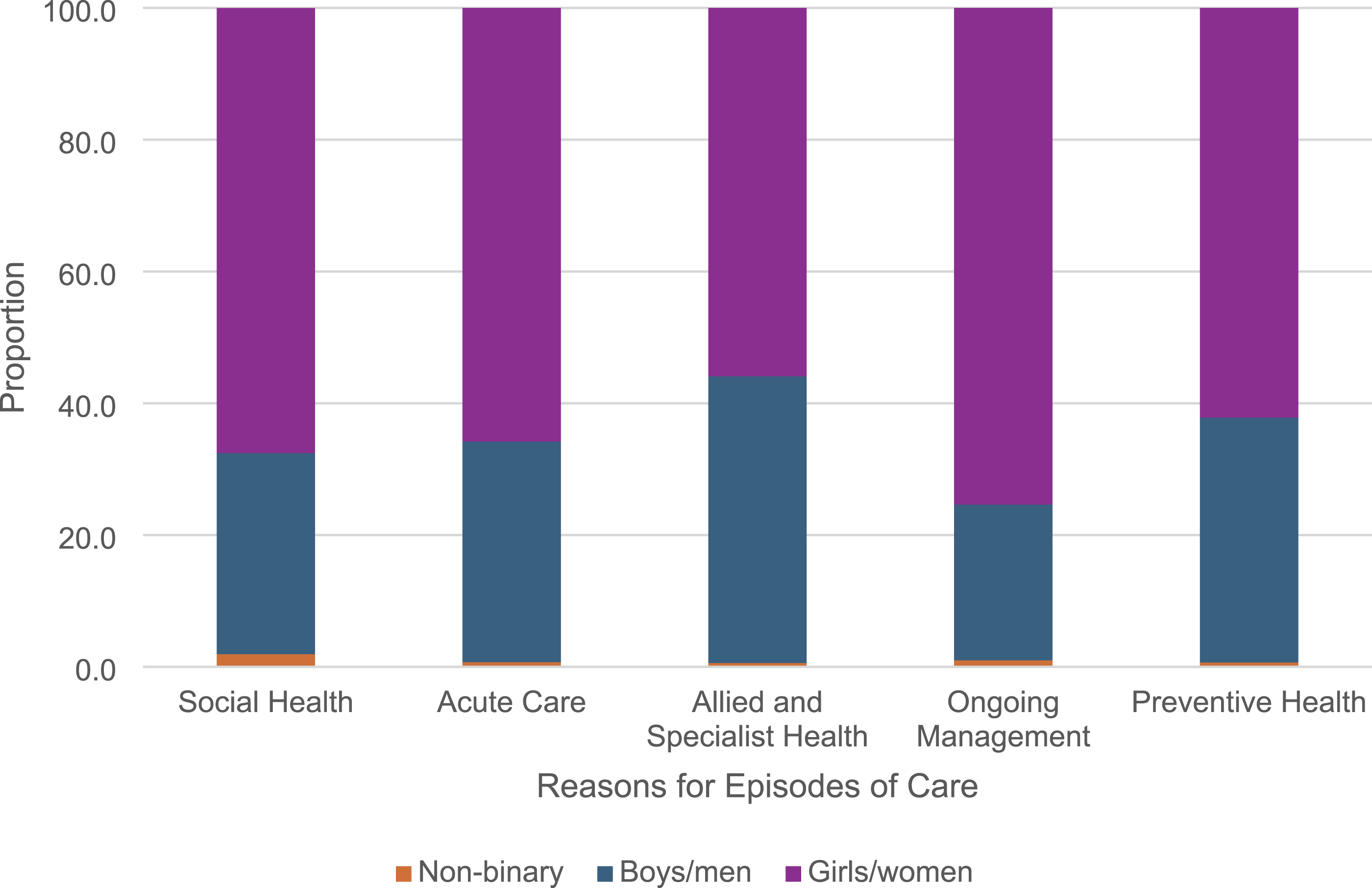
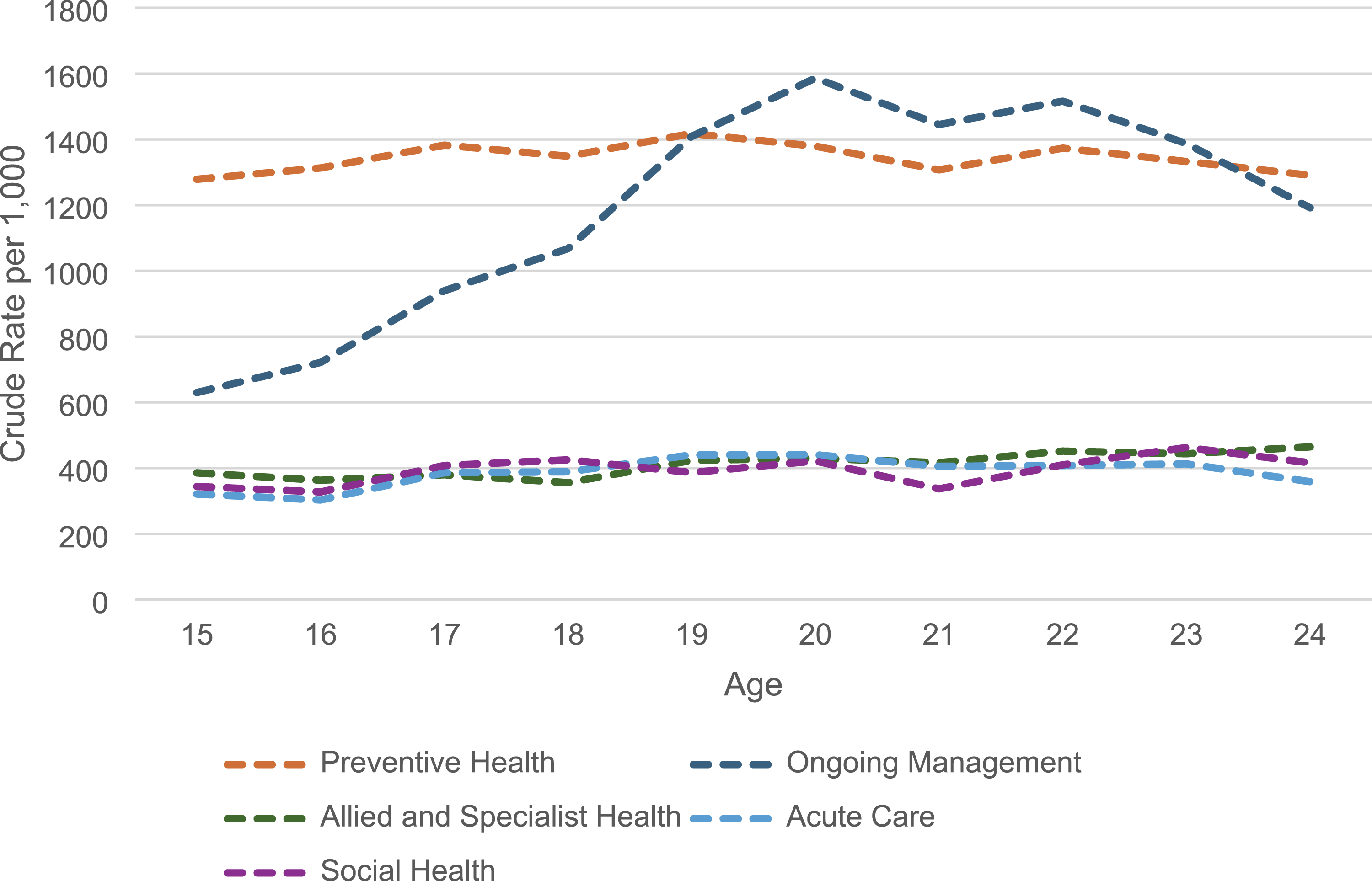
By age, and age and gender, crude rates, for most reasons, were constant as age increased, except for ongoing management, which increased by age, and age and girls/women (Figures 5 and 6, and Figure 7), although the number of encounters for all reasons decreased as age increased except for ongoing management, which increased with age and age and girls/women. Preventive health was the primary reason for encounters across all age groups and genders, except among girls/women aged 20-23 years. Similarly, the number of reasons for encounters decreased with age across all genders. However, the only exceptions were social health, allied and specialist health, and ongoing management, which increased with age for girls/women. Among boys/men, the number of reasons for preventive health declined from ages 15 to 20. PHC encounters by Aboriginal and Torres Strait Islander young people aged 15 to 24 years, by age and reasons for encounter, 2018-2022 PHC encounters by Aboriginal and Torres Strait Islander girls/women aged 15 to 24 years, by age and reasons for encounter 2018-2022 PHC encounters by Aboriginal and Torres Strait Islander boys/men aged 15 to 24 years, by age and reasons for encounter, 2018-2022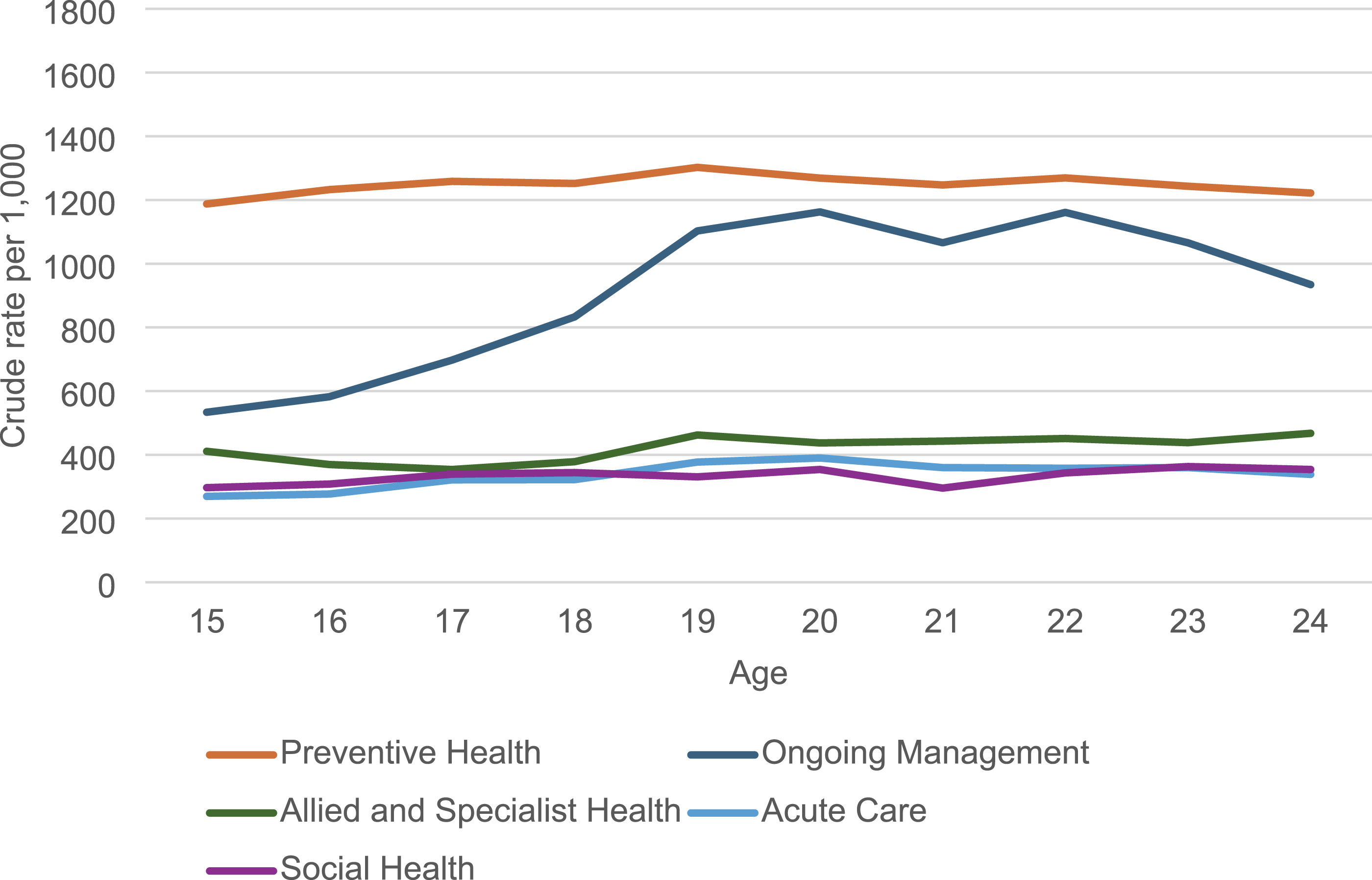

Over time, encounters increased for most reasons among girls/women and boys/men of all ages, and for non-binary individuals across most ages; however, girls/women comprised the largest proportion across all ages for each reason (data not presented). There were notable increases in social health and preventive health-related reasons for encounters for girls/women for most ages and boys/men aged 15-19 years, and for preventive health-related reasons for all ages for girls/women and boys/men, and most ages for non-binary young people in 2021. However, there were decreases over time in the number of encounters related to ongoing management for girls/women aged 16, 17, 18, 19, 20, 21 and 22 years, and boys/men aged 18, 19 and 20 years; preventive health for girls/women aged 18 and 19 years, and boys/men aged 20, 21 and 22 years; allied and specialist health for girls/women aged 16 years and boys/men aged 18 and 19 years; acute care for girls/women aged 15, 18 and 24 years, and boys/men aged 19 and 20 years; and social health for boys/men aged 24 years.
Discussion
This is one of the first studies to examine encounters at ATSICCHO services among Aboriginal and Torres Strait Islander people aged 15-24 years in Australia. The study focused on urban SEQ and analysed patient records for 12,449 individuals, comprising 127,225 encounters, from 2018 to 2022. It was estimated that over one-third of the Aboriginal and Torres Strait Islander population aged 15-24 years who resided in the ATSICCHO catchment area utilised these services during the study period. Girls/women received two-thirds of these encounters, despite boys/men comprising 43% of the study population. Boys/men were less likely to utilise services and did so less frequently than girls/women. This data is consistent with other evidence, which has also identified that young people, especially young boys/men, do not utilise PHC services as frequently. 5
The utilisation of ATSICCHOs among the study population showed a notable increase, with a 27% rise in the number of individuals utilising these services and a 29% increase in the frequency of encounters. This trend is particularly significant in the context of the broader Aboriginal and Torres Strait Islander population in SEQ. This population grew from 70,162 individuals in 2016 to 100,101 in 2021, reflecting a 42.7% increase over the intercensal period.33,35 Notably, despite population growth and increased demand for health care services, annual funding and resource allocation for ATSICCHOs have not increased sufficiently to meet the growing needs of this population.36-38 This discrepancy raises important concerns regarding equity in health care utilisation and the sustainability of service provision for Aboriginal and Torres Strait Islander communities.
Further, the increase in individuals utilising services and encounters during the study period, particularly in 2021, can be partially linked to the COVID-19 pandemic, including the expanded access to COVID-19 vaccines. This increase may reflect a deviation from typical utilisation patterns, and this should be considered when interpreting these results. During the pandemic, the Australian government implemented several initiatives to facilitate pandemic-related care while also maintaining usual care practices. Initiatives included enhancing telehealth, introducing electronic prescribing, and introducing additional MBS items for general practitioners to support in-person and telehealth care for COVID-19-positive patients.39,40 The implementation of these initiatives supported increased utilisation of care during a time of heightened demand. Additionally, similar strategies, such as bulk billing for young people, could be explored as a long-term solution to enhance utilisation of PHC services and to encourage health promotion and prevention for this important age group.
Preventive health and ongoing management were the main reasons for young people, mostly girls/women, utilising ATSICCHOs during the study period. This is likely due to increased maternal and reproductive health care during this period of life.5,41 Similarly, encounters related to social health had the greatest increase. This increase may reflect that mental health disorders often first emerge during adolescence, 42 and that mental health and substance use disorders are the leading contributors to the burden of disease in young people. 43 Encouragingly, preventive health reasons for encounters increased over the five-year period. The ATSICCHOs included in this study are part of the Deadly Choices initiative, which encourages health checks among the Aboriginal and Torres Strait Islander community by incentivising participation with a free Deadly Choices shirt. 44 The uptake of health checks and COVID-19 vaccines is a testament to the work of ATSICCHOs, their strong history of culturally appropriate health promotion, 45 and being a part of their communities allows them to understand the community’s needs.
While utilisation of PHC services is important, the frequency with which an individual uses them is equally important. The study found that over the five-year period, the median number of encounters was three. Only 6% of young people utilised an ATSICCHO annually, while 47% utilised a service one year during the five-year period. These data indicate insufficient opportunities to utilise health care. The National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people, 46 recommends that Aboriginal and Torres Strait Islander young people receive annual or opportunistic screening or assessment for age or condition-specific health and wellbeing factors. These factors include lifestyle, sexual health and blood-borne viruses, pregnancy and antenatal care, diabetes, cardiovascular disease, and oral health. This study highlights discrepancies between policy, practice, and health promotion initiatives.
In addition, the decline in utilisation of ATSICCHOs among young people with increasing age is noteworthy. The decrease may be related to the fact that, as young people age, their independence increases, reducing their likelihood of utilising health services independently and proactively. However, we know that the burden of disease increases with age among Aboriginal and Torres Strait Islander young people. 43 It is more plausible that older young people find it difficult to utilise PHC services when needed due to work, study, or other commitments. Discrete efforts to engage with and increase utilisation for older young people are required to address this gap.
One limitation of the study was its focus on SEQ; our findings may not necessarily be transferable to all ATSICCHOs or PHC services in Queensland or Australia. Nevertheless, it emphasises the increasing health needs of Aboriginal and Torres Strait Islander young people, particularly in areas related to preventive health and ongoing management. EMR data were used in this study, and there are limitations inherent to these data, including issues related to quality, accuracy, and completeness. 47 Overall, the data quality for this study was acceptable; however, there were some challenges, such as variable completeness. For example, the reason for contact data was used to create reasons for encounter. Reasons for encounter were captured in 79.3% of all encounters; pathology and other investigations accounted for 7.9%. While these are essential components of PHC, most of this data was non-descriptive and not attributable to specific aspects of health and wellbeing or health care. A further 21.9% of observations had missing reasons for contact. This suggests that how EMR data are recorded, captured, and extracted from EMRs is important; improving EMR practices, systems, extraction methods, and training for health professionals could address issues related to data quality and reliability, particularly when data are used for quality improvement processes or research purposes. Despite this, the incompleteness and quality of EMR data may introduce selection and information biases into the results, as records with incomplete fields/variables may differ systematically from those with complete records, potentially skewing outcomes and limiting the generalisability of results. Service-level differences, such as staffing and EMR practices, may influence encounter patterns. Furthermore, there may have been an interpretation bias; however, this is likely to have been mitigated by the involvement of the Indigenous advisory group and the participating ATSICCHOs in interpreting the results. Additionally, the analysis and interpretation of results were led by an Aboriginal person and overseen by experienced researchers, including a medical doctor.
Conclusion
This study provides one of the first comprehensive examinations of health care encounters among Aboriginal and Torres Strait Islander young people utilising urban ATSICCHOs in SEQ. Despite data limitations, the findings demonstrate increased service utilisation between 2018 and 2022, with preventive health and ongoing management constituting the most common reasons for encounters. However, engagement with services remained largely episodic, with most young people attending infrequently over the five-year period, and marked differences were observed by gender and age. Boys/men and older young people were consistently less likely to utilise services and did so less often, highlighting persistent inequities in continuity of care during a critical life stage characterised by increasing health and wellbeing needs.
While ATSICCHOs play a vital role in delivering culturally safe, holistic, comprehensive PHC, these findings underscore the need to move beyond measures of utilisation alone and towards strategies that strengthen sustained engagement and continuity of care for young people. Purpose-designed, youth-centred models of care, co-designed with Aboriginal and Torres Strait Islander young people and supported by adequate and sustained funding, are essential to address structural barriers to utilisation and optimise opportunities for preventive, early intervention, and ongoing care. Strengthening PHC engagement during adolescence and young adulthood has the potential to improve immediate health outcomes and contribute to longer-term and intergenerational health equity for Aboriginal and Torres Strait Islander communities. Future efforts should prioritise targeted engagement strategies, particularly for boys/men and older young people, strengthen continuity-of-care mechanisms, and further research to inform and evaluate effective youth-centred models of care.
Supplemental Material
Supplemental Material - Supplemental Material for Health Care Encounters by Aboriginal and Torres Strait Islander People Aged 15-24 years at Urban Aboriginal and Torres Strait Islander Community-Controlled Health Organisations in southeast Queensland
Supplemental Material for Health Care Encounters by Aboriginal and Torres Strait Islander People Aged 15-24 years at Urban Aboriginal and Torres Strait Islander Community-Controlled Health Organisations in southeast Queensland by Stephen Harfield, Peter Azzopardi, Gita D Mishra and James Ward in Journal of Primary Care & Community Health.
Footnotes
Acknowledgements
The authors wish to acknowledge the traditional custodians of the Brisbane area, the Country on which this research was conducted, the Turrbal and Jagera people, and pay respects to their ancestors and descendants. We also acknowledge the Aboriginal and Torres Strait Islander community-controlled health services that participated in the study and for sharing their communities’ data.
Ethical Considerartions
Ethics approval was granted by the Human Research Ethics Committees at The University of Queensland (2022/HE001155).
Consent to Participate
Approval for the study was obtained from participating ATSICCHOs and their respective research sub-committee. Approval of the results and final output was sought and provided by the participating ATSICCHOs.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SH was supported by Australian Government Research Training Program Scholarship, an Aboriginal and Torres Strait Islander Research Training Program, UQ Poche Centre for Indigenous Health Research Top-Up Scholarships, a Lowitja Institute Higher Degree Research Top-Up Scholarship, and a Top-Up Scholarship from the Australian Longitudinal Study on Women’s Health, funded by the Australian Government Department of Health and Aged Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Sharing Statement
The de-identified data we analysed for this study will not be shared, as we do not have permission from the participating services or ethics approval to do so.
Positionality Statement
The study was led by SH, a Narungga and Ngarrindjeri man from South Australia, who is a public health researcher and Senior Research Fellow. He has over 10 years of research experience with Aboriginal and Torres Strait Islander communities. JW, a Pitjantjatjara and Narungga man, is an infectious diseases epidemiologist and Director of the UQ Poche Centre, with over 25 years in Indigenous health research. PA is a non-Indigenous adolescent health researcher and head of Adolescent Health and Wellbeing at the Kids Research Institute, working in partnership with Aboriginal and Torres Strait Islander communities across Australia. GM is a non-Indigenous professor in life course epidemiology and women’s health at the University of Queensland, who leads health research initiatives focused on women and non-communicable diseases.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.