
Abstract
During the 4-year time interval of 2005 through 2008, the Society of Thoracic Surgeons Congenital Heart Surgery Database documented data about 2882 operations to repair atrioventricular (AV) canal defects: partial, 623 (21.5%); intermediate, 342 (11.8%);. complete, 1917 (66.3%). Mean age at complete repair (years) was as follows: partial, 6.1; intermediate, 2.9; complete, 0.6. Median age at complete repair (years) was as follows: partial, 2.6; intermediate, 0.9; complete, 0.4. Down syndrome was present in 1767 patients (61.1%). Debanding of the pulmonary artery was rarely performed: partial, 1 (0.2%); intermediate, 0 (0.0%); complete, 66 (3.4%). Deep hypothermic circulatory arrest was rarely used: partial, 6 (1.0%); intermediate, 5 (1.5%); complete, 52 (2.7%). Discharge mortality was low: partial, 2 (0.3%); intermediate, 3 (0.9%); complete, 38 (2.0%). Atrioventricular block requiring permanent pacemaker occurred but was uncommon: partial, 6 (1.0%); intermediate, 2 (0.6%); complete, 29 (1.5%). Unplanned reoperation prior to hospital discharge occurred in 3.9% of complete AV canal repairs. The sternum was left open in 3.0% of complete AV canal repairs. Postoperative cardiac arrest occurred in 1.9% of complete AV canal repairs. Mean postoperative length of stay (days) was as follows: partial, 5.2; intermediate, 7; complete, 13.1. Median postoperative length of stay (days) was as follows: partial, 4; intermediate, 4; complete, 7. This review of data from the Society of Thoracic Surgeons Congenital Heart Surgery Database allows for unique documentation of patterns of practice and outcomes. From this review, we learned that 98% to 99% of patients survive complete repair of AV canal and 96% to 97% survive complete repair of AV canal with no major complications.
Keywords
The Congenital Heart Surgery Database of the Society of Thoracic Surgeons (STS) is the largest database in North America that tracks the outcomes of pediatric and congenital heart surgery. 1 The terms atrioventricular septal defect, atrioventricular canal defect, and endocardial cushion defect are synonyms. 2,3 The essence of this cardiac malformation is an atrioventricular septal defect in the setting of a common atrioventricular junction. 4,5 These defects are characterized by varying degrees of incomplete development of the septal tissue surrounding the atrioventricular valves along with varying degrees of abnormalities of the atrioventricular valves themselves. Consequently, atrioventricular septal defect may include defects in the inferior and posterior portion of the atrial septum (ostium primum atrial septal defect), defects in the inflow portion of the ventricular septum (inlet ventricular septal defect), and defects in the tissue forming the left and right atrioventricular valves (“cleft” of the left atrioventricular valve).
The purpose of this article is to review the data about atrioventricular canal defects in the STS Congenital Heart Surgery Database. This article first reviews the system of nomenclature and classification used in the STS Congenital Heart Surgery Database for atrioventricular canal defects and then presents the data contained in the STS Congenital Heart Surgery Database about atrioventricular canal defects.
Methods
Nomenclature
In April 2000, the proceedings of the International Congenital Heart Surgery Nomenclature and Database Project of the STS and the European Association for Cardio-Thoracic Surgery (EACTS) were published as a supplement to the Annals of Thoracic Surgery. 2 An article in this supplement was devoted to atrioventricular canal defect, 3 and in this article, a comprehensive system of nomenclature and classification was presented for atrioventricular canal defect, along with associated definitions. The topic had been the subject of extensive debates and review during the meetings of members of the STS and the EACTS, which took place from 1998 through 2000 as part of the International Congenital Heart Surgery Nomenclature and Database Project. 2,3 Efforts were made to include all relevant categories of nomenclature, using synonyms where appropriate.
The topic of nomenclature and classification was further debated at the first meeting of the International Working Group for Mapping and Coding of Nomenclatures for Paediatric and Congenital Heart Disease, also known as the Nomenclature Working Group (NWG), 6-11 which was held in Montreal, Canada, May 9 to 13, 2002. The NWG is one of three committees of the International Society for Nomenclature of Paediatric and Congenital Heart Disease (ISNPCHD). The ISNPCHD was constituted in January of 2005.
The NWG created and maintains the International Paediatric and Congenital Cardiac Code (IPCCC). The IPCCC was created by reviewing 28 major categories of cardiac lesions and cross-mapping several existing systems for nomenclature, including the nomenclature of the International Congenital Heart Surgery Nomenclature and Database Project of the STS and EACTS and the nomenclature of European Paediatric Cardiac Code (EPCC) of the Association for European Paediatric Cardiology (AEPC). 6-11 This IPCCC was proposed at the First International Summit on Nomenclature for Congenital Heart Disease at the Third World Congress of Pediatric Cardiology and Cardiac Surgery, Toronto, Canada, May 27, 2001. The IPCCC was unveiled officially at the Second International Summit on Nomenclature for Pediatric and Congenital Heart Disease at the Fourth World Congress of Pediatric Cardiology and Cardiac Surgery, Buenos Aires, Argentina, September 19, 2005. A more mature and evolved version of the IPCCC was then presented at the Third International Summit on Nomenclature for Pediatric and Congenital Heart Disease at the Fifth World Congress of Pediatric Cardiology and Cardiac Surgery, Convention Center, Cairns, Queensland, Australia, June 21, 2009. The IPCCC is available for download from the Internet, free of charge, at www.ipccc.net.
The IPCCC has 2 widely used versions: The version of the IPCCC derived from the nomenclature of the International Congenital Heart Surgery Nomenclature and Database Project of the EACTS and STS The version of the IPCCC derived from the nomenclature of the European Paediatric Cardiac Code of the AEPC
Both of these systems were developed with considerable input from both cardiologists and surgeons.
In the STS Congenital Heart Surgery Database and the EACTS Congenital Heart Surgery Database, the system of nomenclature used is the version of the IPCCC derived from the nomenclature of the International Congenital Heart Surgery Nomenclature and Database Project of the EACTS and STS. In the next section of this article, we present the definitions used for the nomenclature in the STS Congenital Heart Surgery Database and the EACTS Congenital Heart Surgery Database.
Definitions Related to Atrioventricular Septal Defect
As stated above, the essence of the malformation remains an atrioventricular septal defect in the setting of a common atrioventricular junction.
4,5
Atrioventricular septal defect represents a spectrum of cardiac anomalies subdivided into 3 subtypes
12
: Partial atrioventricular septal defect Transitional atrioventricular septal defect Complete atrioventricular septal defect
Partial atrioventricular septal defect (also known as incomplete atrioventricular septal defect as well as partial atrioventricular canal defect and incomplete atrioventricular canal defect) has a crescent-shaped atrial septal defect in the inferior portion of the atrial septum just above the atrioventricular valves (an ostium primum atrial septal defect) and may have varying degrees of malformation of the left atrioventricular valve leading to varying degrees of left atrioventricular valve regurgitation.
Complete atrioventricular septal defect (also known as complete atrioventricular canal defect) has both a defect in the atrial septum just above the atrioventricular valve (ostium primum atrial septal defect) and a defect in the ventricular septum just below the atrioventricular valve (inlet ventricular septal defect). In hearts with complete atrioventricular septal defect, the atrioventricular valve is one valve that bridges both the right and left sides of the heart, creating superior (anterior) and inferior (posterior) bridging leaflets.
Transitional atrioventricular septal defect (also known as intermediate atrioventricular septal defect as well as transitional atrioventricular canal defect and intermediate atrioventricular canal defect) is in the middle of this spectrum and has 2 distinct left and right atrioventricular valve orifices but also has both an atrial septal defect just above and a ventricular septal defect just below the atrioventricular valves. Although these atrioventricular valves in the intermediate form comprise 2 separate orifices, they remain abnormal valves. The ventricular septal defect in this lesion is often restrictive.
The Rastelli classification, originally described in 1966, 13 describes 3 types of complete atrioventricular septal defect based on the morphology of the superior (anterior) bridging leaflet, its degree of bridging, and its chordal attachments. The Rastelli classification does not relate to the anatomy of the inferior (posterior) bridging leaflet because this leaflet displays greater anatomic variation, and no consistent relationship exists between the morphology of the superior (anterior) bridging leaflet and that of the inferior (posterior) bridging leaflet. In a Rastelli type A defect, the common superior (anterior) bridging leaflet is effectively split in two at the septum: the left superior (anterior) leaflet is entirely over the left ventricle, and the right superior (anterior) leaflet is similarly entirely over the right ventricle. The division of the common superior (anterior) bridging leaflet into left and right components is caused by extensive attachment of the superior (anterior) bridging leaflet to the crest of the ventricular septum by chordae tendineae. In many cases, this chordal attachment pulls the plane of the atrioventricular valve down into the ventricular septal defect below the plane of the annulus. Rastelli type B is rare and involves anomalous papillary muscle attachment from the right side of the ventricular septum to the left side of the common superior (anterior) bridging leaflet. In Rastelli type C defects, there is marked bridging of the ventricular septum by the superior (anterior) bridging leaflet. The superior (anterior) bridging leaflet is generally not divided and floats freely over the ventricular septum without chordal attachment to the crest of the ventricular septum.
In the official Short List of the STS Congenital Heart Surgery Database 14 and the EACTS Congenital Heart Surgery Database, the following abbreviations are used: AVC, atrioventricular canal; AVSD, atrioventricular septal defect; CAVSD, complete atrioventricular septal defect; PAVSD, partial atrioventricular septal defect; ASD, atrial septal defect; TOF, tetralogy of Fallot; AV, atrioventricular.
The following diagnostic terms are contained within the Diagnosis Short List of the STS Congenital Heart Surgery Database and the EACTS Congenital Heart Surgery Database: AVC (AVSD), Complete (CAVSD) AVC (AVSD), Intermediate (transitional) AVC (AVSD), Partial (incomplete) (PAVSD) (ASD, primum) TOF, AVC (AVSD) Single ventricle, Unbalanced AV canal AVC (AVSD) repair, Complete (CAVSD) AVC (AVSD) repair, Intermediate (transitional) AVC (AVSD) repair, Partial (incomplete) (PAVSD) TOF-AVC (AVSD) repair
The following procedural terms are contained within the Procedure Short List of the STS Congenital Heart Surgery Database and the EACTS Congenital Heart Surgery Database:
The following definitions are used by the STS Congenital Heart Surgery Database and the EACTS Congenital Heart Surgery Database and are published in the STS Congenital Heart Surgery Database Data Specifications version 3.0, which became the active version of definitions for these databases on January 1, 2010
15
:
AVC (AVSD), Complete (CAVSD)
“Indicate if the patient has the diagnosis of ‘AVC (AVSD), Complete (CAVSD).’ An ‘AVC (AVSD), Complete (CAVSD)’ is a ‘complete atrioventricular canal’ or a ‘complete atrioventricular septal defect’ and occurs in a heart with the phenotypic feature of a common atrioventricular junction. An ‘AVC (AVSD), Complete (CAVSD)’ is defined as an AVC with a common AV valve and both a defect in the atrial septum just above the AV valve (ostium primum ASD [a usually crescent-shaped ASD in the inferior (posterior) portion of the atrial septum just above the AV valve]) and a defect in the ventricular septum just below the AV valve (inlet VSD). The AV valve is one valve that bridges both the right and left sides of the heart. Balanced AVC is an AVC with two essentially appropriately sized ventricles. Unbalanced AVC is an AVC defect with two ventricles in which one ventricle is inappropriately small. Such a patient may be thought to be a candidate for biventricular repair or, alternatively, may be managed as having a functionally univentricular heart. AVC lesions with unbalanced ventricles so severe as to preclude biventricular repair should be classified as single ventricles. Rastelli type A: The common superior (anterior) bridging leaflet is effectively split in two at the septum. The left superior (anterior) leaflet is entirely over the left ventricle and the right superior (anterior) leaflet is similarly entirely over the right ventricle. The division of the common superior (anterior) bridging leaflet into left and right components is caused by extensive attachment of the superior (anterior) bridging leaflet to the crest of the ventricular septum by chordae tendineae. Rastelli type B: Rare, involves anomalous papillary muscle attachment from the right side of the ventricular septum to the left side of the common superior (anterior) bridging leaflet. Rastelli type C: Marked bridging of the ventricular septum by the superior (anterior) bridging leaflet, which floats freely (often termed a ‘free-floater’) over the ventricular septum without chordal attachment to the crest of the ventricular septum.”
AVC (AVSD), Intermediate (transitional)
“An AVC with 2 distinct left and right AV valve orifices but also with both an ASD just above and a VSD just below the AV valves. While these AV valves in the intermediate form do form 2 separate orifices they remain abnormal valves. The VSD is often restrictive.”
AVC (AVSD), Partial (incomplete) (PAVSD) (ASD, primum)
“An AVC with an ostium primum ASD (a usually crescent-shaped ASD in the inferior (posterior) portion of the atrial septum just above the AV valve) and varying degrees of malformation of the left AV valve leading to varying degrees of left AV valve regurgitation. No VSD is present.”
TOF, AVC (AVSD)
“TOF with complete common atrioventricular canal defect is a rare variant of common atrioventricular canal defect with the associated conotruncal abnormality of TOF. The anatomy of the endocardial cushion defect is that of Rastelli type C in almost all cases.”
Single ventricle, Unbalanced AV canal
“Single ventricle anomalies with a common atrioventricular (AV) valve and only one completely well developed ventricle. If the common AV valve opens predominantly into the morphologic left ventricle, the defect is termed a left ventricular (LV)–type or LV-dominant AV septal defect. If the common AV valve opens predominantly into the morphologic right ventricle, the defect is termed a right ventricular (RV)–type or RV-dominant AV septal defect.”
AVC (AVSD) repair, Complete (CAVSD)
“Repair of complete AV canal (AVSD) using 1 or 2 patch or other technique, with or without mitral valve cleft repair.”
AVC (AVSD) repair, Intermediate (transitional)
“Repair of intermediate AV canal (AVSD) using ASD and VSD patch, or ASD patch and VSD suture, or other technique, with or without mitral valve cleft repair.”
AVC (AVSD) repair, Partial (incomplete) (PAVSD)
“Repair of partial AV canal defect (primum ASD), any technique, with or without repair of cleft mitral valve.”
TOF-AVC (AVSD) repair
“Tetralogy of Fallot repair (assumes VSD closure and relief of pulmonary stenosis at one or more levels), with repair of associated AV canal defect. Repair of associated atrial septal defect or atrioventricular valve repair(s) should be listed as additional or secondary procedures under the primary TOF-AVC procedure.”
STS Congenital Heart Surgery Database
The STS Congenital Heart Surgery Database is the largest database in North America dealing with congenital cardiac malformations. It has grown annually since its inception, in terms of both the number of participating centers submitting data and the number of operations analyzed (Figures 1-3). The STS Congenital Heart Surgery Database currently has 85 participating centers: 83 from the United States, 1 from Canada, and 1 from Japan. The report of the 2005 STS Congenital Heart Surgery Practice and Manpower Survey, undertaken by the STS Workforce on Congenital Heart Surgery, documented that 122 centers in the United States of America perform pediatric and congenital heart surgery. 16 In Canada, 8 centers perform pediatric and congenital heart surgery.
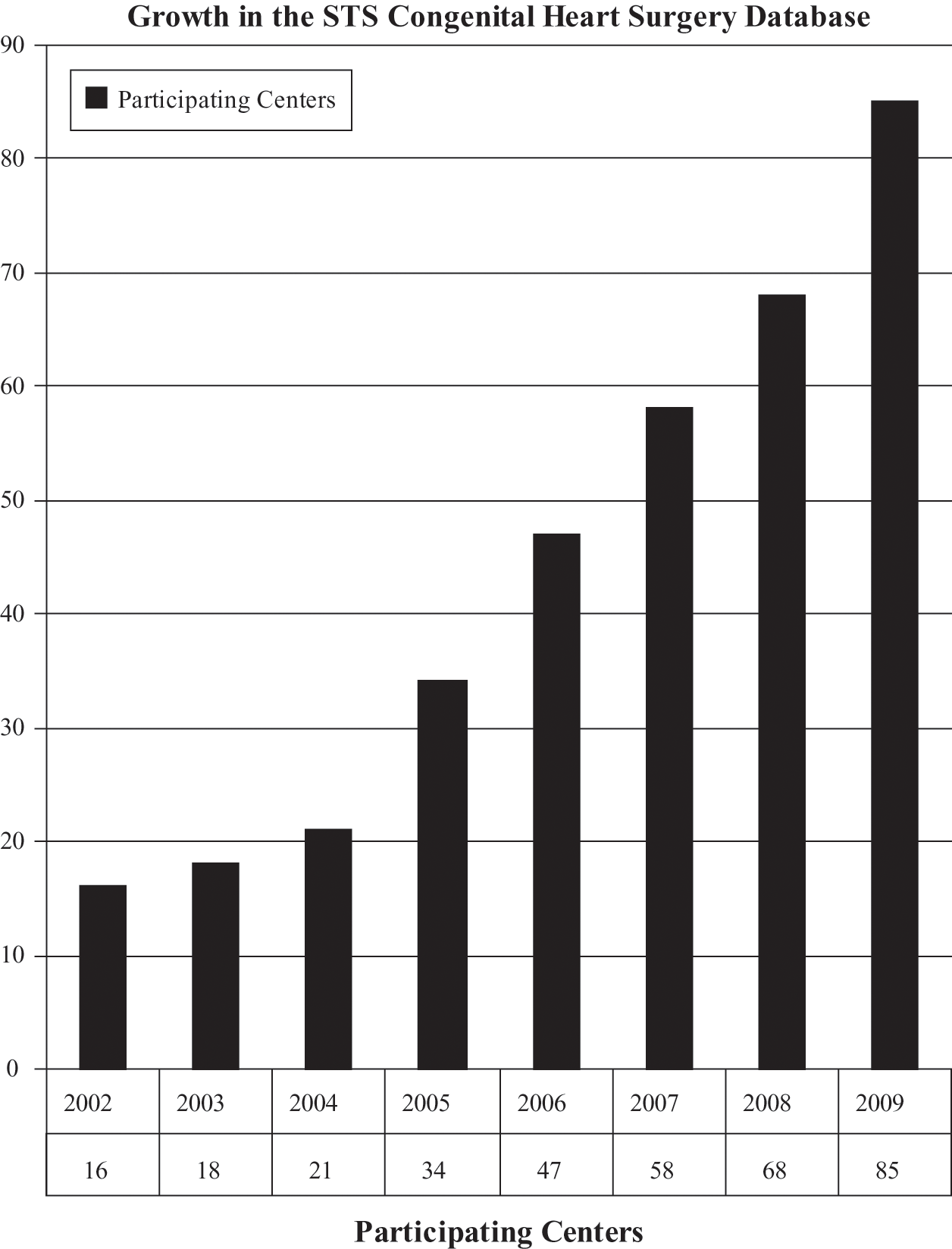
Annual growth in the Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database by number of participating centers. The STS Congenital Heart Surgery Database currently has 85 participating centers: 83 from the United States, 1 from Canada, and 1 from Japan.
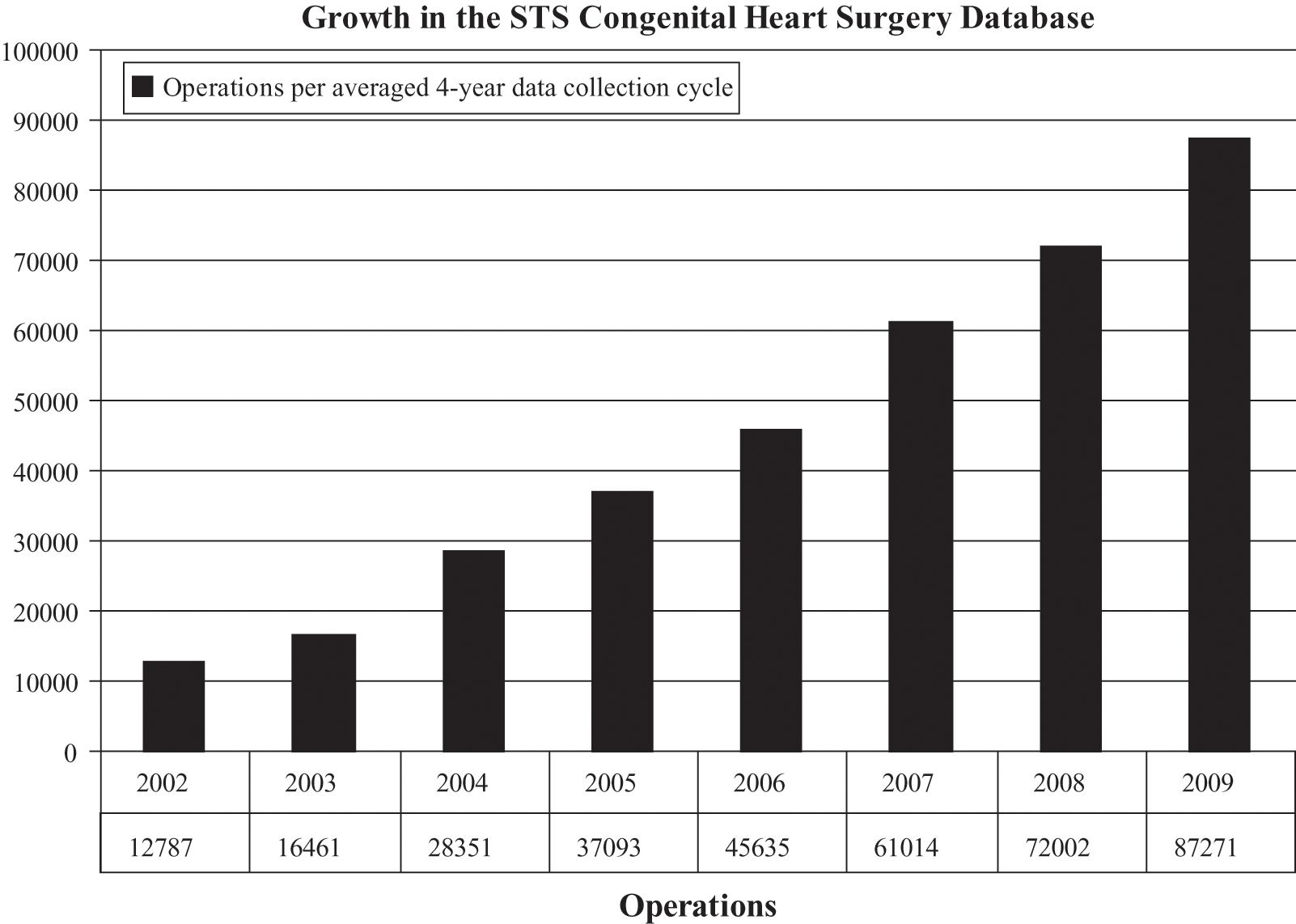
Annual growth in the Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database by the number of operations per averaged 4-year data collection cycle. The aggregate report from the spring 2009 harvest of the STS Congenital Heart Surgery Database included 87 271 operations performed in the 4-year period of January 1, 2005, through December 31, 2008, submitted from 76 centers from North America: 75 from the United States and 1 from Canada. One Japanese center also submits data; however, these Japanese data are not included in the aggregate report produced by the STS.
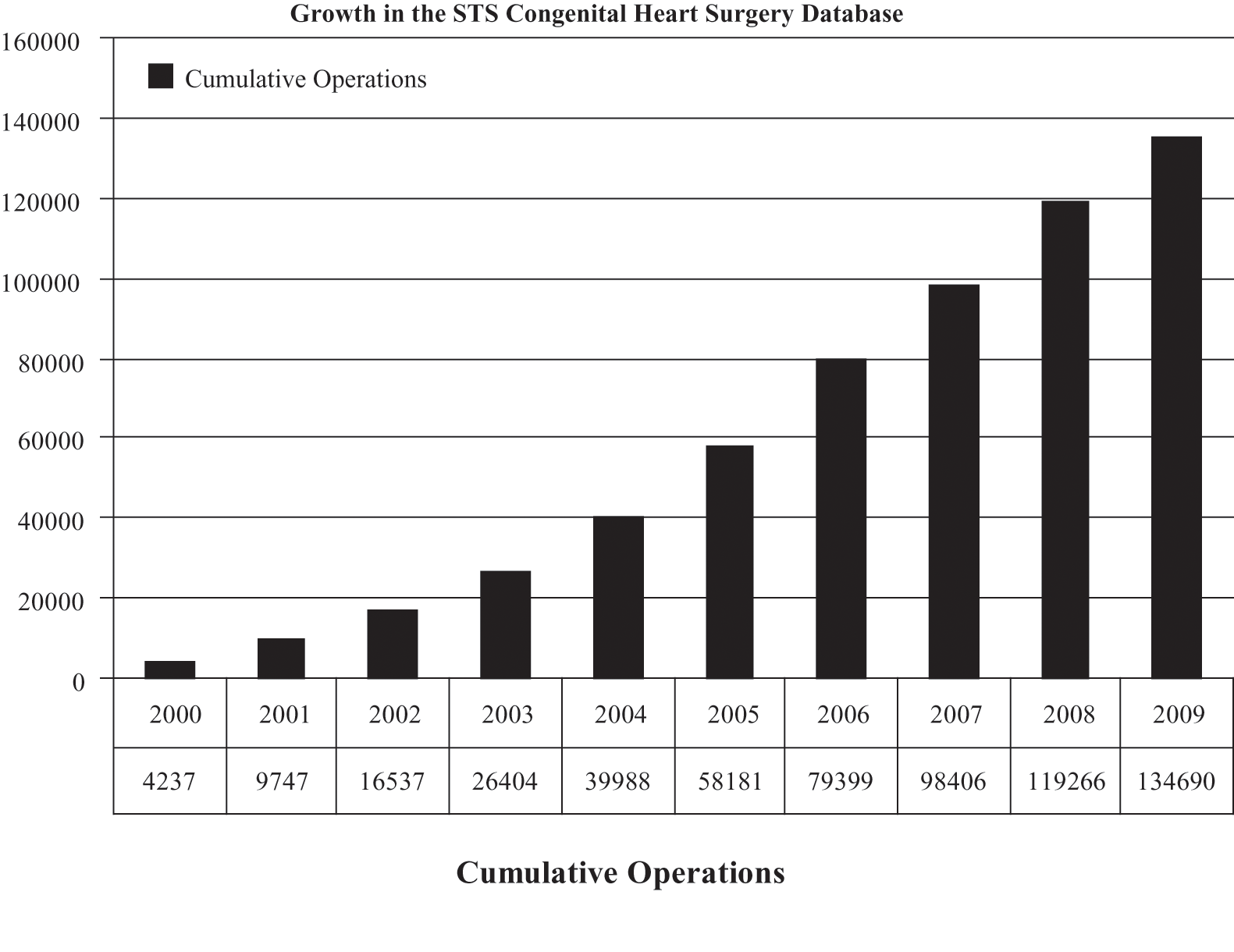
Annual growth in the Society of Thoracic Surgeons (STS) Congenital Heart Surgery Database by the cumulative number of operations over time. The current number of cumulative total operations in the STS Congenital Heart Surgery Database is 134 690. The aggregate report from the spring 2009 harvest of the STS Congenital Heart Surgery Database included 87 271 operations performed in the 4-year period of January 1, 2005, through December 31, 2008, submitted from 76 centers from North America: 75 from the United States and 1 from Canada. One Japanese center also submits data; however, these Japanese data are not included in the aggregate report produced by the STS.
The data in this article are derived from the Spring 2009 STS Congenital Heart Surgery Database Report, 17 which includes 87,271 operations performed during the time interval of January 1, 2005, to December 31, 2008, inclusive, at 76 centers in North America: 75 from the United States and 1 from Canada. One Japanese center also submitted data to this spring 2009 report; however, these Japanese data are not included in the aggregate report produced by the STS.
Results
Data From the STS Congenital Heart Surgery Database
Tables 1 through 8 document demographic, preoperative, intraoperative, and postoperative data about surgery for AV canal from the STS Congenital Heart Surgery Database during the time interval of January 1, 2005, through December 31, 2008, inclusive. Data are presented as percentages, mean values, median values, and interquartile ranges (Q1, Q3) where appropriate.
Diagnostic Incidence of Atrioventricular Canal in the STS Congenital Heart Surgery Database
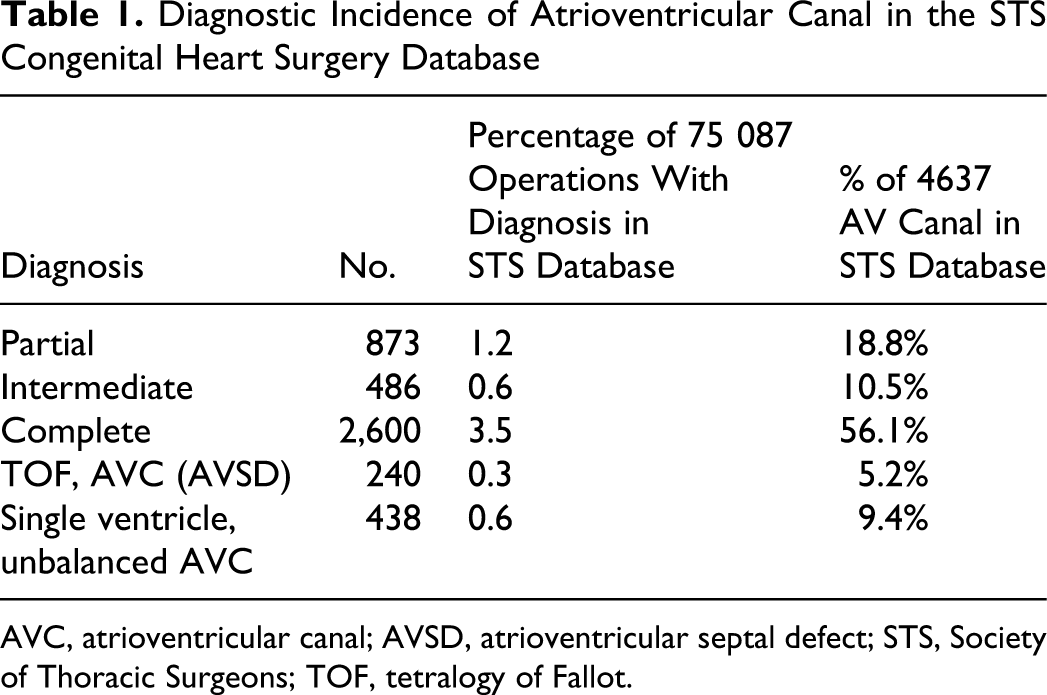
AVC, atrioventricular canal; AVSD, atrioventricular septal defect; STS, Society of Thoracic Surgeons; TOF, tetralogy of Fallot.
Incidence of Complete Repair of 2882 Atrioventricular Canal in the STS Congenital Heart Surgery Database
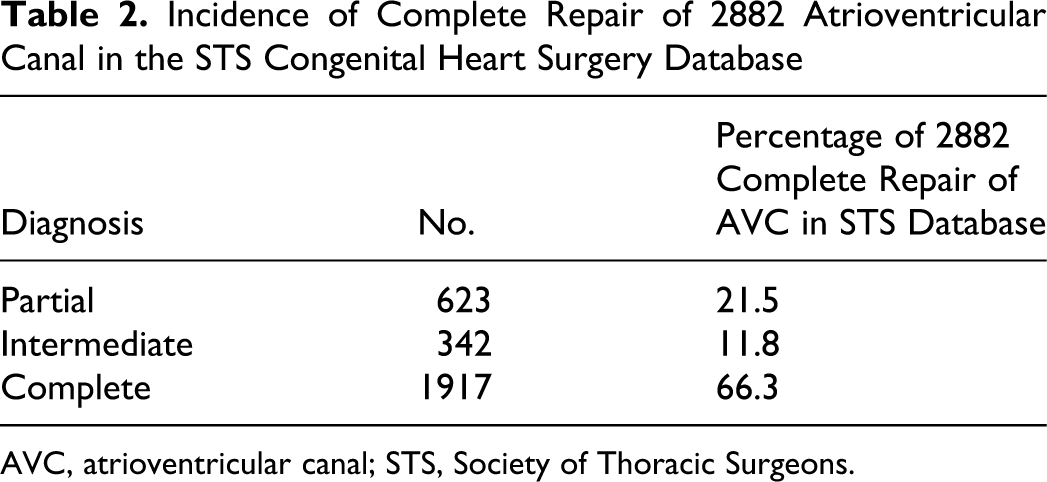
AVC, atrioventricular canal; STS, Society of Thoracic Surgeons.
Age at Complete Repair in Years of 2882 Atrioventricular Canal Operations in the STS Congenital Heart Surgery Database
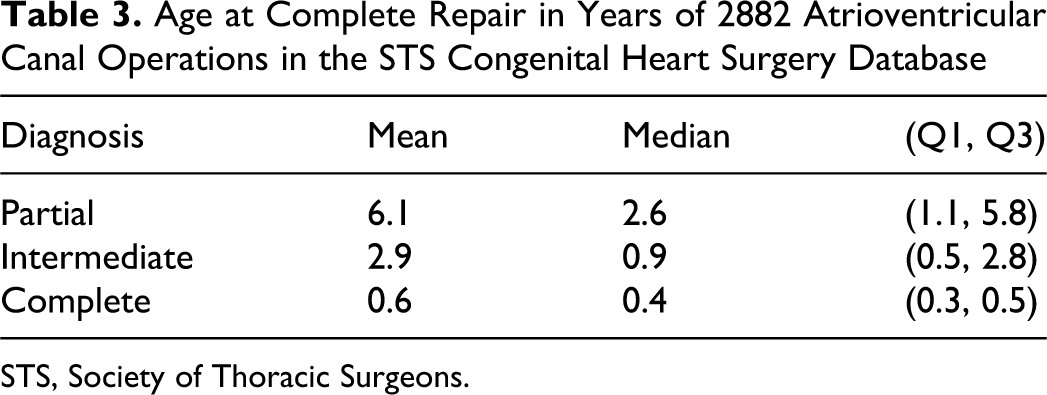
STS, Society of Thoracic Surgeons.
Preoperative Factors and Noncardiac Abnormalities in 2882 Atrioventricular Canal Operations in the STS Congenital Heart Surgery Database
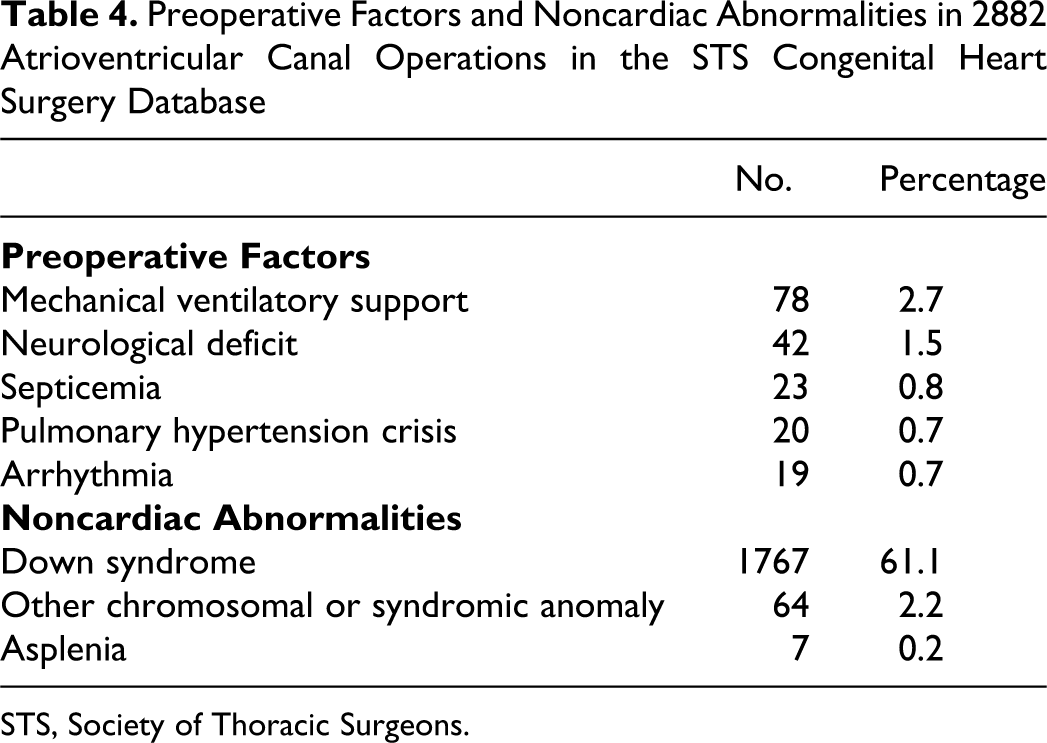
STS, Society of Thoracic Surgeons.
Cardiopulmonary Bypass Time and Aortic Cross-Clamp Time in 2882 Atrioventricular Canal Operations in the STS Congenital Heart Surgery Database
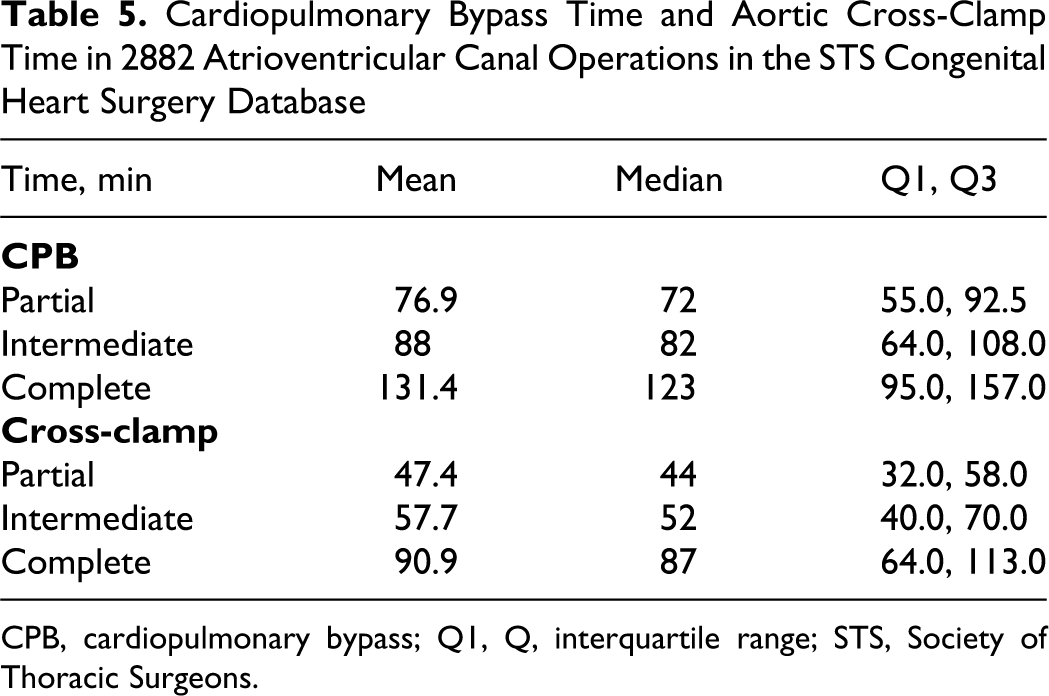
CPB, cardiopulmonary bypass; Q1, Q, interquartile range; STS, Society of Thoracic Surgeons.
Operative Features Including Incidence of Pulmonary Artery (PA) Debanding and Use of Deep Hypothermic Circulatory Arrest (DHAC) in 2882 Atrioventricular Canal Operations in the STS Congenital Heart Surgery Database
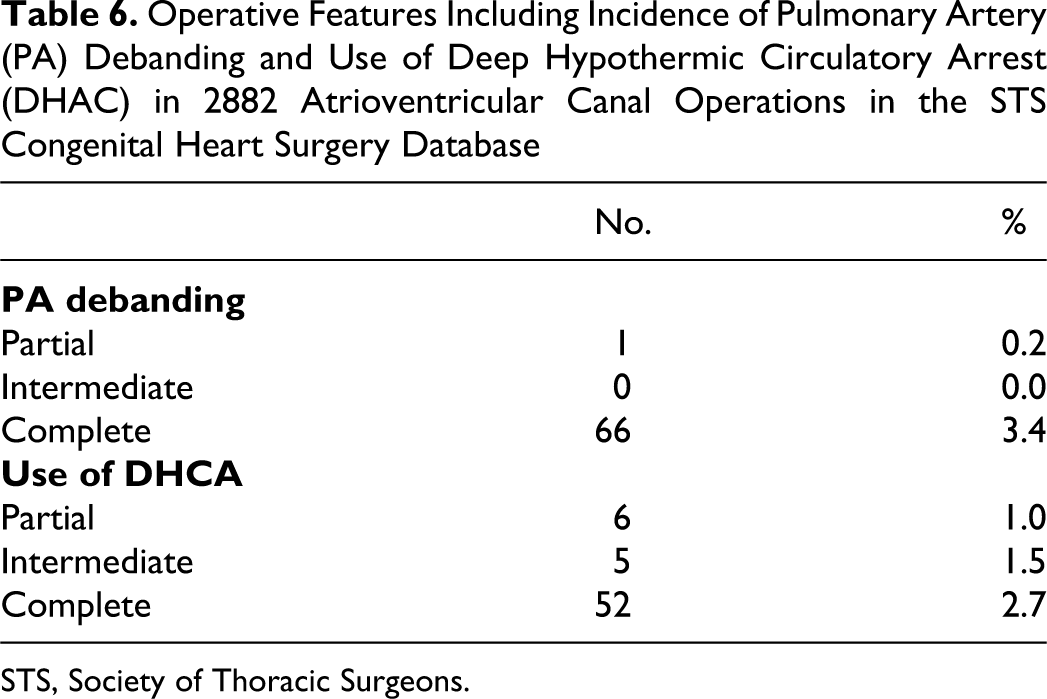
STS, Society of Thoracic Surgeons.
Discharge Mortality and Postoperative Complications in 2882 Atrioventricular Canal Operations in the STS Congenital Heart Surgery Database
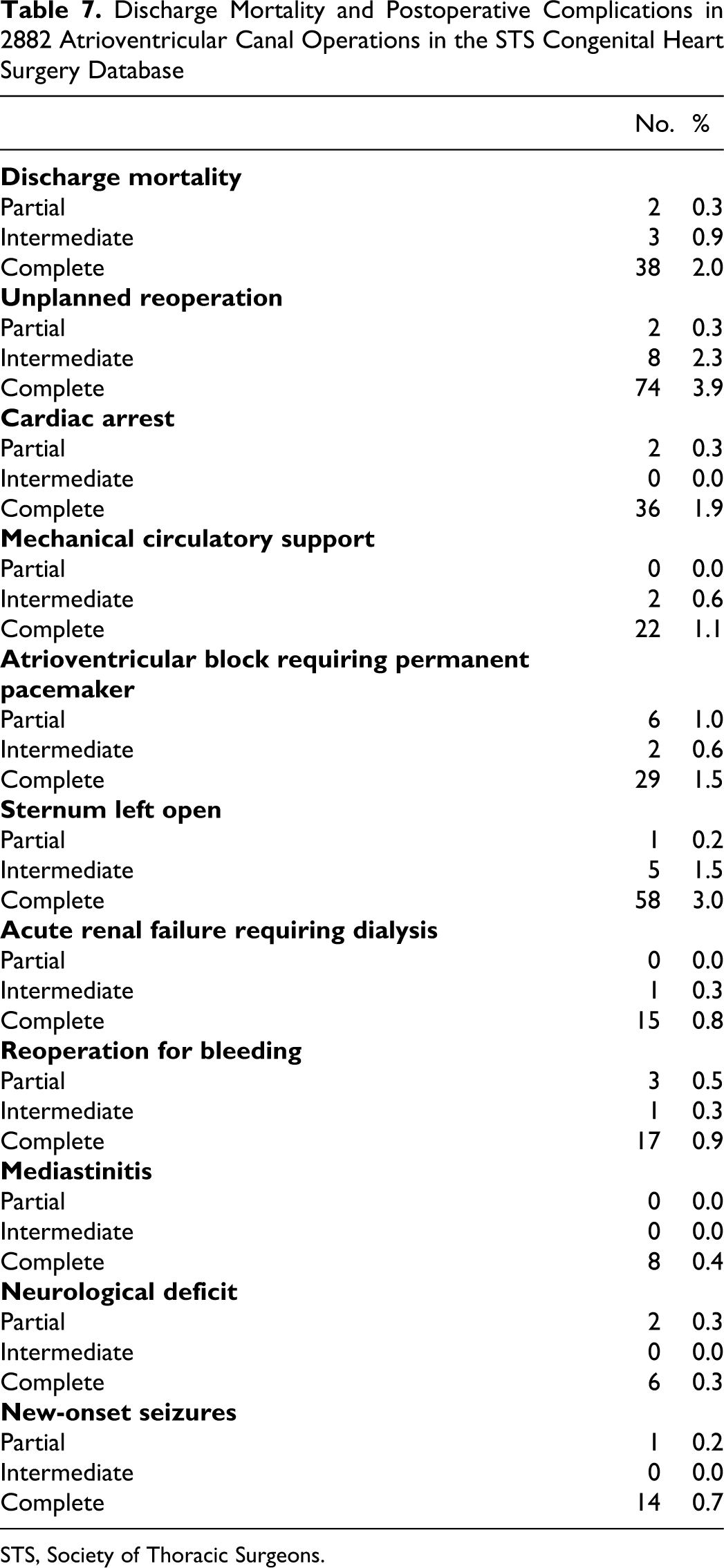
STS, Society of Thoracic Surgeons.
Postoperative Length of Stay in 2882 Atrioventricular Canal Operations in the STS Congenital Heart Surgery Database
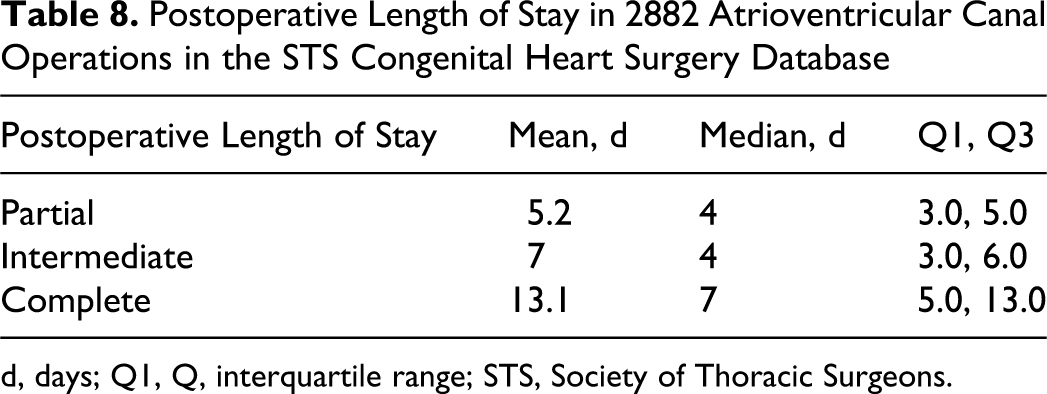
d, days; Q1, Q, interquartile range; STS, Society of Thoracic Surgeons.
Table 1 documents the diagnostic incidence of the following 5 diagnostic groups within the STS Congenital Heart Surgery Database during the 4-year interval of 2005 through 2008, inclusive, regardless of the operation performed: AVC (AVSD), Complete (CAVSD) AVC (AVSD), Intermediate (transitional) AVC (AVSD), Partial (incomplete) (PAVSD) (ASD, primum) TOF, AVC (AVSD) Single ventricle, Unbalanced AV canal Diagnostic Inclusionary Criteria AVC (AVSD), Complete (CAVSD) AVC (AVSD), Intermediate (transitional) AVC (AVSD), Partial (incomplete) (PAVSD) (ASD, primum) Procedural Criteria AVC (AVSD) repair, Complete (CAVSD) AVC (AVSD) repair, Intermediate (transitional) AVC (AVSD) repair, Partial (incomplete) (PAVSD)
Tables 2 through 8 provide preoperative, intraoperative, and postoperative data about surgery for AV canal. In Tables 2 through 8, the data are derived from an analysis of a cohort that is limited to operations performed during the time interval of January 1, 2005, through December 31, 2008, inclusive, with 1 of the following 3 primary diagnoses and 1 of the following 3 primary procedures:
In Tables 2 through 8, the data are derived from an analysis of a cohort that does not include any operations with any primary diagnoses other than the 3 listed above and also does not include any operations with any primary procedures other than the 3 listed above. Thus, in Tables 2 through 8, operations with a primary diagnosis of “TOF, AVC (AVSD)” or “Single ventricle, Unbalanced AV canal” are excluded. The number of operations included in Table 1 is different from the number of operations included in Tables 2 through 8 because of the different inclusionary and exclusionary criteria used for the different analyses, as described above.
Discussion
The STS Congenital Heart Surgery Database is the largest congenital heart surgery database in North America. This review of data from 2882 repairs of AV Canal allows for unique documentation of patterns of practice and outcomes. From this review, we have learned that 98% to 99% of patients survive complete repair of AV canal and 96% to 97% survive complete repair of AV canal with no major complications.
During the 4-year time interval of 2005 through 2008, the STS Congenital Heart Surgery Database documented data about 2882 operations to repair AV canal defects: partial, 623 (21.5%); intermediate, 342 (11.8%); complete, 1917 (66.3%). Mean age at complete repair (years) was partial, 6.1; intermediate, 2.9; complete, 0.6. Median age at complete repair (years) was partial, 2.6; intermediate, 0.9; complete, 0.4. Down syndrome was present in 1767 patients (61.1%).
It is quite clear that pulmonary artery banding is almost never used in patients with partial or intermediate AV canal. It is also only rarely used in patients with complete AV canal. Debanding of the pulmonary artery was rarely performed: partial, 1 (0.2%); intermediate,: 0 (0.0%); complete, 66 (3.4%).
Very few centers are using deep hypothermic circulatory arrest for the repair of patients with complete AV canal. In fact, deep hypothermic circulatory arrest was rarely used for repair of any of the 3 common forms of AV canal: (partial, 6 (1.0%); intermediate, 5 (1.5%); complete, 52 (2.7%).
Discharge mortality was low: partial, 2 (0.3%); intermediate, 3 (0.9%); complete, 38 (2.0%). Atrioventricular block requiring permanent pacemaker occurred but was not common: partial, 6 (1.0%); intermediate, 2 (0.6%); complete, 29 (1.5%). Mean postoperative length of stay (days) was partial, 5.2; intermediate, 7; complete, 13.1. Median postoperative length of stay (days) was partial, 4; intermediate, 4; complete, 7.
Although most patients with AV canal do quite well with surgical repair in the modern era, it is clear that a small subset of patients, usually with complete AV canal, present challenges and do not fare as well. Unplanned reoperation prior to hospital discharge occurred in 3.9% of complete AV canal repairs. The sternum was left open in 3.0% of complete AV canal repairs. Postoperative cardiac arrest occurred in 2% of complete AV canal repairs. Identification of these challenging patients and prevention of these rare but significant complications present a challenge for the future.
The definition of the terms “Balanced AV Canal” and “Unbalanced AV” Canal remain controversial. In April 2000, the International Congenital Heart Surgery Nomenclature and Database Project of the STS and EACTS offered the following definitions and commentary about this topic:
An AVC with two essentially appropriately sized ventricles
18
.
An AVC with two ventricles in which one ventricle is inappropriately small but is thought to be a candidate for a biventricular repair
18
. AVC lesions with unbalanced ventricles so severe as to preclude biventricular repair should be classified as single ventricles. GUEST EDITORS’ NOTE: The term “biventricular unbalanced AV canal” is difficult to pin down in light of a biventricular repair. It also leaves too much room for “gaming” the database, that is, making the patient more complex than he/she actually is. Although some favor removing this term from the hierarchy, others feel strongly to keep it in. We will keep it in place so as to remain inclusive. However, this term may not play a meaningful role in multiinstitutional analysis.”
The above definition has since been updated, and the following definition is currently used by the STS Congenital Heart Surgery Database and the EACTS Congenital Heart Surgery Database, and is published in the STS Congenital Heart Surgery Database Data Specifications Version 3.0, which became the active version of definitions for these databases on January 1, 2010
14
:
“Balanced AVC is an AVC with two essentially appropriately sized ventricles. Unbalanced AVC is an AVC defect with two ventricles in which one ventricle is inappropriately small. Such a patient may be thought to be a candidate for biventricular repair, or, alternatively, may be managed as having a functionally univentricular heart. AVC lesions with unbalanced ventricles so severe as to preclude biventricular repair should be classified as single ventricles.”
It is a fact that the decision of whether to perform a univentricular repair or a biventricular repair may vary from surgeon to surgeon and center to center. Consequently, the operative strategy chosen for a given patient is a variable that by itself should not determine anatomic classification. Obviously this topic remains controversial and will require further clarification in the future. This topic is being actively investigated by Overman and colleagues, who compose “The Unbalanced AVSD Working Group of the Congenital Heart Surgeons’ Society” 19 .
We agree with Robert Professor Anderson when he states, “The presence of the common atrioventricular junction underscores the associated phenotypic features, such as the presence of a trifoliate left atrioventricular valve, which has no resemblance to a cleft.” 20 In hearts with AV canal defects, we use the term “cleft of the mitral valve” as synonymous with the term “zone of apposition of the superior bridging leaflet and the inferior bridging leaflet of the left atrioventricular valve.” We agree that the latter term is more anatomically precise.
We also use the terms atrioventricular septal defect, atrioventricular canal defect, and endocardial cushion defect as synonyms. The key phenotypic feature of a heart with an AV canal defect is a common atrioventricular junction. This common atrioventricular junction may occur with an atrioventricular septal defect, an atrial septal defect only, or rarely, a ventricular septal defect only. It is also possible for a heart with 2 separate atrioventricular junctions to have an atrioventricular septal defect: the Gerbode defect, which permits left ventricular to right atrial communication. 20,21 Although the Gerbode VSD is a type of atrioventricular septal defect, the rare heart with a Gerbode VSD does not have a common atrioventricular junction, and, therefore, the rare heart with a Gerbode VSD is not considered a type of AV canal defect.
The main limitation of this analysis is the main limitation of the STS Congenital Heart Surgery Database: it only allows for analysis of outcomes up to discharge from the hospital. By transforming the STS Congenital Heart Surgery Database into a platform for longitudinal follow-up, 22-24 important information about the intermediate-term and long-term effects of these treatments will become available. Therefore, on January 1, 2010, the STS Congenital Heart Surgery Database began collecting unique patient identifiers compliant with the Health Insurance Portability and Accountability Act (HIPAA) of the federal government of the United States. These unique patient identifiers will allow the STS Congenital Heart Surgery Database to function as a tool for longitudinal follow-up and will lead to the collection of important data about the intermediate-term and long-term status of our patients.
Footnotes
Presented at the Second Scientific Meeting of the World Society for Pediatric and Congenital Heart Surgery at the Fifth World Congress of Pediatric Cardiology & Cardiac Surgery, Convention Centre, Cairns, Queensland, Australia, June 21 to 26, 2009.
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.