
Abstract
Improving mortality rates in children undergoing surgery for congenital heart disease has enabled a shift in focus to improving morbidity, particularly with respect to neurological complications. Various factors have been implicated in influencing neurological outcomes. We share our experience in formulating a customized cardiopulmonary bypass (CPB) protocol based on currently available evidence. Theoretical advantages of intraoperative neuromonitoring during CPB, specifically use of near-infrared spectroscopy, will be discussed in the context of methodologies to monitor cerebral perfusion during surgery.
Keywords
Introduction
As operative mortality in congenital heart surgery continues to decline, there is an increased emphasis on decreasing early and late morbidity. With advancements in surgical technique and the advent of innovative technology, the vast majority of the children born with congenital heart defects (CHDs) will survive to adult life and there are now more adults than children with CHD. 1 It is apparent that these patients face considerable challenges as they progress into adult life including the risks of sudden death, reoperation, and neurocognitive complications. These neurocognitive complications often manifest early in life. Creighton et al showed that 26% of the children that had cardiac surgery as neonates had IQ <85 at five years. 2 Similarly, Majnemer et al showed that 49% of these children have gross motor deficits and 39% have fine motor deficits at five years. 3 The risk of neurological problems is greater for those that have the more severe forms of cardiac disease and especially for those requiring surgical intervention in the neonatal period. It has been reported that the incidence of long-term neurodevelopmental outcomes after neonatal and infant congenital heart surgery ranges from 21% to 69%.3–5
In this brief review, we discuss our approach in attempting to mitigate some of the risks of perioperative neurological injury in neonates with CHD. Specifically, we will focus on the various techniques used as elements of the cardiopulmonary bypass (CPB) protocol at Texas Children’s Hospital emphasizing particularly the use of near-infrared spectroscopy (NIRS) as the neuromonitoring strategy to aid customized CPB.
Neurological Injury in Neonates With CHD
Risk factors associated with neurological injury after cardiac surgery in children are postulated to be multifactorial with prenatal, genetic, socioeconomic, and perioperative factors being implicated. It is becoming increasingly clear that preoperative injury may be an important contributor to this effect. Miller et al showed increased white matter injury in newborns with congenital heart disease. 6 A study from our group confirmed that brain immaturity is associated with pre- and postoperative magnetic resonance imaging (MRI) abnormailities. 7 Limperopoulos et al reported that newborns with abnormal somatosensory-evoked potentials prior to or following open heart surgery had abnormal neurologic examinations both perioperatively and again one year after surgery. 8 Licht et al observed smaller and structurally less developed brains among term infants with hypoplastic left heart syndrome and transposition of great arteries. They concluded that these patients are susceptible to periventricular leukomalacia (PVL) in the perioperative period. 9 Periventricular leukomalacia is cerebral white matter necrosis adjacent to lateral ventricles, resulting from injury to immature oligodendrocytes. Galli et al reported PVL in over 50% of the neonates in their study population after cardiac surgery, a finding not observed in older infants. 10 In relation to genetic susceptibility to neurologic injury, Gaynor et al described an association between certain polymorphisms of apolipoprotein E genotype and low Psychomotor Development Index scores at one year after infant cardiac surgery. 11 It is in this complex environment that efforts are ongoing to optimize individual neurodevelopmental potential. To us, it is logical that efforts to reduce intraoperative cerebral malperfusion or unrecognized ischemia should have a net positive effect on long-term neurodevelopmental potential.
Refining CPB Strategies
Despite considerable progress in the development of CPB strategies for small children, significant challenges remain, particularly, when one considers the potential for brain injury. There have been a number of experimental and clinical studies examining neurological outcomes associated with various CPB strategies. The period of support with CPB is, of course, one element of the continuum of risk that these children face, which the surgeon can strongly influence. As such, it is critical for the operating surgeon to carefully assess currently available data and methodologies as they relate to the potential for impacting neurodevelopmental outcomes.
Low-flow CPB and the use of deep hypothermic circulatory arrest (DHCA) are frequently employed strategies to aid in the conduct of complex congenital cardiac corrections, but some reports suggest that these strategies have been associated with neurologic complications and/or neurodevelopmental abnormalities in up to 50% of patients.12–14 In a piglet model of low-flow hypothermic CPB, Loepke et al observed that neuronal injury occurred predominantly in deep neocortex and in the hippocampus. Factors mitigating injury were higher arterial carbon dioxide, hematocrit (Hct), and blood glucose levels. 15 One of several important findings from the Boston Circulatory Arrest Trial was the observation that the duration of continuous DHCA did not adversely affect the neurological outcome unless it exceeded 41 minutes. 16 In a study looking at the outcomes of neonatal arterial switch operations performed with hypothermic full-flow CPB (150 mL/kg per min), alpha-stat pH management, and minimal periods of hypothermic circulatory arrest, Karl et al observed that the incidence of all perioperative neurologic abnormalities was 20%. Based on the evaluation at late follow-up, they concluded that not all survivors could be considered neurodevelopmentally normal but that the risk of important impairment was low. 17 Pouard et al published their findings regarding the use of normothermic CPB for neonatal arterial switch operations. They compared the results with hypothermic CPB and concluded that not only was normothermic CPB a feasible option but also allowed a faster recovery time. 18 Controversy persists as to the optimal strategy of acid–base and arterial blood gas management during the various phases of CPB. Two commonly used strategies are the pH-stat and the alpha-stat strategy. Studies have shown lower morbidity and shorter recovery for patients managed with pH-stat versus alpha-stat strategy. 19 Kurth et al studied a piglet model of CPB with deep hypothermnic circulatory arrest. They reported that cortical deoxygenation during hypothermic arrest was slower after pH-stat CPB and that the pH-stat strategy of blood gas management was associated with improved neurologic outcomes when compared with the alpha-stat strategy.20,21
Core Principles and Practices of CPB at Texas Children’s Hospital
We follow two basic principles to guide CPB technique at our institution. We aim to deliver “adequate” amounts of oxygenated blood to both cerebral hemispheres during all phases of CBP. Second, we try to avoid or minimize the use of any technique that violates the first core principle.
Our strategy is based primarily on the use of full-flow CPB (≥150 mL/kg per min). We aim to minimize and eliminate wherever possible the use of low-flow CPB and DHCA. For procedures that could alternatively be performed utilizing DHCA, such as aortic arch reconstruction and Norwood stage I palliation, we favor continuous bypass with selective antegrade cerebral perfusion (ACP) during the arch reconstruction. The basic technique, now uniformly adopted, was described by Pigula et al as a means of reducing circulatory arrest time and maintaining cerebral blood volume and oxygen saturation. 22 We have modified the original technique with some critical differences relating to flow rates and cerebral physiologic monitoring. 23 We use bilateral NIRS and transcranial Doppler (TCD) ultrasound to guide ACP. Flow rates used during ACP at our institution are almost double the rates that others have reported.24–26 Our strategy is highly influenced by the observation that flow rates of <30 mL/kg per min may not provide adequate cerebral blood flow to some patients. 27 Pigula and associates studied a cohort of patients that had undergone a stage I Norwood palliation with either regional low-flow perfusion of the brain (ACP) or DHCA. Neurodevelopmental outcomes were not significantly different for the two groups at one year. 28 This was a nonrandomized study. We believe that the ACP flow rates used in this study (30-40 mL/kg per min) may be less than optimal for some patients.
We favor the use of a pH-stat strategy of acid–base management in neonates in all phases of CPB. Some centers still use alpha-stat management and although there are pros and cons to both techniques, pH-stat has been shown by some to be associated with reduced perioperative morbidity in infants when compared with alpha-stat. 19
We use Hct levels ranging from 30% to 35% on CPB. Jonas et al demonstrated in a single-center randomized trial that neonates who were maintained at Hct of around 20% during hypothermic CPB had poorer perioperative and developmental outcomes than those maintained at Hct of about 30%. 29
We emphasize slow cooling over no <20 minutes to deep hypothermia (18°C-20°C). Figure 1 demonstrates a typical NIRS recording obtained during a case conducted using the above-mentioned CPB protocol in our institution. A study published by our group on 20 neonates that underwent aortic arch reconstruction using this CPB strategy showed excellent short-term survival and clinical outcomes. Bilateral NIRS showed regional cerebral oxygenation saturation (rSO2) of 87% to 95% during ACP. 30 Table 1 summarizes the CPB strategy used in our institution.
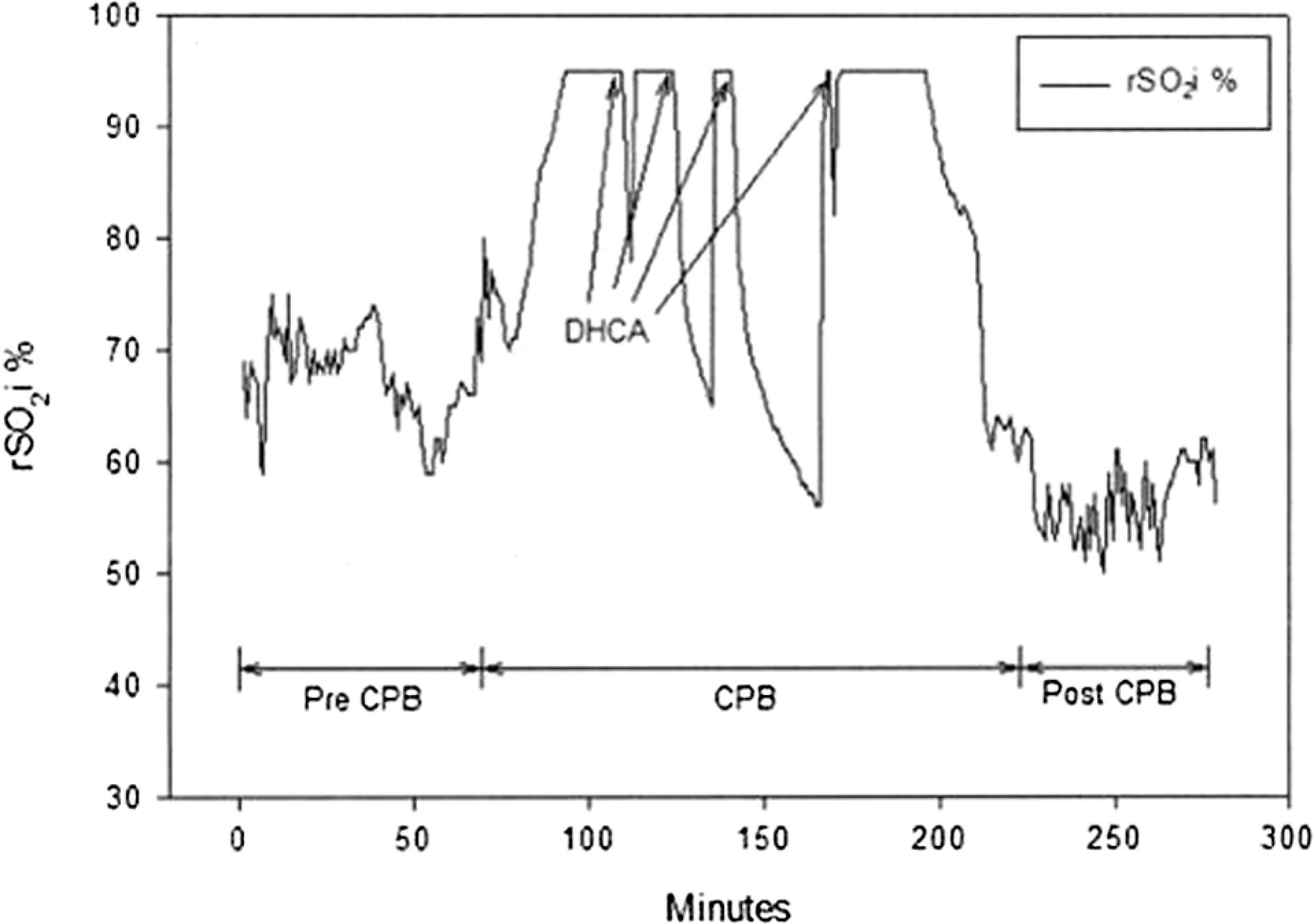
A near-infrared spectroscopy (NIRS) graph showing regional cerebral saturation of oxygen index (rSO2i) in a neonate with an unbalanced complete common atrioventricular canal defect (left ventricular dominance) and infradiaphragmatic total anomalous pulmonary venous return. This patient underwent four periods of deep hypothermic circulatory arrest (DHCA) at 18°C of 3, 12, 26, and 1 minute duration, respectively, for a total of 42 minutes. We used hematocrit (Hct) >30%, slow cooling over >20 minutes, pH-stat, full-flow CPB at 150 mL/kg per min and rSO2 was kept above 90% before DHCA. The rSO2i was not allowed to fall beyond baseline levels during the entire period from initiation of CPB to end of support.
Core Practices of the CPB Strategy in Texas Children’s Hospital
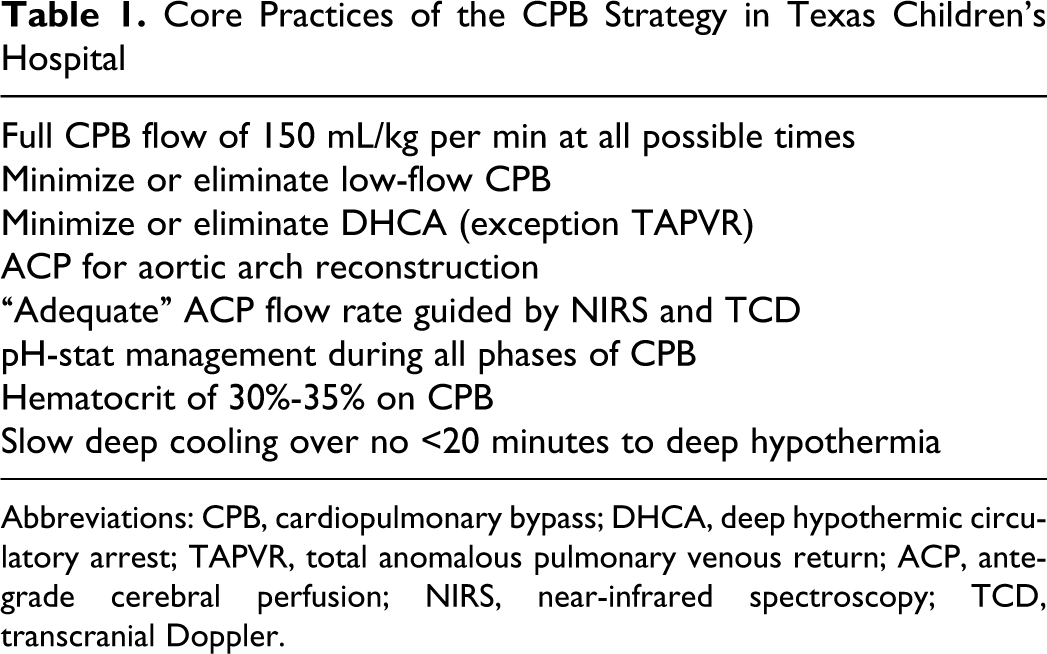
Abbreviations: CPB, cardiopulmonary bypass; DHCA, deep hypothermic circulatory arrest; TAPVR, total anomalous pulmonary venous return; ACP, antegrade cerebral perfusion; NIRS, near-infrared spectroscopy; TCD, transcranial Doppler.
NIRS Monitoring of Cerebral Oxygen Saturation during CPB
Near-infrared spectroscopy is a noninvasive optical technique used to monitor brain tissue oxygenation. Near-infrared spectroscopy monitoring tools for pediatric patients use different algorithms than those used for adults. Near-infrared light at 730 and 810 nm wavelengths is used to estimate relative amounts of oxygenated and deoxygenated hemoglobin (Hb) in the cerebral blood. Also, there is a subtraction algorithm for the thinner pediatric skull and extracranial tissue compared with adults. 31 One light-emitting diode is used that emits near-infrared light to a portion of the frontal cerebral cortex and is detected through two detectors placed three and four centimeters from the emitter. The device that we use is the Somanetics INVOS system which is US Food and Drug Administration (FDA) approved. It displays a numerical result as rSO2 index (rSO2i). This index is a ratio of oxygenated Hb to total Hb in the light pathway and is reported as a percentage ranging from 15% to 95%.
Near-infrared spectroscopy can accurately estimate cerebral oxygenation during cardiac operations. 32 Blood in the cerebral circulation is predominantly venous and this accounts for the relationship of the rSO2 measured by NIRS to the oxygen saturation in the jugular venous bulb. Daubeney et al reported a comparison between the two and showed excellent correlation. 32 However, as Tortoriello et al reported, although NIRS can predict trends in cerebral oxygen saturation quite well, it cannot predict absolute values of systemic venous oxygen saturation (SvO2) solely through measurement of rSO2. 33
In a study of cerebral oxygenation during pediatric cardiac surgery with deep hypothermic circulatory arrest in 26 patients, Kurth et al observed that postoperative neurologic status was abnormal in three (12%) patients. The cerebrovascular hemoglobin oxygen saturation (SCO2) increase during deep hypothermic CPB was less in these three patients than in the remaining study population. There were no other significant SCO2 differences between outcome groups. 34 Hoffman et al investigated potential relationships between SvO2 following the Norwood stage 1 procedure and childhood neurodevelopmental outcomes. Participants scored significantly below the population mean for motor, visual–motor integration, and composite neurodevelopmental outcomes at age of four years. 35 The five (of 13) patients with abnormal outcomes had significantly lower postoperative SvO2 values than those with normal outcomes (46% ± 8% vs 56% ± 6%, P = .024). Standard hemodynamic parameters did not differentiate patient outcomes. The risk of abnormal outcome increased with increasing time at a SvO2 of <40% (P < .001).
A study by Dent et al involving brain imaging by MRI after Norwood stage I palliation showed that nine of the ten neonates with rSO2 <45% for >180 minutes during the perioperative period had new ischemic MRI lesions. 25 Austin et al reported a benefit associated with multimodality neurophysiologic monitoring during pediatric cardiac surgery in a cohort of 250 patients. Obvious neurologic sequelae occurred in 7% of patients for whom monitoring had not detected noteworthy changes in cerebral perfusion or metabolism, and 6% in whom noteworthy changes were followed by an intervention that altered patient management. In contrast to this, obvious neurologic sequelae occurred in 26% of patients in whom changes were detected by monitoring but were not followed by an intervention. 36
Near-infrared spectroscopy may be very sensitive in detecting altered perfusion and oxygen delivery and thus may help to avert disasters during operation, particularly in neonates and infants. Sakamoto et al reported on the detection of cerebral ischemia caused by an obstructed superior vena cava cannula with the help of NIRS, which could not be identified by other monitoring modalities. 37 Gottlieb et al reported on the recognition of aortic cannula displacement during cardiac surgery through bilateral NIRS monitoring of rSO2. The authors felt that the aortic cannula malposition would not have been detected using standard monitors. 38
In our institution, we employ bilateral NIRS in all aortic arch repairs as a guide to ACP. We have earlier shown the efficacy of ACP to provide comparable blood flow to both cerebral hemispheres with bilateral NIRS and TCD as guides to adequacy of the flow.30,39 We also use NIRS in cases that require DHCA to guide our strategy of minimizing the duration of DHCA and to help assess adequacy of perfusion during the cooling phase of CPB prior to DHCA. We use NIRS to help confirm proper cannula positioning and also for monitoring during closed heart procedures such as coarctation repairs and placement of systemic to pulmonary artery shunts.
Bilateral NIRS as a Guide to ACP
Antegrade cerebral perfusion is a technique devised to avoid or minimize DHCA during procedures such as aortic arch reconstruction and Norwood stage I palliation in neonates (Figure 2 ). Pigula et al demonstrated that with ACP use there is blood flow both to the brain and to subdiaphragmatic structures.22,40 As discussed earlier, the ACP technique that we use is a modification of their strategy; the critical differences being the neurophysiologic monitoring with bilateral NIRS and ACP flow rate. We have good success in terms of outcomes for our patients that require aortic arch repair on ACP. 41
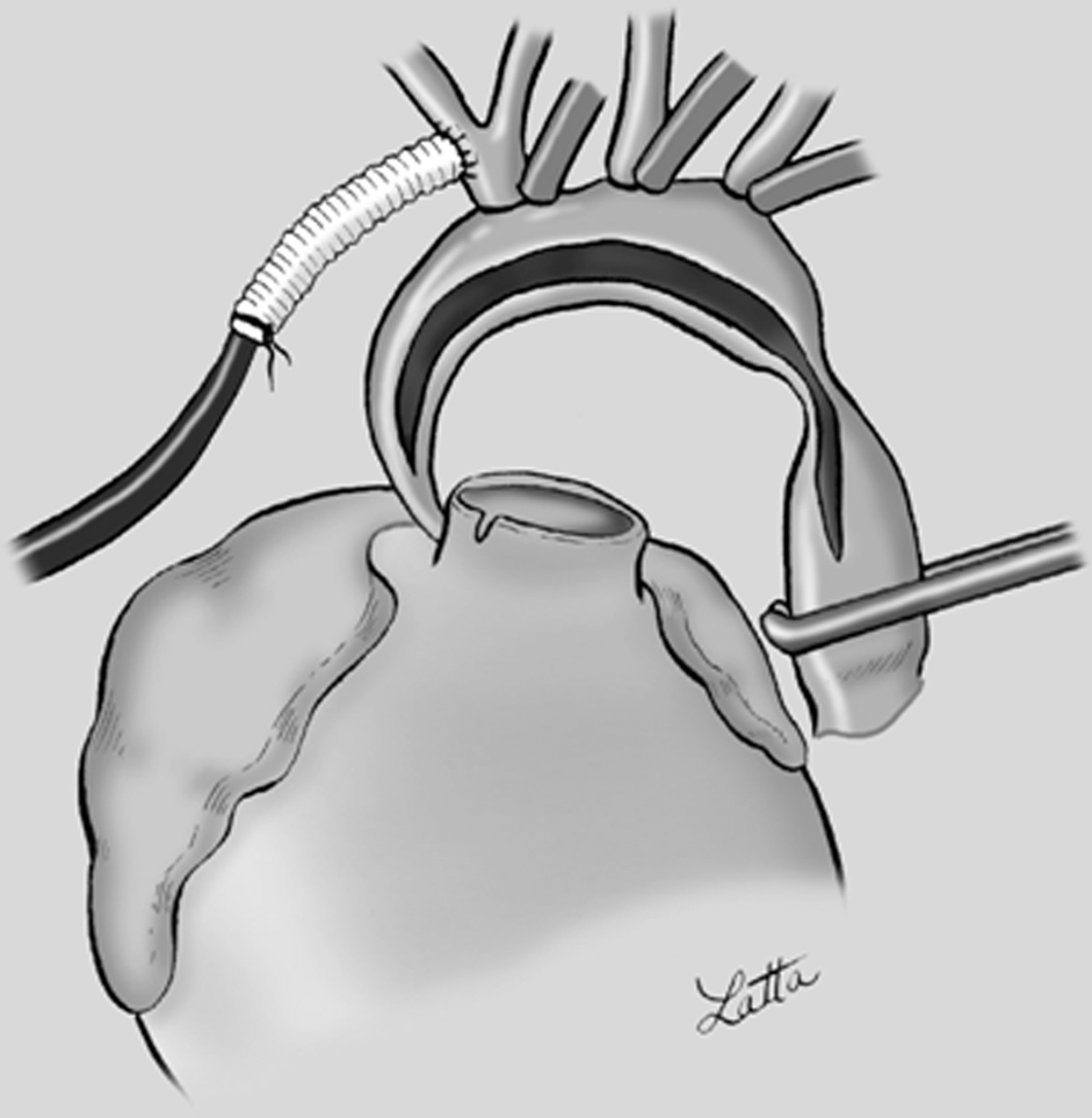
Depiction of the operative field during aortic arch recontruction with antegrade cerebral perfusion (ACP). Arterial inflow is through the cannulated three to four mm polytetrafluoroethylene (PTFE) graft following anastomosis of the graft to the innominate artery. Exposure is maintained by gentle retraction on the brachiocephalic vessel snares and a snare or clamp on the descending aorta and the right atrial cannula.
We use bilateral NIRS to guide ACP during cardiac surgery. This strategy stems from the published studies that demonstrated lower rSO2 on the left side of brain compared with the right side, while on ACP. The reasons for this disparity may be multiple, including the fact that all blood flow to the left side during ACP is through the circle of Willis. Other reasons for these findings may include anatomic variations, obstructed left-sided venous drainage or positioning of the patient.30,39,42 Hence, without left-sided monitoring strategy, left-sided desaturations may go undetected.
Future Neuroprotection Studies
Studies are currently underway examining novel techniques to improve neurological outcomes after neonatal cardiac surgery. One of these studies includes looking at the role of erythropoietin (EPO) at improving neurodevelopmental outcomes at one, three, and five years of age. Erythropoietin has been shown to have multiple biologic roles including neurological and cardioprotective effects. 43 Neonates are ideal candidates for this therapy as the timing of the neurologic insult is known, thus allowing appropriate time for the effect of EPO to occur.
In the recent past, there has been concern about the use of anesthesia and its effect on neurodevelopment on neonates.
44
On the other hand, it is also known that anesthetics like ketamine that antagonize N-methyl-
An ongoing study by our group is using brain MRI, electroencephalogram, and neurodevelopmental outcomes to assess the effects of our high-flow CPB and increased oxygen delivery strategy on new hypoxic brain injury after cardiac surgery in neonates. The hypothesis is that our CPB strategy may reduce the incidence of hypoxic–ischemic brain lesions postoperatively compared to that in previously published reports. Early results have shown a strong relationship of postoperative white matter injury to preoperative brain injuries and single-ventricle anatomy. No association of brain injury has so far been established between the gestational age at birth, use of ACP versus full-flow CPB or rSO2 <45% for >240 minutes in the perioperative period. The study is currently enrolling patients and will include planned follow-up evaluations out to five years.
Conclusion
Although our CPB strategy has not been conclusively demonstrated to be superior to others, considerable evidence exists that can help in formulating a successful customized CPB protocol. Inadequate cerebral blood flow has been strongly associated with poor neurological outcomes and providing adequate blood flow during all phases of CPB is the goal of most strategies. We believe that this is facilitated by continuous monitoring of cerebral perfusion, which can be reliably achieved through the application of bilateral NIRS and TCD. Our CPB strategy has shown promise and we are encouraged by our preliminary outcomes. However, further studies looking at long-term neurological outcomes are required and are currently underway.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presented at the Fourth Annual Symposium of the Walter Sisulu Paediatric Cardiac Centre for Africa, Johannesburg, South Africa; March 23–24, 2011.