
Abstract
Background: Pediatric extracorporeal membrane oxygenation (ECMO) programs are sophisticated endeavors usually found only in high-volume cardiac surgical programs. Worldwide, many cardiology programs do not have on-site pediatric cardiac surgery expertise. Our single-center experience shows that an organized multidisciplinary rescue-ECMO program, in collaboration with an accepting facility, can achieve survival rates comparable to modern era on-site ECMO. Methods: A retrospective review was conducted of all patients initiated on rescue-ECMO from 2004 to 2009 in a single academic pediatric hospital without a pediatric cardiac surgery program. All aspects of ECMO were formalized using Failure Mode Effects Analysis. Results: Eight patients were initially cannulated for ECMO at our institution. Six were subsequently transported by air to the receiving facility 1,305 km away. Extracorporeal membrane oxygenation was initiated in 0.2% of our Pediatric Intensive Care Unit admissions and in 0.52% of all our pediatric cardiac patients. Mean age was 4.0 years (7 weeks to 15 years). Indications for ECMO initiations were cardiogenic shock (n = 5) and acute respiratory distress syndrome (n = 3). Six had veno-arterial- and two had veno-veno ECMO. Two patients were not transported (one death and one weaned locally). Six patients were successfully transported within 2 to 24 hours, with a survival to hospital discharge rate of 67% (four of six). Median total time on ECMO was 5.5 days. Complication rate was 50% (4/8). Conclusions: Our rescue-ECMO survival results were comparable to that of current published results from established pediatric ECMO programs. Air transport of ECMO patients can be performed safely using an organized multidisciplinary team approach.
Keywords
Background
Many critically ill patients not responding to conventional therapies have mortality rates of 75% to 100%, without access to extracorporeal life support (ECLS). In the current era, rescue-extracorporeal membrane oxygenation (ECMO) has regained favor as a life-saving treatment modality for pulmonary and cardiac patients in extremis. Modern day publications of observational studies have revealed survival rates of 41% to 73% (see Table 1 ).
ECMO Survival Rates Summary
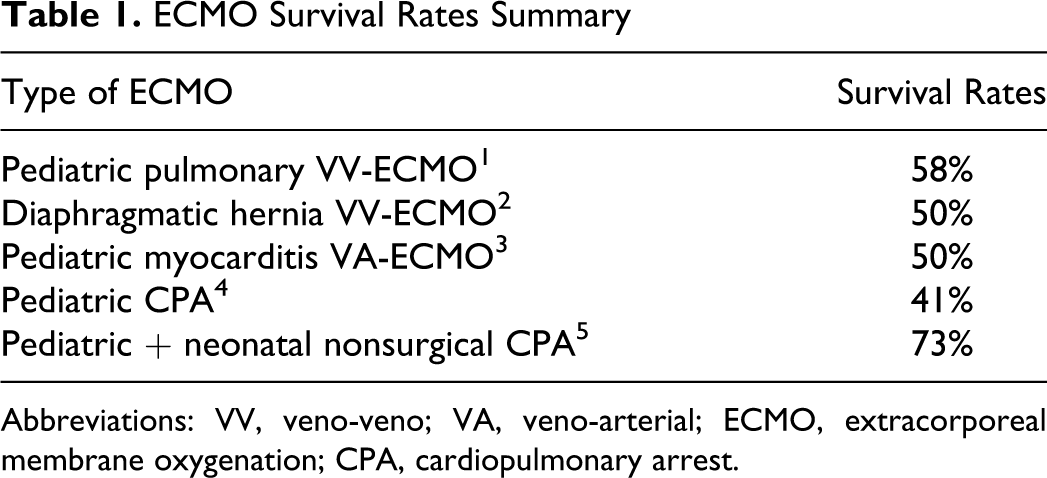
Abbreviations: VV, veno-veno; VA, veno-arterial; ECMO, extracorporeal membrane oxygenation; CPA, cardiopulmonary arrest.
The dilemma in ECMO is that it is a highly specialized, high-risk and costly treatment modality that is currently reserved for centers with cardiac surgery and designated ECMO programs. Many cardiology programs across the world do not have local pediatric cardiac surgery expertise/programs available and thus ECMO is not offered.
Through this review, our goal is to show that rescue-ECMO can be initiated successfully in centers without an official ECMO or pediatric cardiac surgery program. Patients can then safely be transported by air (which has not yet been reported in pediatric literature) to a designated facility with such programs while still achieving acceptable survival rates comparable to recent ECMO publications. There is little published data on the incidence of ECMO usage in the pediatric population (excluding post cardiotomy patients). We present the incidence in our institution.
Winnipeg Children’s Hospital (University of Manitoba) does not have a cardiac surgery program. Until 2004, an ECMO program also did not exist. However, full Pediatric Cardiology services have been available at the hospital through the Variety Children’s Heart Centre for the last 50 years. University of Manitoba also has a well-established adult cardiac surgery program performing over 1,200 open heart cases per year. In 2007, an official adult ECMO program was established.
During the summer of 2004, a nine-year-old boy in cardiogenic shock required ECMO after failure of conventional therapies. Innovative medical staff committed to best patient care with the assistance of an adult cardiac surgeon led to the first cannulation in Winnipeg. He was airlifted with a Hercules aircraft to Edmonton (1,305 km), where he was eventually weaned and survived to hospital discharge. This was the birth of the Winnipeg pediatric rescue-ECMO program.
In rescue-ECMO, multidisciplinary team approach is important in ensuring best patient outcome. Extensive coordination is needed in the shortest time frame possible. Doing this on an ad hoc basis may lead to patient compromise. The evolution to our current status, criteria, and flow charts will be discussed.
Methods
A retrospective review of all pediatric ECMO cases at The Winnipeg Children’s Hospital from January 2004 to December 2009 was undertaken using the Western Canadian Children's Heart Network Database as well as the Variety Children’s Heart Centre Database. This retrospective review received the approval of the University of Manitoba Health Research Ethics Board. Fourteen pediatric patients were identified receiving some form of ECLS. Only 8 patients were cannulated for conventional ECMO in Winnipeg. The excluded 6 patients had received either NOVO-Lung, continuous renal replacement therapy with an in-line oxygenator or were transported and then cannulated in Edmonton. These patients were excluded from the review.
Denominators for incidence calculation were obtained from the pediatric intensive care unit (PICU) logbook (incidence per PICU admissions) as well as the Variety Children’s Heart Centre Database (Cardiac ECMO per total number of new pediatric cardiac patients). The incidence of ECMO initiation in PICU admissions was 1 (0.28%) in 359 patients per year. The incidence of Cardiac ECMO in cardiac patients was 1 (0.52%) in 192 patients per year.
Parameters reviewed included age, diagnosis, type of ECMO, ECMO cannulator, time on ECMO in Winnipeg, total ECMO-time, ECMO-related complications, and supportive treatment on ECMO.
Outcomes reviewed were (a) overall 30 day/in-hospital survival, (b) transport survival, (c) wean success, and (d) complication rate.
Inclusion criteria for ECMO eligibility were weight >7.5 kg (limitations due to adult ECMO circuit used in all patients), acute respiratory distress syndrome (ARDS) in previously healthy patient, palliated congenital heart disease and other patients with severe cardiac dysfunction/cardiogenic shock, and patients not responding to maximal standard medical therapy. Exclusion criteria for patients were evidence of brain death, extensive interventricular hemorrhage, mechanical ventilation >14 days, irreversible or untreatable cardiopulmonary etiology.
Pre-ECMO, all patients were supported with mechanical ventilation and maximal inotropic support if needed. All patients failed maximal conventional therapies including high-frequency oscillation. Extracorporeal membrane oxygenation cannulation was performed with at least two members with cannulation training or experience. They consisted of dedicated adult cardiac surgeons, pediatric general surgeons, and pediatric interventional cardiologists.
Results
The data collected is summarized in Table 2 . One patient with a diagnosis of ARDS had premorbid Ventricular Septum Defect (VSD) and patent ductus arteriosus (PDA) with significant L-to-R shunting. This patient was initiated on veno-veno (VV)-ECMO but eventually required conversion to veno-arterial (VA)-ECMO.
Data Summary
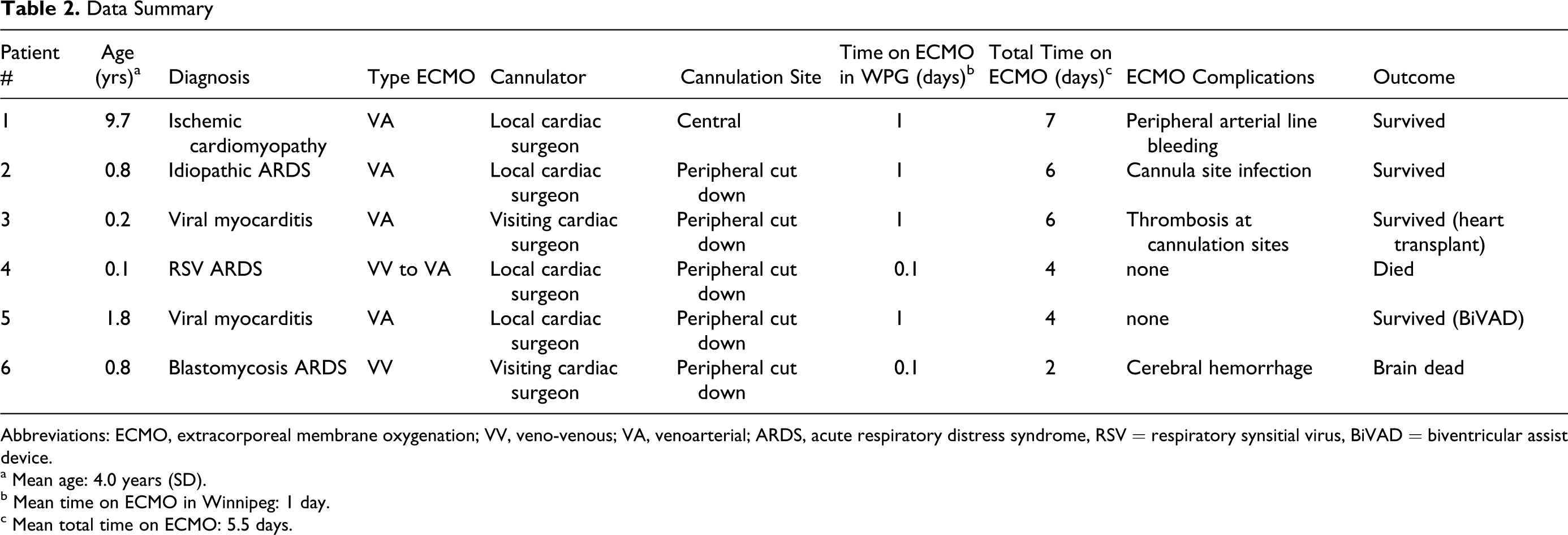
Abbreviations: ECMO, extracorporeal membrane oxygenation; VV, veno-venous; VA, venoarterial; ARDS, acute respiratory distress syndrome, RSV = respiratory synsitial virus, BiVAD = biventricular assist device.
a Mean age: 4.0 years (SD).
b Mean time on ECMO in Winnipeg: 1 day.
c Mean total time on ECMO: 5.5 days.
One patient required continuous renal replacement therapy (CRRT) after ECMO cannulation. Six patients were transported within 2 to 24 hours. Two additional patients were cannulated but remained in Winnipeg. Both of these patients had pre-hospital arrests. They were weaned off ECMO once a diagnosis of irreversible severe ischemic encephalopathy was confirmed.
Table 3 summarizes the survival outcomes. Of note, there was 100% air transport survival on ECMO (Figure 1 ). One patient was weaned from ECMO and converted to a biventricular assist device as bridge to eventual heart transplantation. Another patient was weaned and eventually received a heart transplant. There was one complication during air transport related to cannula site bleeding. Complication rate secondary to ECMO was 50% (four of eight). Other complications included cannula site infection and cannula site thrombosis.
Outcomes Summary
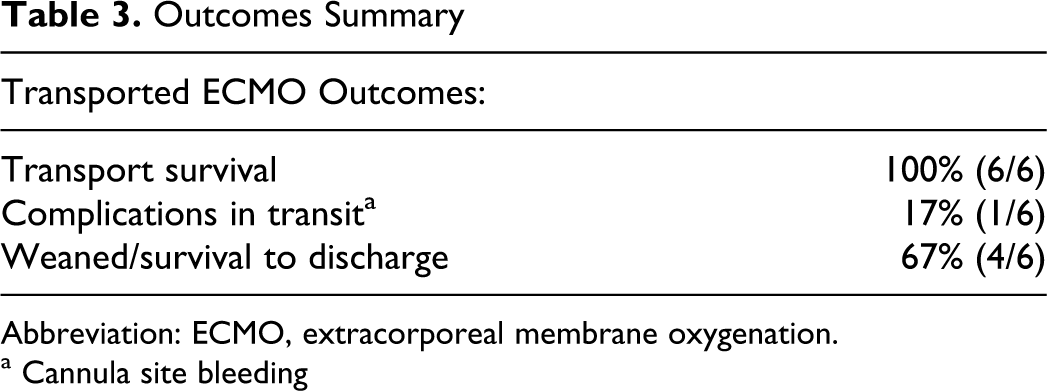
Abbreviation: ECMO, extracorporeal membrane oxygenation.
a Cannula site bleeding
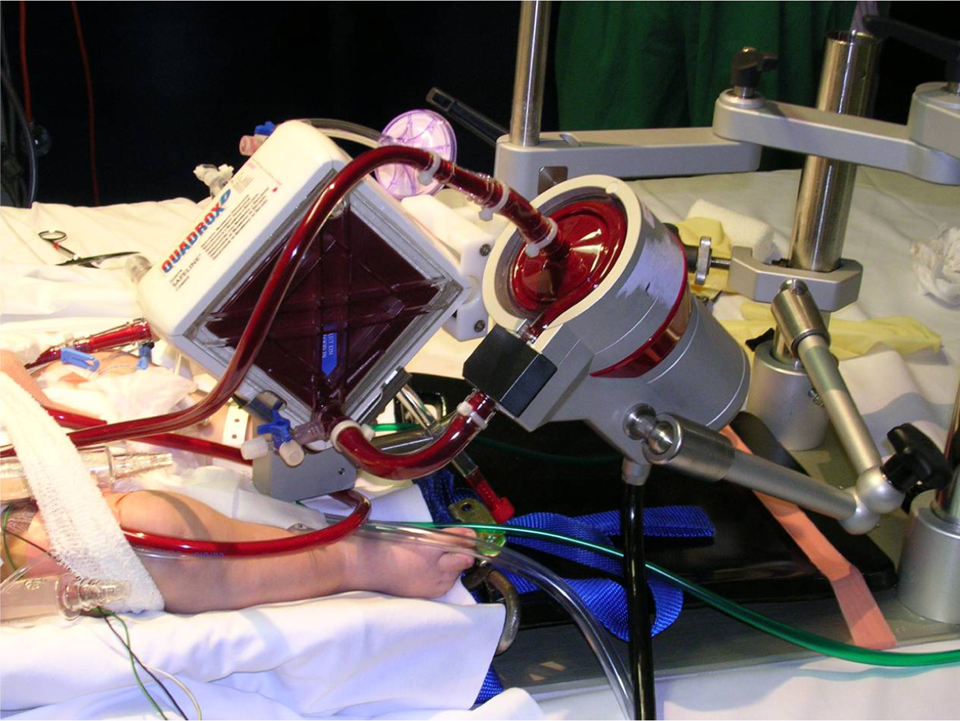
Mobile pediatric ECMO set-up during air transport.
Two patients in the cohort diagnosed with ARDS and sepses died at the receiving center. One patient died from a severe cerebral hemorrhage while on ECMO. The other had portal vein thrombosis diagnosed pre-ECMO and succumbed due to overwhelming sepsis.
Discussion
Despite a small number of cases, our rescue-ECMO program survival rates are comparable to modern published data. Our study indicates that initiation and cannulation of ECMO at the referring center can be performed by trained local staff and then subsequently transported successfully. The advantage of this approach is that it eliminates the wait time of up to 12 hours for the cannulation team to fly in before ECMO is initiated. Earlier cannulation and ECMO support with earlier organ reperfusion can lead to greater organ salvage and ultimately patient stabilization. By the time the transport team arrives, the patient is already stabilized for air transport.
Our rescue-ECMO program model (local cannulation expertise by adult cardiac surgeon/pediatric general surgeon/pediatric cardiologist and perfusionists, stabilization, fixed wing air transport) is currently the first and only one of its kind in Canada. We believe this can be a blue print for the development of rescue-ECMO programs in other parts of the world. Emphasis is placed that our “rescue-ECMO” is not “ECMO-cardiopulmonary resuscitation (ECPR),” as ECMO is not part of the CPR protocol in our institution.
At the time of our first ECMO case in 2004, there was no rescue-ECMO program. We started with a patient in extremis, cardiologists and intensivists with vision, an adult cardiac surgeon with pediatric ECMO experience, and an able and willing receiving facility. Our major limitation was to adapt the adult ECMO circuit (i.e. tubing, cannulas, pump, etc.) to our nine-year-old patient. As the patient had previous congenital cardiac surgical repair, central cannulation (16F Argyle inflow cannula to aorta and 28F outflow cannula from right atrium) was performed utilizing the adult circuit. Another major logistical issue with this case was deficient power supply in the aircraft.
In 2005, we cannulated an infant with a 14F dialysis catheter through peripheral cut down technique and initiated ECMO with the same adult ECMO circuit. This led to the realization that (i) a stock of pediatric cannulas were needed and (ii) a formal program/protocol needed to be formulated.
The Stollery Children’s Hospital in Edmonton, Alberta, became our receiving facility. With their input and collaboration, we adopted the same ECMO system and circuit for consistency. Table 4 summarizes the components currently used in our rescue ECMO program. The system allows safe and effective support for patients >7.5 kg.
Pediatric ECMO-Circuit Components
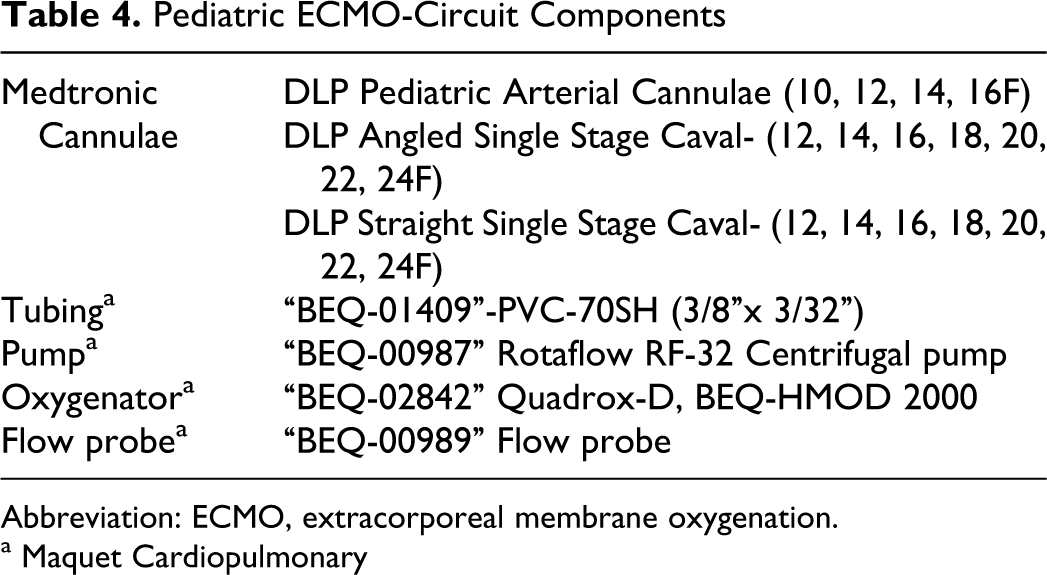
Abbreviation: ECMO, extracorporeal membrane oxygenation.
a Maquet Cardiopulmonary
In September 2005, the Winnipeg Regional Health Authority (WRHA) called together a multidisciplinary team to perform a “Failure Mode Effects Analysis” (FMEA) on rescue ECMO. 6 The Goal with FMEA was “… to facilitate designing as much safety as possible into the procedure ….” Three phases were identified to be addressed: (1) patient selection, (2) establishment and maintenance, and (3) transport. Flow charts (Supplemental Figures 2–4) were created, each step analyzed for failure modes and failure effects (Supplemental Figure 1 ), and finally action plans and accountabilities determined to prevent failures. Major risk areas identified were patient selection and preparation, as well as timely blood product availability. Supplemental Figures 2–4 represent the flow charts we designed and emphasize the extent of the logistics leading to successful rescue-ECMO initiation and transport.
The incidence of patients needing ECMO at our institution was insufficient to support a full-scale ECLS program. Collaboration between referring and receiving centers resulted in the creation of a protocol that includes rapid mobilization of the transport team, standardized cannulation, and ECMO initiation. Competency is maintained by sending members of the rescue-ECMO team to Edmonton to attend their ECMO-training course. An adult cardiac surgeon with ECMO experience and a perfusionist are present for all cannulations. We believe ECMO cannulation/initiation is most successful when done in a multidisciplinary team approach.
Using this protocol, fixed wing air transport of children on Rescue-ECMO was associated with survival and complication rates comparable to current published results from established pediatric ECMO programs.
In conclusion, for patients in extremis, early initiation of a rescue-ECMO protocol at the referring hospital can be lifesaving. This multidisciplinary approach if properly implemented can minimize delay and adverse outcomes. It has the potential to make lifesaving technology more accessible to extremely ill children across Canada and the rest of the world.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.