
Abstract
Background: We sought to determine whether immediate postoperative serum cortisol concentration predicts adrenal insufficiency in neonates after cardiac surgery with cardiopulmonary bypass. We hypothesized that cortisol <10 µg/dL would be associated with increased catecholamine requirements and fluid resuscitation and would predict hemodynamic responsiveness to exogenous steroids. Methods: Retrospective study of 41 neonates was carried out for the levels of cortisol in the immediate postoperative period; of whom, 15 received steroids due to high levels of inotropic support. Laboratory and clinical outcomes were collected. Results: Median cortisol was 12 µg/dL (interquartile range: 5.2-27.4). Levels of cortisol <10 µg/dL was not associated with any clinical variable indicative of increased illness severity. Peak lactate (9.1 vs 11.8 mmol/L, P = .04) and maximum arteriovenous saturation difference ([Sa
Keywords
Introduction
Growing evidence suggests that children and neonates with congenital heart disease may suffer from inadequate corticosteroid activity relative to their severity of illness after cardiopulmonary bypass (CPB). This so-called critical illness-related corticosteroid insufficiency (CIRCI) 1 may contribute to hemodynamic instability and capillary leak in the postoperative period. A few small studies have reported a benefit from corticosteroid replacement in these patients, including improved hemodynamics in children with fluid- and catecholamine-refractory hypotension.2–4 However, little evidence exists regarding the best method to identify which patients may benefit from corticosteroid treatment. Low serum total or free cortisol, response to adrenocorticotropic hormone (ACTH) stimulation test, high ACTH/cortisol ratio, and improvement in hemodynamics after corticosteroid administration have all been used as surrogates for CIRCI, with inconsistent results.5–7 As corticosteroid therapy has associated risks, 8 prospective identification of the steroid-responsive population is desirable. In this study, we sought to determine whether serum cortisol obtained from neonates in the immediate postoperative period after CPB is associated with greater need for fluid resuscitation and inotropic support and whether it can predict steroid responsiveness. We hypothesized that the levels of cortisol <10 µg/dL would be associated with higher inotropic support, a greater degree of fluid resuscitation, and a favorable hemodynamic response to exogenous steroids, supporting presence of CIRCI.
Methods
Patients
We identified all neonatal patients who underwent CPB and surgery of complex congenital heart disease between January 2009 and September 2010. Patients with the levels of serum cortisol obtained in the immediate postoperative period were included in this study for analysis (n = 41). Data were extracted from the cardiac intensive care unit (CICU) clinical database and patients' electronic medical records. The Institutional Review Board, University of Alabama, Birmingham, AL, approved this study.
Operative Management
Patients with single ventricle lesions underwent the Norwood procedure (NP) with the placement of a 5-mm ringed GORE-TEX shunt from the right ventricle to the pulmonary artery bifurcation except when precluded by anatomy. Arterial switch operations (ASOs) were performed utilizing a standard Lecompte maneuver ± ventricular septal defect (VSD) repair. Truncus arteriosus repair was performed with VSD closure, commitment of the common arterial trunk to the left ventricle, and placement of a valved conduit from the right ventricle to patch-augmented pulmonary arteries. Total anomalous pulmonary venous connection (TAPVC) repair was performed via direct anastamosis of the pulmonary venous confluence to the left atrium. Interrupted aortic arch (IAA) lesions were repaired with an end-to-end anastamosis of the aorta with patch augmentation plus VSD closure.
Intraoperatively, patients were cooled to 22°C (NP and IAA) or 28°C (all others). Selective low-flow cerebral perfusion was utilized during aortic arch reconstruction. All the patients received zero-balance ultrafiltration during CPB and single-pass ultrafiltration after CPB. A peritoneal drain was placed in all the patients in the operating room (OR). The sternum was left open in all the patients undergoing NP and in any other patient experiencing high inotrope requirements or abnormal bleeding per the surgeons' discretion. All the patients received 10 mg/kg methylprednisolone eight hours and one hour before transport to the OR. No intraoperative steroids were given.
Postoperative Management
Our CICU neonatal management focuses on a hemodynamic goal-oriented approach with vasoactive agent titration, ventilator adjustments, and colloid boluses to achieve the following general goals within the first 24 hours after complex neonatal repairs: mean arterial pressure 40 to 55 mm Hg, central venous pressure (CVP) eight to 12 cm H2O, pulse oximetry 75% to 85% (NP) or >95% (all others), heart rate (HR) <170, arteriovenous oxygen saturation difference (Sa
Cortisol Measurement and HC Administration
Serum cortisol was routinely measured on arrival to the CICU and/or prior to initiating hydrocortisone (HC) therapy. Patients requiring epinephrine ≥0.1 or >0.07 µg/kg/min plus any dose of vasopressin despite adequate preload, normal hemoglobin, and ionized calcium received IV HC (100 mg/m2/d). Hydrocortisone was continued if a hemodynamic response was apparent or for a cortisol <20 µg/dL. After the need for high-dose vasoactive medication infusions was subsided, HC was tapered over five days. Adrenocorticotropic hormone stimulation tests were not routinely performed.
Definitions
Inotrope score (IS) was modified from Gaies et al 9 and Wernovsky et al 10 as follows: 1× dopamine dose (µg/kg/min), plus 10× milrinone or phenylephrine dose (µg/kg/min), plus 100× epinephrine or norepinephrine dose (µg/kg/min), and 10,000× vasopressin dose (U/kg/min). A hemodynamic response to HC was defined as a 50% reduction in IS within 24 hours of the initial HC bolus. Cortisol <10 µg/dL was identified a priori as a threshold for “low” cortisol and CIRCI per recent consensus statement from the American College of Critical Care Medicine. 1
Data Analysis
SPSS 19 (SPSS Inc, Chicago, Illinois) was used for all statistical tests. Continuous variables not normally distributed were summarized as a median with range, with group comparison performed using the Wilcoxon rank sum test. Continuous variables with a normal distribution were summarized as means with standard deviations and compared using the unpaired Student t test. Categorical data were compared using Fisher exact test. Spearman rank correlation was used to determine associations between postoperative level of cortisol and other clinical variables. P < .05 were considered statistically significant. All statistical tests were two-tailed.
Results
A total of 54 neonates underwent CPB during the study period. Of these, a total level of serum cortisol was obtained from 41 patients on admission to the CICU, who are included in this analysis. The majority of our study population comprised patients undergoing either an NP (n = 22) or ASO (n = 13). Other patient characteristics are found in Table 1 . The median serum cortisol concentration was 12 µg/dL (interquartile range: 5.2-27.4). Levels of cortisol were <5 µg/dL in nine patients (22%), <10 µg/dL in 18 (44%) patients, and <20 µg/dL in 27 (66%) patients. Nine patients had a second serum cortisol assay (due to escalating inotrope requirement) at a median time of 11 hours (range 8-13) after CICU admission. In these nine patients, the median admission cortisol was 11.4 µg/dL versus subsequent cortisol of 7.6 µg/dL (P = .28).
Patient Characteristics a
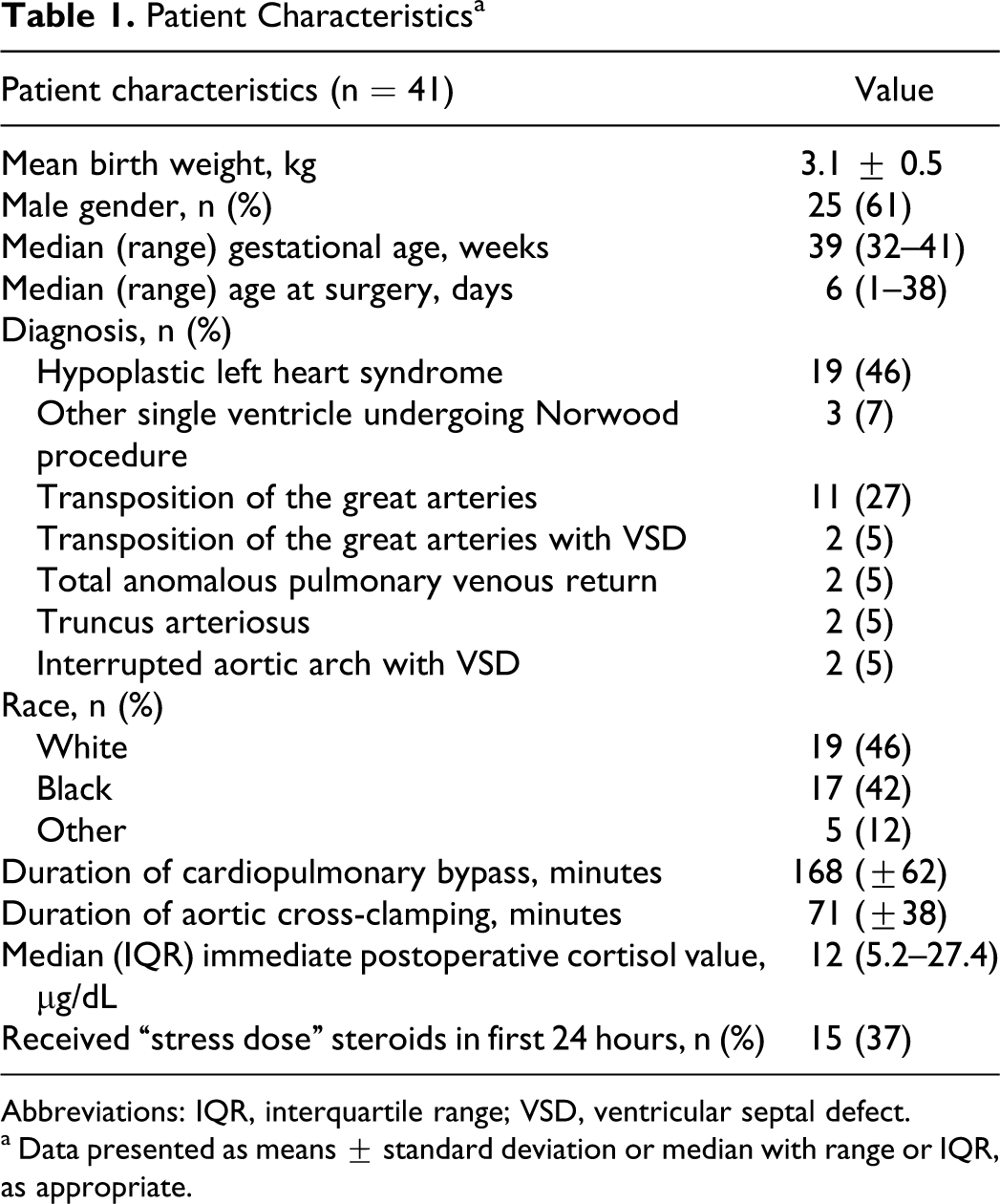
Abbreviations: IQR, interquartile range; VSD, ventricular septal defect.
a Data presented as means ± standard deviation or median with range or IQR, as appropriate.
Immediate postoperative levels of serum cortisol correlated positively with maximum lactate, maximum Sa
Relationship Between Clinical Variables and Immediate Postoperative Serum Cortisol Level (n = 41)
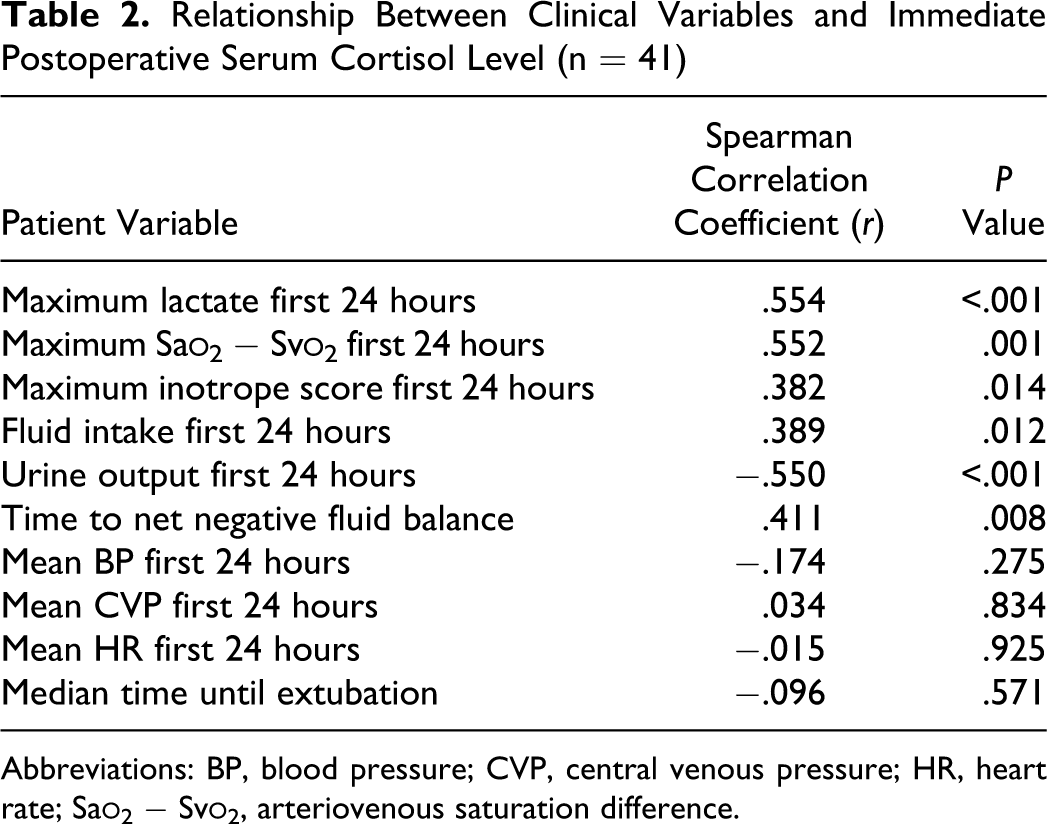
Abbreviations: BP, blood pressure; CVP, central venous pressure; HR, heart rate; Sa
When compared with the low cortisol group, patients with cortisol ≥10 µg/dL had higher maximum lactate (11.8 ± 4.4 mmol/L vs 9.1 ± 3.4 mmol/L, P = .04) and maximum Sa
Comparison of Clinical Variables Between Patients with Cortisol <10 and ≥10 µg/dL a
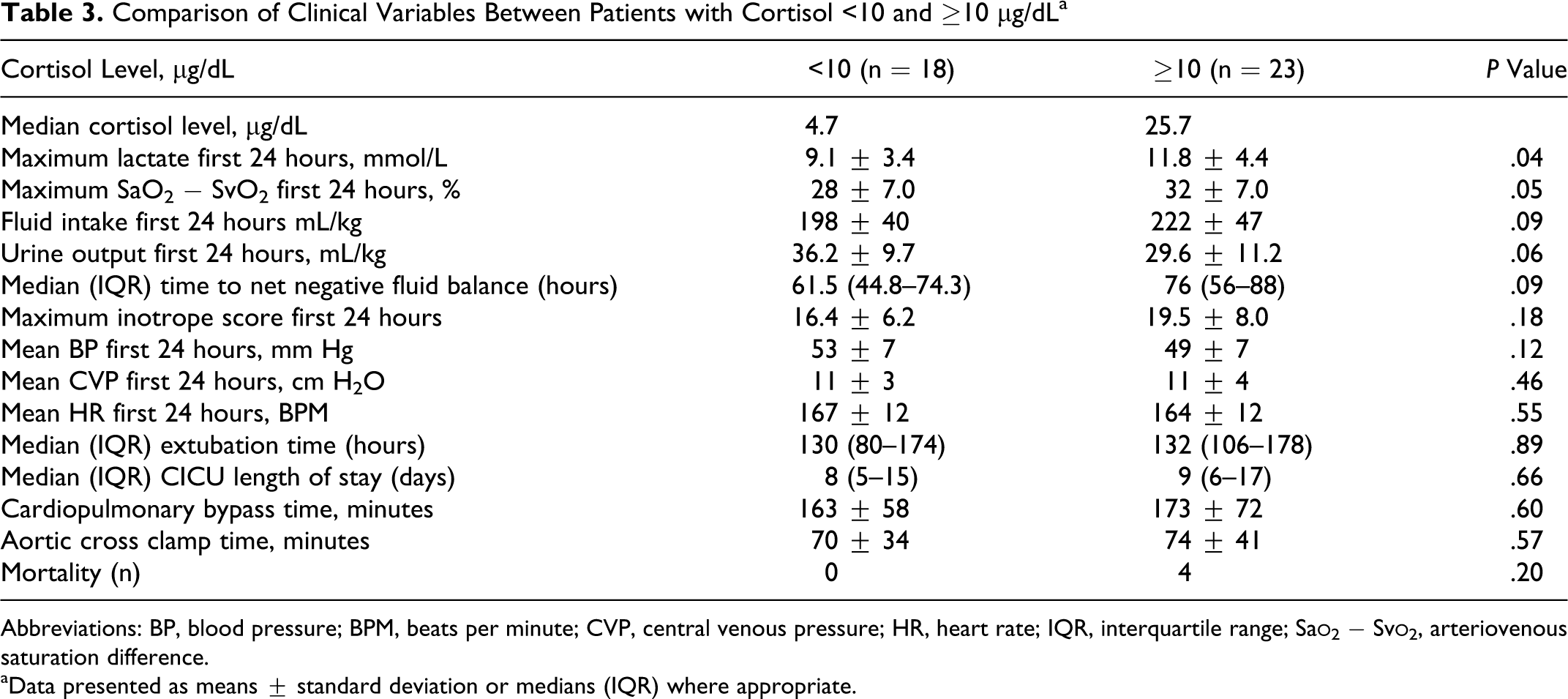
Abbreviations: BP, blood pressure; BPM, beats per minute; CVP, central venous pressure; HR, heart rate; IQR, interquartile range; Sa
aData presented as means ± standard deviation or medians (IQR) where appropriate.
There were trends toward greater fluid intake and lower UOP in patients with cortisol ≥10 µg/dL along with longer time to negative fluid balance. There was no statistically significant difference between the two groups with respect to mean maximum IS, mean blood pressure (BP), mean HR, and median time to extubation. Duration of aortic cross clamp and CPB times was not significantly different (Table 3).
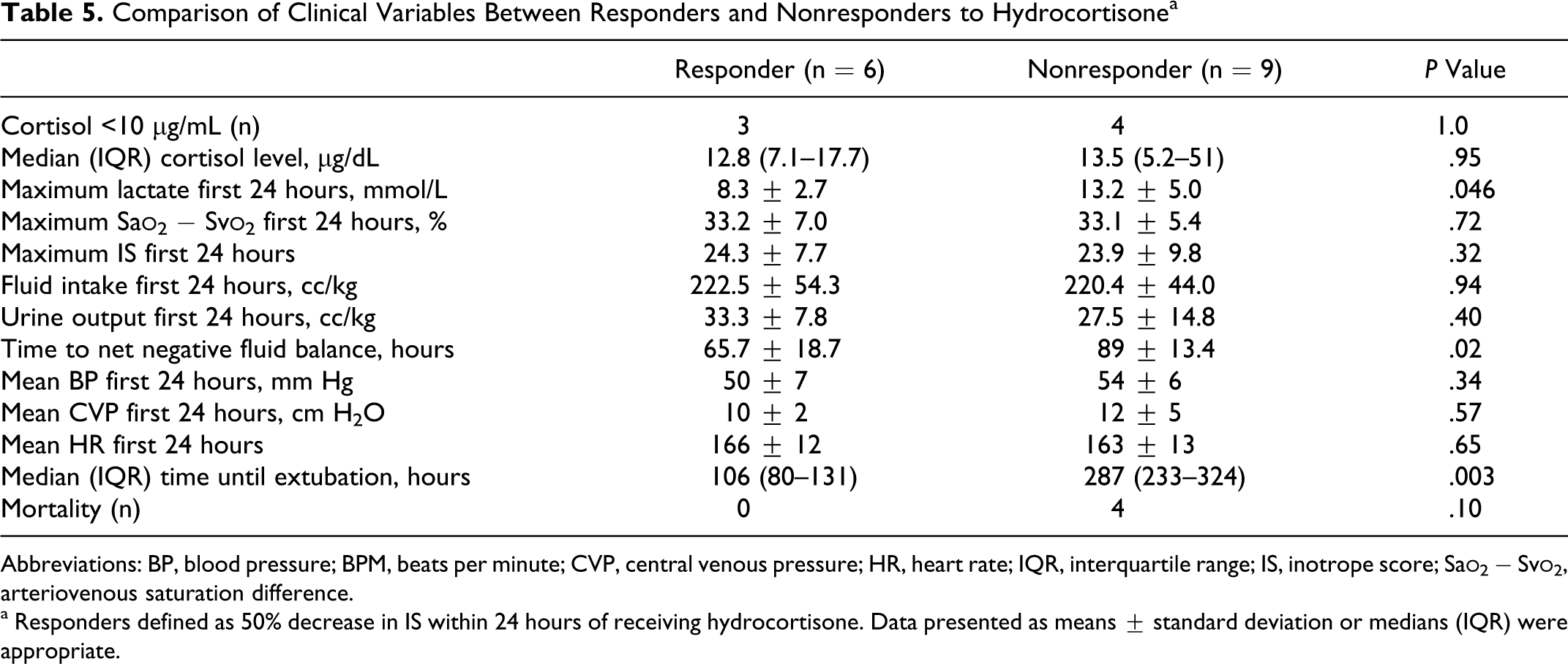
Fifteen patients received HC within 24 hours after CICU admission. The mean IS in patients receiving HC was 24 ± 8.8 versus 14.7 ± 3.3 for those who did not receive HC (P < .001). Of the 15 patients receiving HC, six (40%) had a positive hemodynamic response, with a reduction in mean IS from 23.7 ± 9 to 9.1 ± 4.4 (P < .001) at 24 hours. Three of seven patients (43%) with cortisol <10 µg/dL responded, while three of eight patients (38%) with cortisol ≥10 µg/dL responded (P = 1.0; Table 4 ). There was no statistical difference in the median level of cortisol between responders and nonresponders. Responders had a significantly lower maximum lactate and achieved negative fluid balance and extubation faster than nonresponders (Table 5 ).
Steroid Responsiveness Between Cortisol <10 µg/dL and ≥10 µg/dL
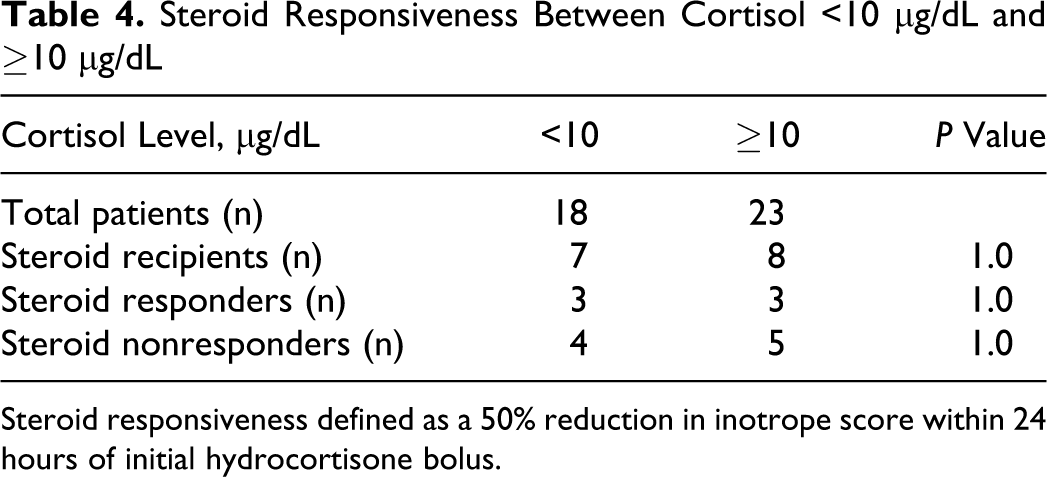
Steroid responsiveness defined as a 50% reduction in inotrope score within 24 hours of initial hydrocortisone bolus.
Comparison of Clinical Variables Between Responders and Nonresponders to Hydrocortisone a
Abbreviations: BP, blood pressure; BPM, beats per minute; CVP, central venous pressure; HR, heart rate; IQR, interquartile range; IS, inotrope score; Sa
a Responders defined as 50% decrease in IS within 24 hours of receiving hydrocortisone. Data presented as means ± standard deviation or medians (IQR) were appropriate.
Four patients (9.8%) died in this study. Three died after NP (POD 11, 23, and 26) and one died after repair of truncus arteriosus (POD 9). Median cortisol of nonsurvivors was 63 µg/dL (range 30-125). All nonsurvivors received steroids but did not respond.
Discussion
Primary Observations of Study
We hypothesized that low levels of cortisol (<10 µg/dL) would be associated with higher inotropic support, a greater degree of fluid resuscitation, and a favorable hemodynamic response to exogenous steroids. Our findings are contrary to this hypothesis and current CICU practice. Within our population, elevated level of serum cortisol was associated with clinical markers of ongoing low cardiac output syndrome (LCOS) and hypoperfusion, such as elevated lactate, increased Sa
Low Cortisol Not Reflective of CIRCI
Critical illness and severe stress trigger a hormonal cascade that leads the anterior pituitary to secrete ACTH, which in turn induces the production and release of cortisol from the adrenal gland. Cortisol is an essential component of the stress response, playing a role in immunomodulation, maintenance of venous and arteriolar tone, limitation of capillary leak, and maintenance of cardiovascular responsiveness to circulating catecholamines.
In a recent consensus statement on the diagnosis and management of CIRCI, Marik et al 1 proposed that adrenal insufficiency during critical illness should be defined as a random cortisol <10 µg/dL or by a Δ cortisol <9 µg/dL after an ACTH stimulation test. A low or low-normal serum cortisol has been suggested as a potential surrogate for CIRCI in children after CPB. 11 Low random cortisol is frequently observed in children with septic shock and has been associated with worse outcomes in some studies.12,13
However, traditional cortisol thresholds used in adults and children may be inappropriate for neonates. Two recent studies of neonates undergoing CPB surgery reveal that postoperative “normal” cortisol values range from 2.2 to 5 µg/dL.7,14 These seemingly low cortisol values were not associated with poor outcomes. Another study of 35 critically ill term and late-preterm neonates without heart disease found a median cortisol of 4.6 µg/dL, without an obvious relationship to severity of illness. 15 Our work supports these findings, as low cortisol was not associated with worse outcomes. Furthermore, as cortisol failed to predict steroid responsiveness, our findings support the consensus statement recommendation that the decision to administer steroids should be based on clinical grounds (ie, catecholamine-refractory shock) and not on the basis of adrenal function testing. 1
Cortisol Positively Correlated With Illness Severity
In our study, higher cortisol was correlated with postoperative surrogates for increased severity of illness, such as higher lactate concentration peak and Sa
Four other recent studies also evaluated the relationship between total serum cortisol and clinical outcomes in the postoperative period with conflicting results.5,6,14,16 A prospective observational study in children younger than 3 months old found that the elevation in cortisol was associated with both higher inotrope requirements at 48 hours and with prolonged mechanical ventilation. 16 However, two prospective, observational studies failed to find any relationship between postoperative levels of serum cortisol and IS 5 or fluid intake, IS, and mechanical ventilation duration. 6 A study of neonatal patients undergoing CPB reported no relationship between serum cortisol and most clinical variables, including lactate, fluid balance, and IS, but did demonstrate an association between levels of cortisol and both higher atrial filling pressure and lower cardiac index. 14 It is noteworthy that the neonates who died in our study had four of the five highest recorded levels of cortisol. This observation is consistent with a number of studies in septic shock in which elevated cortisol concentration is correlated with higher morbidity and mortality.17,18
Glucocorticoid Resistance
The positive correlation between the levels of cortisol and markers of oxygen transport imbalance and LCOS in our study may simply reflect that severely ill children mount a more robust stress response. However, an alternative explanation is that these patients are in fact more severely ill and require higher circulating levels of cortisol due to the inhibition of cortisol or its receptors (glucocorticoid resistance). 19 With glucocorticoid resistance, a patient may require cortisol concentrations higher than the typically accepted normal range to adequately cope with stress. Glucocorticoid resistance may account for the observation that many patients with normal cortisol concentrations appear to benefit from exogenous steroids. Along these lines, it is noteworthy that half of the HC responders in our study had levels of cortisol above the median. Unfortunately, clinically useful surrogates of glucocorticoid resistance are not currently available. Further work should be done to examine the role of glucocorticoid resistance after cardiac surgery in neonates. We speculate that interpretation of cortisol concentration in context with indicators of glucocorticoid resistance may eventually enable more rational use of steroids for patients after CPB.
Steroid Supplementation
Much of the support for CIRCI as a contributor to LCOS after congenital heart surgery originates from small clinical studies that demonstrate benefit of exogenous steroid supplementation on various short-term clinical and laboratory outcomes (ie, decreased inotrope requirements, decreased fluid requirements, improved respiratory function, and decreased inflammatory cytokines).3,4,20 It is not clear whether benefit from exogenous steroids suggests dysregulation of the hypothalamic–pituitary axis or whether these are merely alternative effects of steroids. In addition to their anti-inflammatory effects, corticosteroids have been shown to upregulate adrenergic receptors necessary for the maintenance of cardiac contractility and vascular tone. 21 Furthermore, steroids have poorly defined hemodynamic consequences via nongenomic mechanisms that occur rapidly, with effects occurring as early as seconds to minutes after administration. 22 A recent retrospective study of pediatric CICU patients who received steroids for hypotension found that 41% had hemodynamic improvement, yet no predictors of benefit from exogenous steroids were identified. 20 Similarly, in our study, 40% of patients who received steroids had a positive hemodynamic response. Nonresponders tended to exhibit markers of increased severity of illness but did not have consistently lower levels of cortisol. In fact, a patient was just as likely to respond to exogenous steroids whether postoperative cortisol was low or high. Thus, for many patients, a positive hemodynamic response to exogenous steroid replacement may be unrelated to their adrenal function. That 40% of patients responded to steroids is interesting and accords well with other studies,3,4 but naturally raises the question of whether these patients would have equally improved in its absence. Answers to this question must wait for a prospective clinical trial.
All four patients who died in our study received stress dose steroids in the first 24 hours but did not have a hemodynamic benefit. This is consistent with two studies involving similar populations that also noted lack of steroid responsiveness in their nonsurvivors.3,20 The combination of high levels of cortisol with steroid nonresponsiveness was found in all nonsurvivors in our study, supporting these findings as having potential prognostic value.
Study Limitations
This study is limited by its retrospective single-center design. We cannot discount clinician management variability regarding volume and inotrope management in the immediate postoperative period. Another limitation of our study is the small sample size and, in particular, the small number of patients receiving steroids. Despite our ability to associate cortisol concentration with several laboratory markers of LCOS and/or hypoperfusion, the small sample size prohibits us from drawing conclusions about more important clinical outcomes, such as length of mechanical ventilation, length of CICU stay, and mortality. Our findings may not be applicable to other centers due to differences in preoperative and intraoperative steroid therapy, ultrafiltration methods, exposures to medications that may affect steroid metabolism, timing and method of cortisol assays, and patient ages. Despite a transition to protocolized care in our CICU, some neonates undergoing operations during the study period could not be included because a cortisol assay was not performed. Although these omissions were random, selection bias may have affected our results. Finally, we did not perform ACTH stimulation tests, although there is no consensus on the validity or utility of such testing.
Conclusions
In light of our data and preexisting studies, we conclude: (1) immediate postoperative serum cortisol concentration is positively correlated with severity of illness, (2) low levels of cortisol in neonates after CPB do not predict worse clinical outcomes, (3) the use of an absolute cortisol concentration threshold in isolation to guide steroid therapy in neonates after cardiac surgery is unjustified, (4) elevated cortisol concentration coupled with nonresponsiveness to HC therapy in the first 24 hours after CPB may be associated with unfavorable outcomes, and (5) HC administration should be considered in neonates with fluid and catecholamine resistant shock following CPB.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presented at the Eighth International Conference of The Pediatric Cardiac Intensive Care Society, Miami Beach, USA; December 8–11, 2010.