
Abstract
We describe rare cases of common arterial trunk (truncus arteriosus communis) with unbalanced atrioventricular septal defect, left ventricular hypoplasia, and restrictive ventricular septal defect. The embryology, hemodynamics, and the clinical implications of this complex combination are discussed.
Keywords
Introduction
Common arterial trunk ([CAT]; truncus arteriosus communis) is described as the origin of a single great artery from the base of the heart giving rise to coronary, systemic, and pulmonary arterial circulations. 1 The phenotypic spectrum of CAT is quite variable and has led to considerable debate among morphologists regarding its embryological origin. We report 2 cases of rare variants of CAT with functionally single ventricle and discuss the embryology and clinical implications.
Case Details
Case I
A 6-month-old male infant from the Fiji Islands was referred to us with cyanosis and a heart defect with increased pulmonary flow. The infant weighing 3200 g was in severe respiratory distress due to cardiac failure and concurrent lung infection. Clinical examination revealed poor nutritional status, deep cyanosis, and features of cardiac failure. Chest radiography revealed cardiomegaly, absence of a main pulmonary artery segment, right aortic arch, pulmonary plethora, and collapse with consolidation of the left lung.
Echocardiography showed atrial situs solitus, levocardia, a large ostium primum atrial septal defect, common atrioventricular valve, and
In view of the unusual and complex nature of the defect, a computed tomographic (CT) angiogram was carried out which confirmed the echocardiographic findings (Figures 1 and 2 ). There was also evidence of extensive collapse consolidation of both lungs in the CT. Bilateral pulmonary artery banding was contemplated as a possible first-stage palliation in view of the estimate of very high risk and potentially grave long-term prognosis. Meanwhile, the infant succumbed with rapid worsening of respiratory status due to refractory heart failure, severe pneumonia, and sepsis.
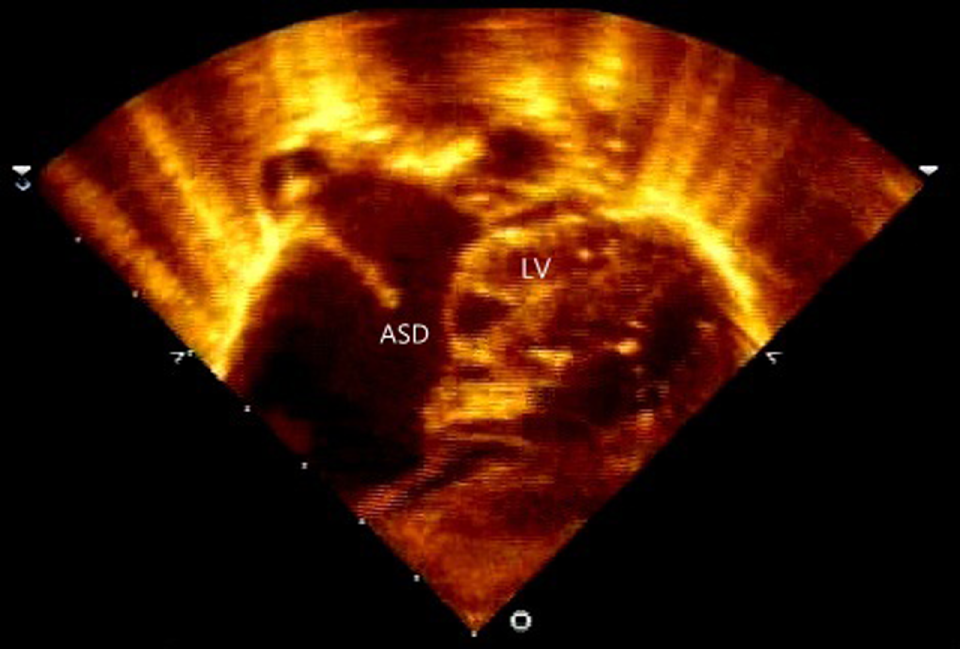
Case 1—Echocardiogram: subcostal long axis view showing large primum atrial septal defect (ASD) and hypoplastic left ventricle (LV).
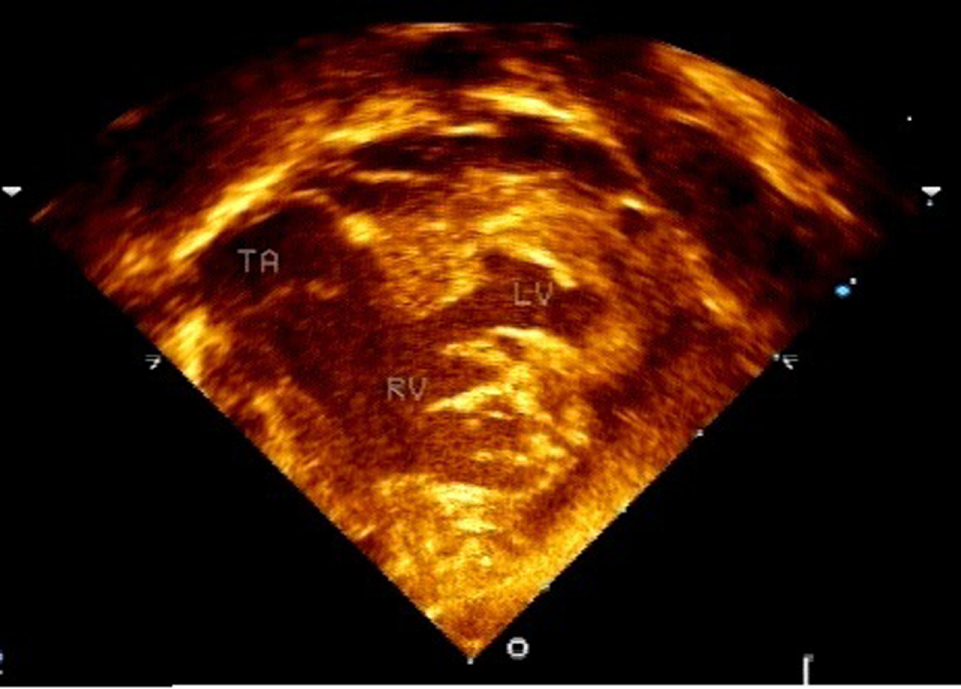
Case1—Echocardiogram: modified subcostal view showing hypoplastic left ventricle (LV) with small ventricular septal defect and truncus arteriosus (TA) arising from the right ventricle (RV).
Case II
Almost a month following the previous case, we received a 5-month-old infant from Uganda with a similar anomaly. On examination, the infant was failing to thrive with weight of 2900 g and signs of congestive cardiac failure and cyanosis. Echocardiography revealed atrial situs solitus, levocardia, restrictive ostium primum atrial septal defect, unbalanced atrioventricular septal defect with hypoplastic left ventricle, and moderate common atrioventricular valve regurgitation (Figures 3 and 4 ). The ventricular component of the atrioventricular septal defect was restrictive, with a small anterior muscular extension. The common trunk was arising from the right ventricle and it gave rise to both the aorta and main pulmonary artery (Collet and Edwards Type I) with no truncal valve stenosis or regurgitation and with unrestricted pulmonary blood flow and pulmonary arterial hypertension. The aortic arch was left-sided and there were bilateral superior caval veins.
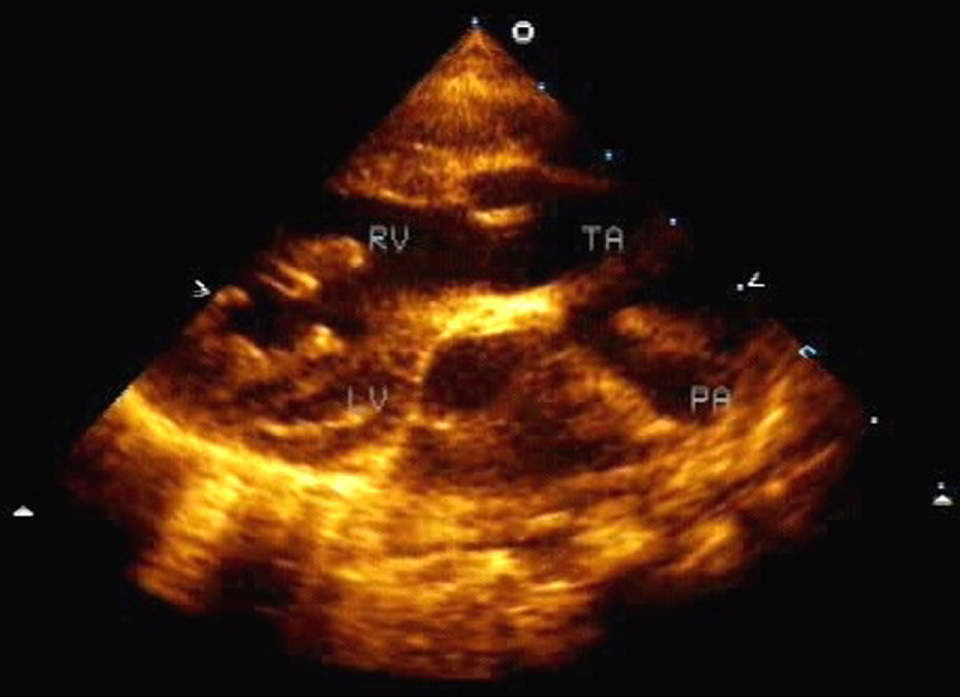
Case2—Echocardiogram: parasternal long axis (modified) view showing hypoplastic left ventricle (LV), truncus arteriosus (TA) arising from right ventricle (RV). Pulmonary arterial trunk (PA) is arising from truncus arteriosus and gives rise to right and left pulmonary arteries (Collet Edward Type I).
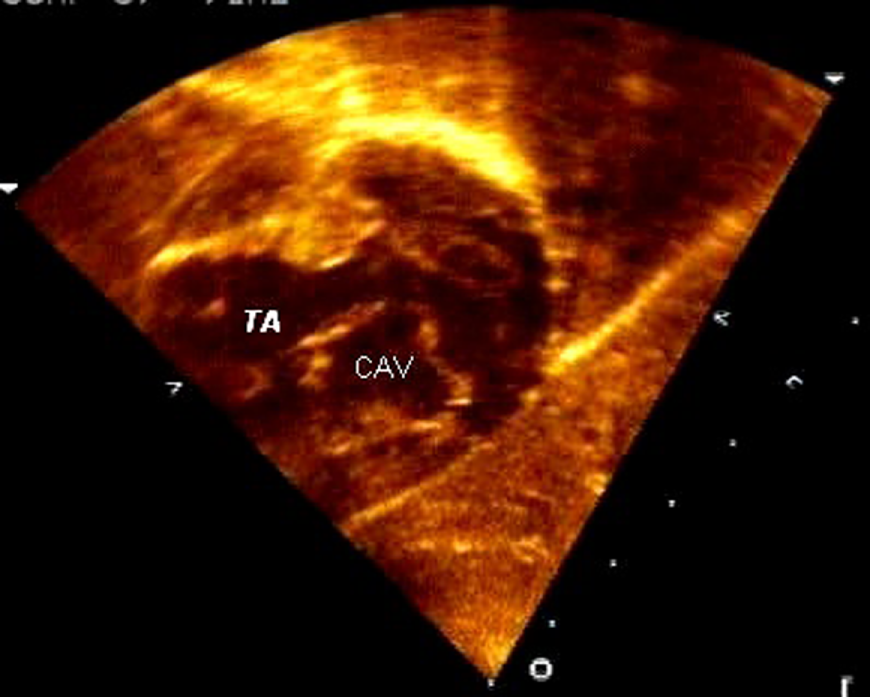
Case2—Echocardiogram: modified subcostal view showing common atrioventricular valve (CAV) in cross-sectional view of unbalanced atrioventricular septal defect and truncus arteriosus (TA) arising from right ventricle.
As the patient required a single-ventricle palliation and had features of severe pulmonary arterial hypertension, the surgery was deferred and medical management was continued.
Discussion
Among the rare variants, CAT with intact ventricular septum and single-ventricle physiology has raised considerable interest regarding the embryological aspects of the condition. The embryological basis of CAT is thought to be failure of septation of the embryonic conotruncus. This has been attributed to decreased population of mesenchymal cells derived from the neural crest over the region of the arch. Carr and colleagues 2 proposed the theory that CAT represents a spectrum of defective septation of aorticopulmonary, truncal, and infundibular septum. They described that relatively normal formation of infundibular septum in the absence of aorticopulmonary and truncal septation can lead to CAT without subtruncal ventricular septal defect (VSD).
The presence of subtruncal conus with origin of the CAT entirely over the right ventricle which has been observed in some cases of CAT has suggested a similarity between those cases and hearts with double outlet right ventricle (DORV) or transposition. 3 In 1 case report, Murdison and colleagues 4 explained the defect as a combination of truncus with no defect in conal septum as well as persistence of subtruncal conus that resulted in loss of atrioventricular to semilunar valve continuity and the appearance of CAT entirely from right ventricle.
Furthermore, the association of CAT with mitral valve and left ventricular hypoplasia has been postulated to be a combination of developmental defects. Michelfelder and colleagues 5 described a case of CAT with hypoplastic left heart as a possible variant of DORV with intact septum that leads to mitral and left ventricular hypoplasia, together with additional failure of truncal and aorticopulmonary septation leading to associated truncus arteriosus communis.
Our infants (cases I and II) present similar rare variants of CAT with almost intact ventricular septum and single-ventricle physiology. The unique features in these infants were the presence in each of an atrioventricular septal defect in the setting of a CAT arising from right ventricle. The morphology in these infants represents a constellation of embryological aberrations including defective development of the aortopulmonary, truncal, conal, and the atrioventricular septum with persistence of subtruncal conal septum. This combination of CAT variant with endocardial cushion defect (or atrioventricular septal defect) has not been reported earlier.
The current cases represent additional rare anatomic variants of CAT with single-ventricular physiology and unrestrictive pulmonary blood flow. Successful management of these patients would require early first-stage palliation to control pulmonary blood flow in order to prevent the chronic effects of increased pulmonary blood flow on pulmonary arteries and chronic volume overloading of the ventricle.
Aspects of the embryology, hemodynamics, and clinical profile of these rare variants of CAT are unique and differ considerably from the common varieties of CAT. Awareness of these facts is essential as there is a need for early referral and neonatal palliation in order to maximize the possibility of a successful outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.