
Abstract
An eight-year-old child presented with congestive heart failure, blurred vision, and unexplained constitutional symptoms. An echocardiogram demonstrated a giant left atrial mass that obstructed the mitral valve inflow. After excision of the myxoma, the patient had an uneventful recovery.
Introduction
Primary intracardiac tumors, such as myxomas, rhabdomyomas, and teratomas, are uncommon in the pediatric population with an incidence of 0.2%. 1,2 Patients with atrial myxomas may present a variety of symptoms related to the size and location of the tumor. The majority of the patients would experience one or more of a triad of symptoms. These include atrioventricular valve obstruction, systemic embolization, and constitutional symptoms. 3,4 However, early diagnosis may be challenging because of nonspecific symptoms ranging from congestive heart failure to neurological deficits. Therefore, cardiac myxomas are often misdiagnosed.
Case Report
An eight-year-old patient presented with a two-month history of worsening fatigue, shortness of breath, nocturnal fever, weight loss, anemia, and intermittent episodes of blurred vision. Abdominal ultrasound was performed because of abdominal pain and incidentally showed a giant left atrial mass. The patient was then transferred to our center for further evaluation and management. Physical examination revealed stable vital signs with mild retractions. Cardiac auscultation included a regular heart rhythm with normal S1S2. A grade 2/6 holosystolic murmur was best heard at the apex and radiated to the left axilla with an early diastolic rumble. Ophthalmologic and neurological findings were normal.
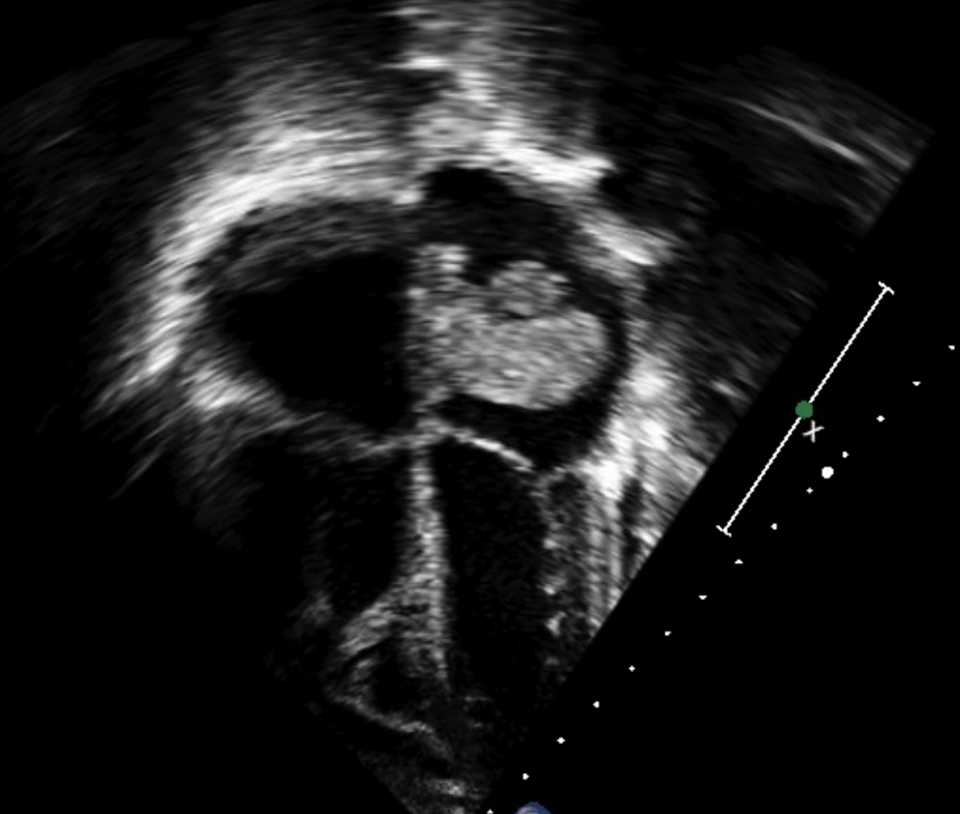
A two-dimensional echocardiography study demonstrated a pedunculated left atrial mass measuring 5.5 × 2.4 cm in size and originating from the atrial septum (Figures 1 –4). The mass prolapsed into the mitral valve annulus during diastole, resulting in inflow obstruction with a peak Doppler pressure gradient of 40 mm Hg and a mean pressure gradient of 23 mm Hg. A moderate mitral valve regurgitation with dilated left atrium was noted. Moderate tricuspid valve regurgitation with a peak pressure gradient of 72 mm Hg was noted, suggesting a moderate degree of pulmonary hypertension associated with diminished right ventricular function.

Preoperative apical four-chamber view. Large left atrial tumor prolapsing into the left ventricle during diastole. Left atrial tumor measured 5.5 × 2.4 cm.
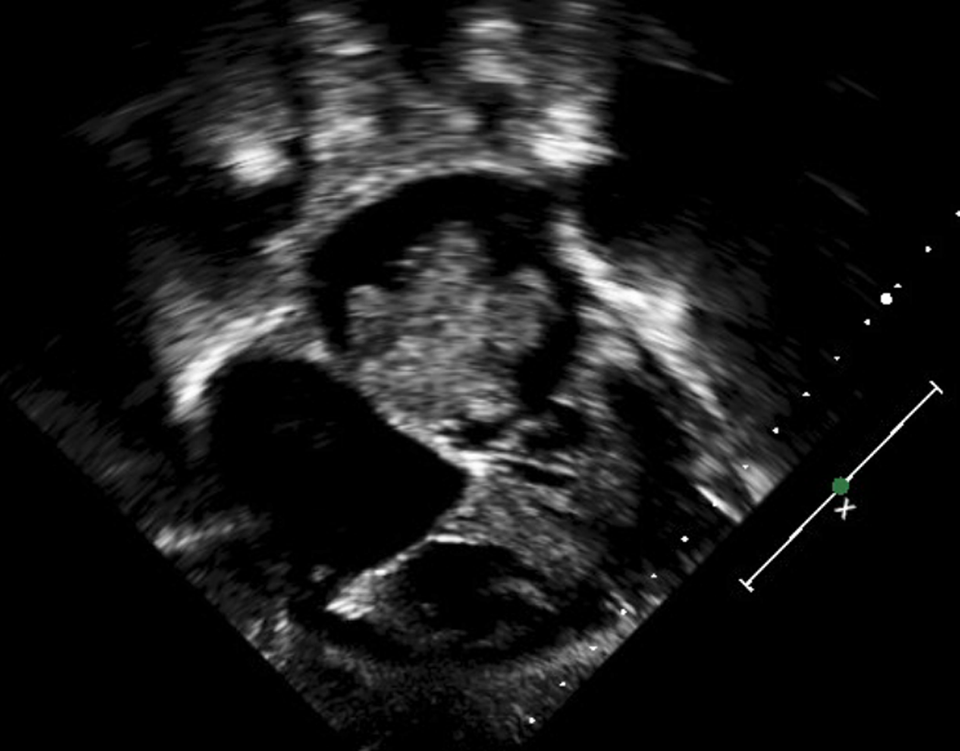
Preoperative apical four-chamber view. Large left atrial tumor attached to the interatrial septum.
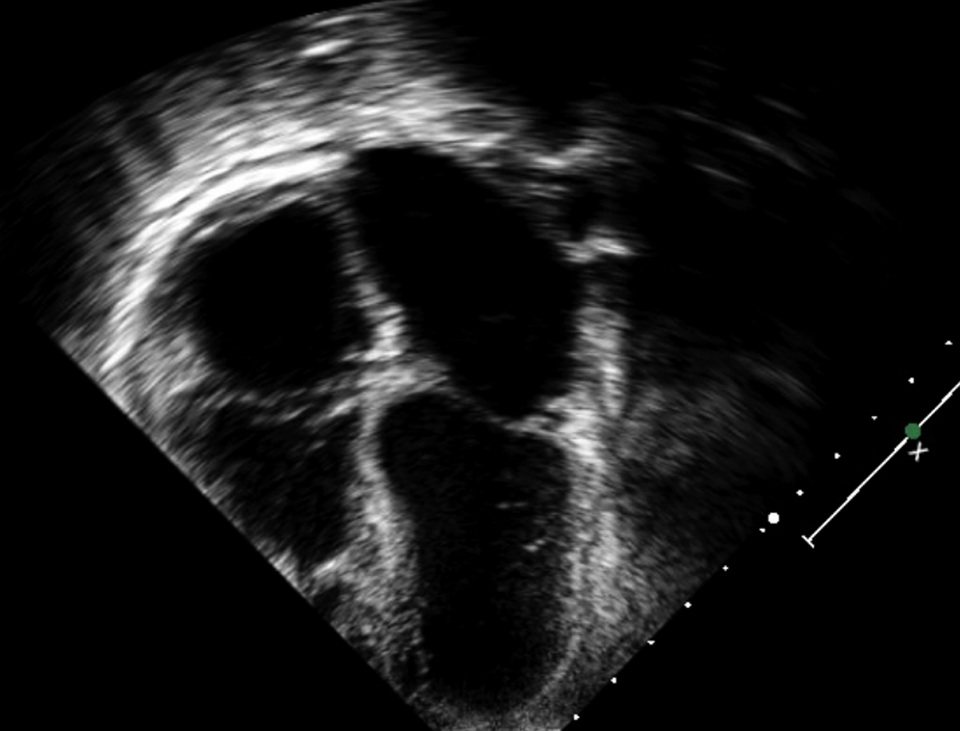
Preoperative coronal subcostal view. Large left atrial tumor with irregular borders.
Postoperative apical four-chamber view. No residual cardiac tumor. Dilated left atrium and trivial pericardial effusion.
Preoperative magnetic resonance imaging (MRI) study of the brain demonstrated multiple emboli in the frontal area (Figure 5). Through a median sternotomy approach, cardiopulmonary bypass was instituted using aortic and bicaval cannulation. After cardioplegic arrest was achieved, the right atrium was opened toward the right upper pulmonary vein. The atrial septum was incised, starting at the fossa ovalis, revealing a large mass, which was extremely fragile and fragmented. The tumor was entirely resected with a full thickness portion of the interatrial septum where the tumor neck was attached. The mitral valve was examined and found to be competent. The defect in the atrial septum was closed using a piece of bovine pericardium. The atrial free wall was closed and the patient weaned from cardiopulmonary bypass without difficulty. Histological examination revealed myxomatous tumor. Postoperative echocardiography showed no residual left atrial mass, intact atrial septum, and mild mitral regurgitation.
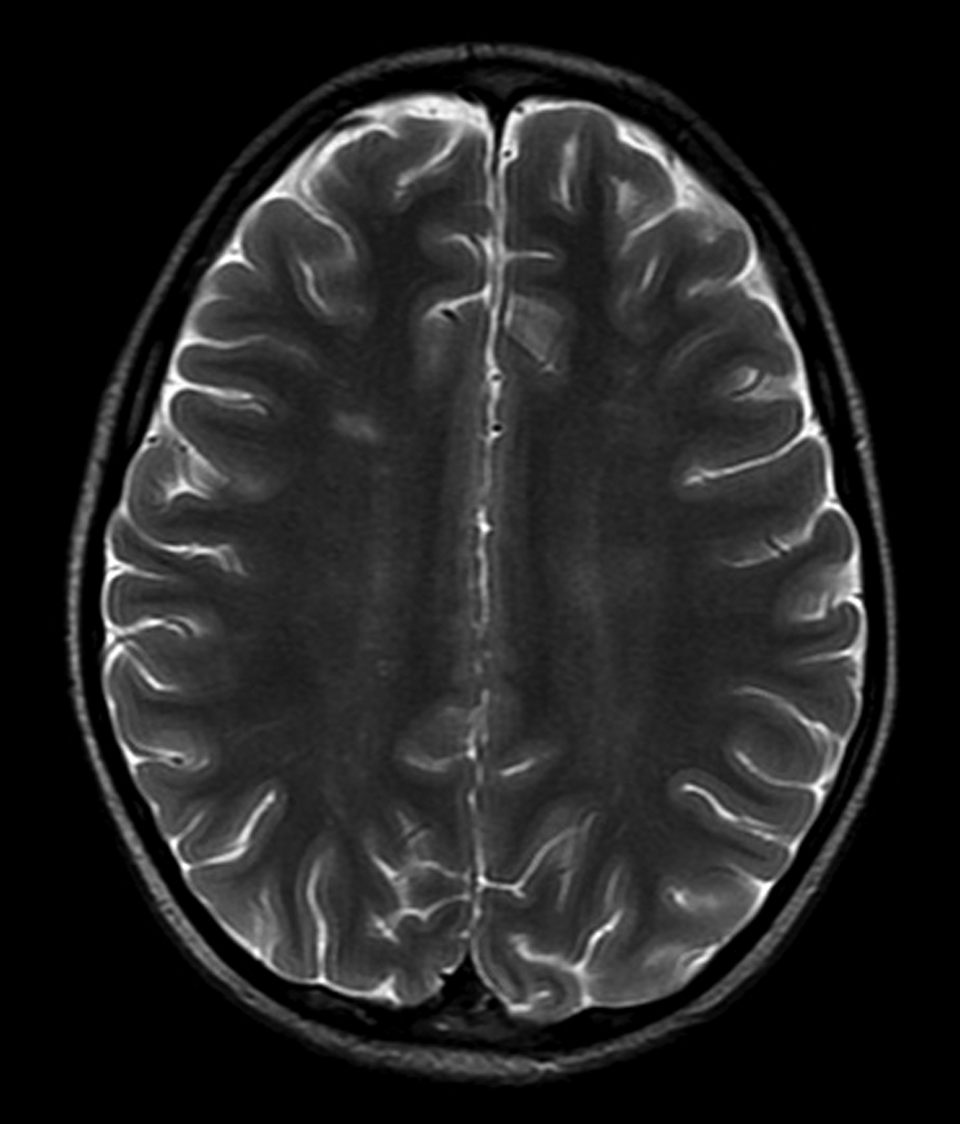
T2-weighted contrast magnetic resonance imaging (MRI) of brain showing 8 mm, white matter lesion in the frontal area.
Discussion
Atrial myxoma is a benign tumor that is rarely seen in the pediatric age group. The literature has only a few case reports of it in children between 1 and 17 years of age. More common in the left atrium, the tumor originates from mesenchymal cells typically located in the fossa ovalis. 1,2 Atrial myxoma primarily occurs in a sporadic fashion. Less than 10% of the cases are associated with autosomal dominant inheritance. 3
Although the clinical spectrum can be wide, the majority of the patients present with one or more of the triad of symptoms known as Goodwin triad. 4 These include embolic phenomena, inflow chamber obstruction, and vague constitutional symptoms.
Clinical manifestations secondary to inflow obstruction are most common, occurring in more than 50% of the patients with atrial myxomas. They include fatigue, dyspnea, and orthopnea when the tumor is located in the left atrium and systemic edema when it is in the right atrium.
Embolic phenomena occur in 30% to 40% of the patients and involve the central nervous system, kidneys, coronary arteries, and extremities. The embolic fragments usually consists of myxomatous tissue and may also be related to thrombus dislodged from the surface of the myxoma. 5 Ischemic strokes and vision defects secondary to occipital lobe involvement have also been reported. 6 Embolic phenomena may also mimic infective endocarditis (splinter hemorrhage, Janeway lesions, conjunctival petechiae, and Osler nodules). 7 The clinical presentation may vary from hemodynamic compromise to neurological deficits and sudden death. 8 ,9
Nonspecific constitutional symptoms, such as fever, weight loss, and rheumatic pain, are commonly associated with atrial myxomas. Abnormal laboratory findings include anemia, thrombocytopenia, elevated erythrocyte sedimentation rate, and high serum levels of interleukin 6. These nonspecific and often vague symptoms result in late diagnosis in many cases. 10 ,11
Cardiac myxomas are typically diagnosed by echocardiography. Computed tomography and MRI can help determine the location and the extent of the tumor. 12,13 The MRI of brain would be a valuable modality to determine the presence of central nervous system pathology, especially if neurological signs and symptoms are present.
A high degree of clinical awareness would help to obtain a timely diagnosis. Urgent surgical resection of the tumor can prevent potential emboli and devastating brain damage. Although resection of atrial myxoma results in rapid resolution of symptoms, long-term follow-up is required in young patients because of a reported recurrence rate of 5% to 7%.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.