
Abstract
Anomalous origin of right subclavian artery arising from the descending aorta is known as “arteria lusoria.” The diagnosis in asymptomatic children is usually the by-product of other symptomatic-associated anomalies, such as aortic coarctation. We describe a case of an eight-year-old boy with juxtaductal aortic coarctation and rare origin of the arteria lusoria proximal to the aortic coarctation. The anomalous arteria lusoria was used as a flap to repair the aortic coarctation. To the authors’ knowledge, this is the first reported application of lusoria flap in a young child (not newborn) with ductal aortic coarctation.
Introduction
Anomalous origin of the right subclavian artery arising from the descending aorta is known as “arteria lusoria.” Arteria lusoria is associated with aortic coarctation in 0.5% to 2% of the cases. 1 In these patients, thanks to the investigations of the suspected aortic coarctation, the presence of anomalous right subclavian artery can be noticed. Usually, the arteria lusoria takes its origin distally from the coarctation. 2,3 In the case described, the arteria lusoria took its origin proximal to the coarctation. The arteria lusoria was subsequently used as a flap to repair the coarctation, analogous to a subclavian flap.
Patient
Physical examination of this asymptomatic eight-year-old child (134 cm and 22 kg) revealed reduced femoral pulse intensity by palpation and leg blood pressure lower than arm, suspected for aortic coarctation. A transthoracic echocardiography confirmed the aortic coarctation and showed a dubious origin of the right subclavian artery. Cardiovascular magnetic resonance imaging confirmed the aortic coarctation and showed a common origin of both the carotid arteries and separated origin of the left subclavian artery. The right subclavian artery originated directly distal to the left subclavian artery and proximal to the severe juxtaductal aortic coarctation (coarctation diameter 6-7 mm; Figure 1). The arteria lusoria crossed the midline posterior to the esophagus. Extensive collateral vessels were detected, particularly from both internal mammary arteries.

Cardiovascular magnetic resonance, three-dimensional (3D) reconstruction. Arteria lusoria originated distal to left subclavian artery and proximal to the ductal aortic coarctation.
Surgery of the aortic coarctation was planned, while a surgical intervention of the arteria lusoria was initially not planned because of the absence of symptoms.
Surgical Findings
The operation was performed via a left posterolateral thoracotomy through the fourth intercostal space and maintaining normothermia. The arteria lusoria was identified directly cranial to the juxtaductal aortic coarctation (Figure 2A). The diameter of the arteria lusoria was 9 mm, while that of left subclavian artery was 7 mm. The ligamentum arteriosum was doubly ligated and divided. Along the entire length of the coarctation and along the descending aorta, large collateral vessels were dissected free and divided into two in order to mobilize the aorta. However, because of the arteria lusoria and the abundant collateral vessels, the possible mobilization of the aorta proved to be insufficient. Moreover, because of patient’s size the distance between aortic arch and descending aorta was wide (2.5 cm). For these two reasons, an end-to-end anastomosis was not feasible. It was decided to use the arteria lusoria as a flap to repair the aortic coarctation because of its advantageous position and to preclude future dysphagia. The arteria lusoria was dissected up to the right side of the vertebral column in order to obtain a long subclavian flap for the coarctation repair and at the same time prevent possible future compression of the mediastinal organs. In order to verify whether the right-arm perfusion could be preserved without the contribution of the arteria lusoria, first a test was made by clamping the arteria lusoria using near-infrared spectroscopy (NIRS) on the right arm. No difference in NIRS on the right arm was noticed after the clamping of the arteria lusoria. Moreover, the invasive blood pressure line in the right radial artery showed no difference in the medium blood pressure after the clamping of the arteria lusoria, although the pulsatility largely disappeared; the blood pressure was 75/55 mm Hg before and 80/60 mm Hg after the clamping test. The arteria lusoria was then divided as distally as possible and closed with a polypropylene suture line. The proximal portion was then incised in the length of the vessel just as in a subclavian flap operation, carrying the incision through the ductal coarctation into the descending aorta (Figure 2B). The “lusoria flap” was turned down and sutured on the aorta with 5-0 polypropylene (Figure 2C). After the clamps were released, the noninvasive mean blood pressure on the left leg was not different from that on the right arm (75 and 70 mm Hg, respectively). The palpation revealed normal femoral pulse intensity. The clamp time was 15 minutes.
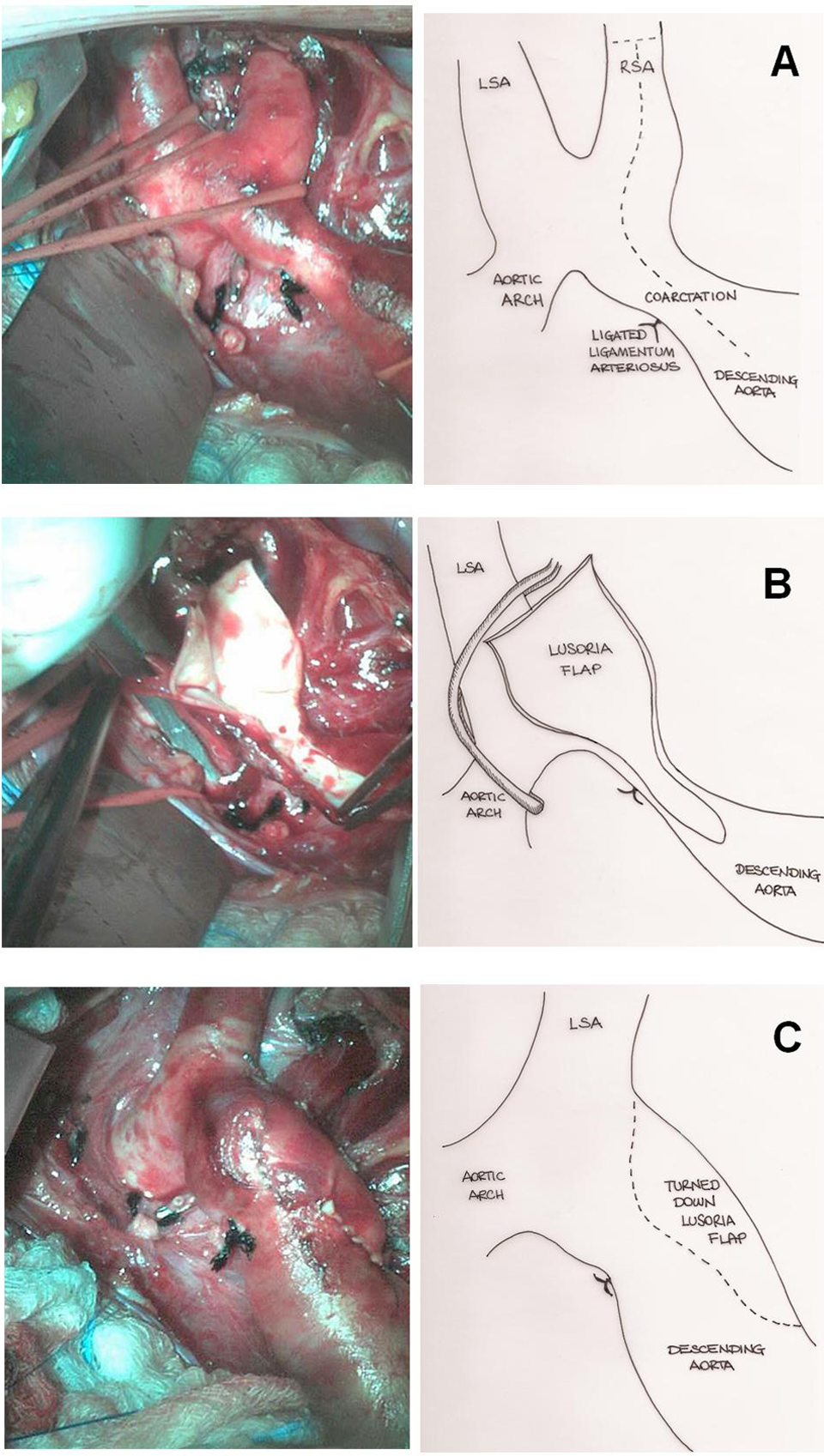
A, Aberrant RSA distal from LSA and directly cranial to the ductal aortic coarctation. The ligamentum arteriosum was already dissected. Dotted line shows the line of incision of the proximal RSA into the descending aorta. B, After clamping LSA and aortic arch, the lusoria flap is prepared to be turned down. C, Final result of the sutured lusoria flap on the aorta. Aortic diameter remains unvaried along the sutured flap. Dotted line shows the sutured flap. LSA, left subclavian artery; RSA, right subclavian artery.
In the postoperative phase, the blood pressure measured on the right arm was not different from that on the left arm or on the legs. The range of blood pressure was around 70 to 80 mm Hg, hence under the 90th percentile for the patient’s age.
The postoperative course was complicated by left-sided chylothorax, treated with surgical reoperation and medium-chain triglycerides diet with the resolution of the clinical picture. On postoperative day 42, the patient was discharged home in good clinical condition. At nine-month follow-up, there was no difference between arm and leg blood pressure, and the range of blood pressure remained below 90th percentile for the patient’s age.
Comment
The pseudonym arteria lusoria takes its origin from the dysphagia experienced by adult patients due to compression of the retroesophageal course of the right subclavian artery; the Latin expression dysphagia lusus naturae means in fact dysphagia caused by a freak of nature. 4 Only 10% of the patients with arteria lusoria have compressive symptoms such as dysphagia. Atherosclerotic degeneration or fibromuscular dysplasia could make the vessel rigid and noncompliant causing compression of the esophagus. These mechanisms occur in adult age; therefore, children are almost always asymptomatic. The diagnosis in children is often incidental because of concomitant associated anomalies such as aortic arch interruption and aortic coarctation. 1
However, while aortic coarctation and arteria lusoria are known congenital entities, their combination is quite unusual (0.5% to 2% of the patients with aortic coarctation). 1
The treatment of choice for children with aortic coarctation, irrespective of the presence of arteria lusoria, is surgical correction. Among the available surgical options, end-to-end anastomosis and subclavian flap technique are the most frequently used. 5 However, in case of older patients, the amount of collateral vessels adds further difficulty to the dissection and the mobilization of the aorta. Moreover, the arteria lusoria fixes the aortic isthmus in cranial position. This reduced aortic mobility makes an end-to-end anastomosis extremely difficult. 2 For these reasons, the arteria lusoria has been used as flap to repair aortic disease, even in case of complex aortic arch reconstruction. 3,6,7 The arteria lusoria flap has been previously described in cases of postductal aortic coarctation, where the arteria lusoria originated distally to the aortic coarctation. 2,3 A previous report described the arteria lusoria flap technique in a 9-day-old newborn with preductal aortic coarctation. 7
However, to the authors’ knowledge, there are no previous cases of juxtaductal aortic coarctation combined with proximal arteria lusoria, diagnosed and surgically treated in a young child.
The use of the arteria lusoria as a flap allowed treating both anomalies. In fact, through a left posterolateral thoracotomy, it was possible to dissect the arteria lusoria up to the right side of the vertebral column, which presumably will prevent possible symptoms of compression and possible late complications such as aneurysmal degeneration, rupture, or distal embolization in adult age.
In general, a further advantage of a subclavian flap is that autologous tissue has growth potential. 3,6 With the exclusion of end-to-end anastomosis, which was not feasible in this case, the other surgical options for aortic coarctation such as interposition of prosthetic graft or pericardial patch do not provide the same growth potential and are thus unattractive.
A possible disadvantage of the subclavian flap technique in a relatively old child is arm perfusion. In order to prevent any possible complication, we recommend verifying the preservation of arm perfusion by means of NIRS and invasive blood pressure measurement before dividing the arteria lusoria.
In summary, we described the case of an eight-year-old boy with juxtaductal aortic coarctation and arteria lusoria with its origin proximal to the coarctation, in which the arteria lusoria was used as a flap to repair aortic coarctation. The origin of the subclavia lusoria proximal to the aortic coarctation occurs very rarely. 2 Moreover, to the authors’ knowledge, this is the first case in which the lusoria flap has been used in a young child with juxtaductal aortic coarctation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.