
Abstract
Anatomical correction of transposition of the great arteries (TGA) with an intramural coronary artery is associated with high risk of coronary complications such as vessel injury and stenosis. Here, we report on a case of left main coronary artery stenting in a neonate with single coronary artery after repair for TGA.
Introduction
Arterial switch operation (ASO) has become the standard of treatment for neonates with transposition of the great arteries (TGA) because of good outcomes and low mortality rates. The precise transfer of the coronary arteries is the key to successful surgery. However, after ASO, complications may occur in cases of anomalous origin of the coronary arteries, single coronary artery, or intramural arterial course. 1,2
Case Report
A two-day-old patient weighing 4.3 kg with diagnoses of TGA, patent foramen ovale (PFO), and patent ductus arteriosus (PDA), was admitted to our clinic. On admission, the patient was in poor condition. He was kept on mechanical ventilation support, and his oxygen saturation was 70%. Prostaglandin E1 infusion (4 ng/kg/minute) was initiated immediately. Echocardiography results confirmed TGA, a left ventricular ejection fraction (LVEF) of 77%, left ventricular end-diastolic volume index of 35 mL/m2, PFO of 0.5 cm, and PDA of 0.3 cm. Single coronary artery anatomy was not detected on preoperative echocardiography.
An emergency balloon atrioseptostomy was performed to stabilize the patient, and ASO was performed on the second day. An intramural course of the left coronary artery (LCA) was noted during the operation prior to coronary mobilization (Figure 1). During mobilization, the LCA trunk was injured 2 mm from the ostium, consisting of a linear artery wall rupture 2 mm in length. To avoid stenosis, plasty of the coronary artery was performed at the injured area using a patch from the native aortic wall. An aortocoronary flap technique was used to transfer the common origin of the coronary arteries to the neoaorta (Figure 2). The cross-clamp time was 62 minutes. Transesophageal echocardiography after weaning from cardiopulmonary bypass (CPB) showed a slightly reduced LVEF (65%) and no signs of regional ventricular contractility disorders.
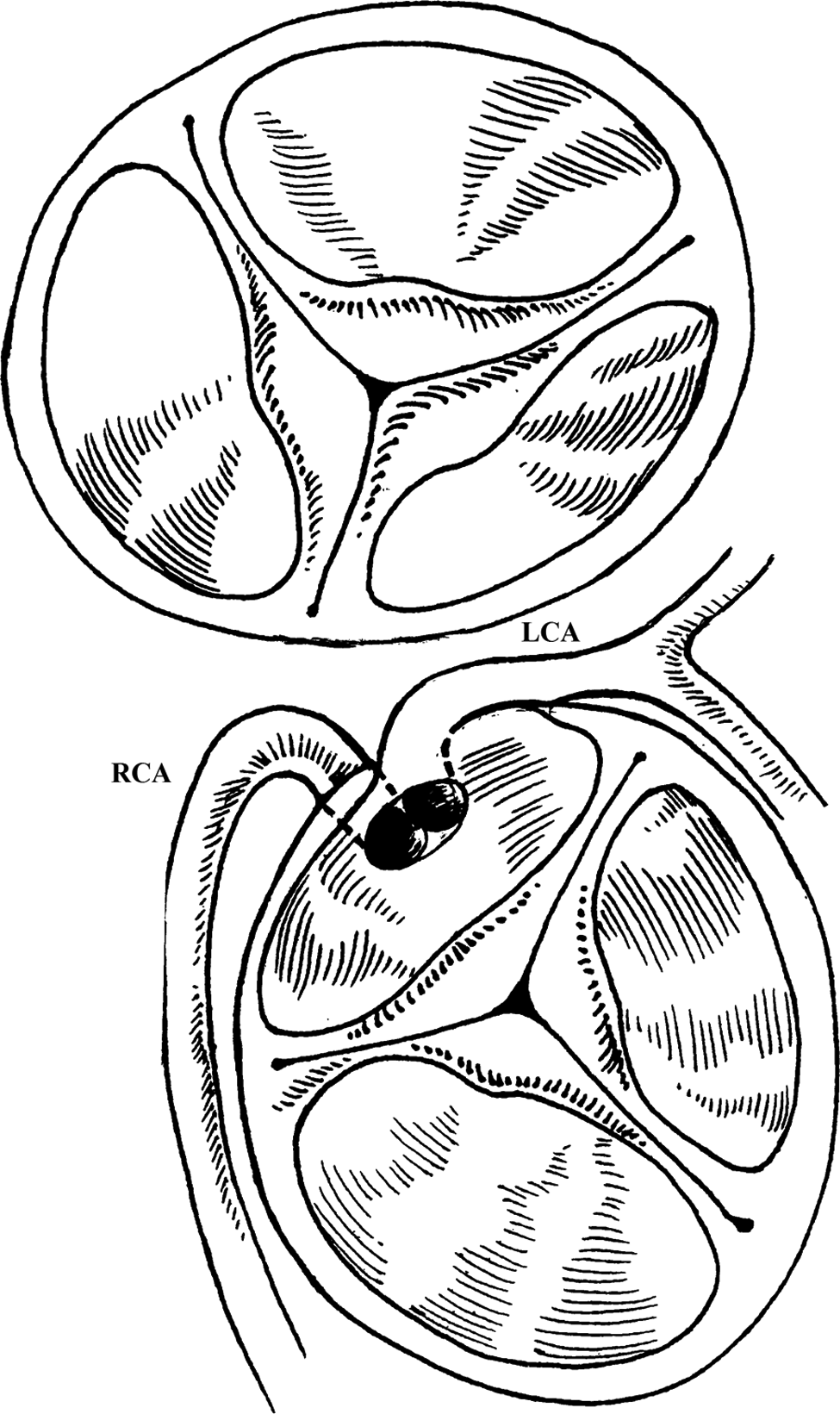
Coronary artery anatomy. LCA indicates left coronary artery; RCA, right coronary artery.
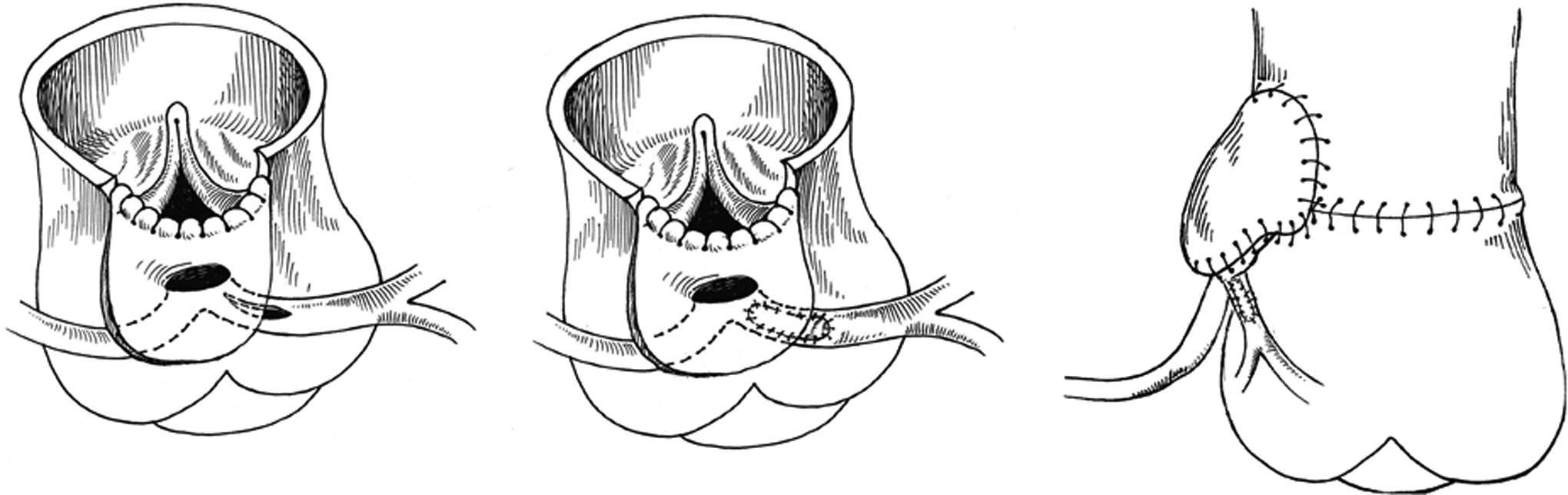
Left coronary artery plasty and aortocoronary flap technique.
The patient was transferred to the intensive care unit (ICU) with an open chest and inotropic support (epinephrine, 0.03 μg/kg/minute) in stable condition. After three hours, sudden hemodynamic collapse occurred; an electrocardiogram showed ST-segment elevation and a wide QRS complex. The patient was immediately transferred to the operating room and underwent emergency coronary artery inspection. There was no visible external compression of the transferred and repaired LCA. Cardiopulmonary bypass support was initiated. We could not exclude coronary artery thrombosis, so the surgically reconstructed neopulmonary artery was transected after initiation of bypass. Aortic cross-clamping was initiated, the heart was stopped with antegrade infusion of cardioplegia, and the aorta was opened. Revision of the coronary ostium and repaired portion of the coronary artery was performed, but there was no visible damage or kinking or evidence of coronary artery thrombosis. The LCA branches were inspected using a vessel probe that passed without difficulty. Thereafter the aorta and pulmonary artery were repaired.
Despite the appearance of adequate myocardial perfusion while on bypass, the patient became unstable while being weaned from CPB (blood pressure, 40/35 torr; left atrium pressure [LAP], 28/25 torr; and bradycardia), with inadequate response to inotropic support. Therefore, the patient was placed on venoarterial extracorporeal membrane oxygenation (ECMO) support. Because of the high LAP (25/23 torr), the left atrial vent introduced via the right proximal pulmonary vein was connected to the drainage limb of the ECMO circuit. Echocardiography on ECMO showed an LVEF of 25% to 28% and hypokinesia of the lateral, anterior, and posterior walls of the left ventricle (LV). On the second postoperative day, a creatine kinase (CK) level of 1,790 units/L and CK-MB level of 425 units/L were noted. A low LVEF (35%) and LV wall hypokinesia were observed; therefore, an examination was performed in the cardiac cathetherization laboratory.
Angiography revealed partial occlusion of the LCA trunk up to the site of the previously repaired injury (Figure 3A). Thus, we decided to stent the LCA trunk (Figure 3B). The right common carotid artery was exposed for the insertion of a 6F introducer. The LCA trunk was catheterized using the Guide Catheter AR2 (Boston Scientific International SA, Paris, France). The area of partial occlusion was recanalized using a Guide Wire Pilot 150 (Abbott Vascular, Santa Clara, California). After predilating the stenotic vessel using 1.2 × 12-mm2 and 2.25 × 15-mm2 balloons (Abbott Vascular), we placed an Integrity 3 × 9-mm2 stent (Medtronic, Minneapolis, Minnesota). The stent extended from the left main artery into the left anterior descending coronary artery with the circumflex artery originating proximal to the distal end of the stent. The subsequent angiogram showed restoration of blood flow into the coronary artery branches (Figure 3C) including the circumflex artery. The introducer was removed, and the right common carotid artery was repaired. The patient, who remained on venoarterial ECMO support, was again transferred to the ICU while the chest was still open.
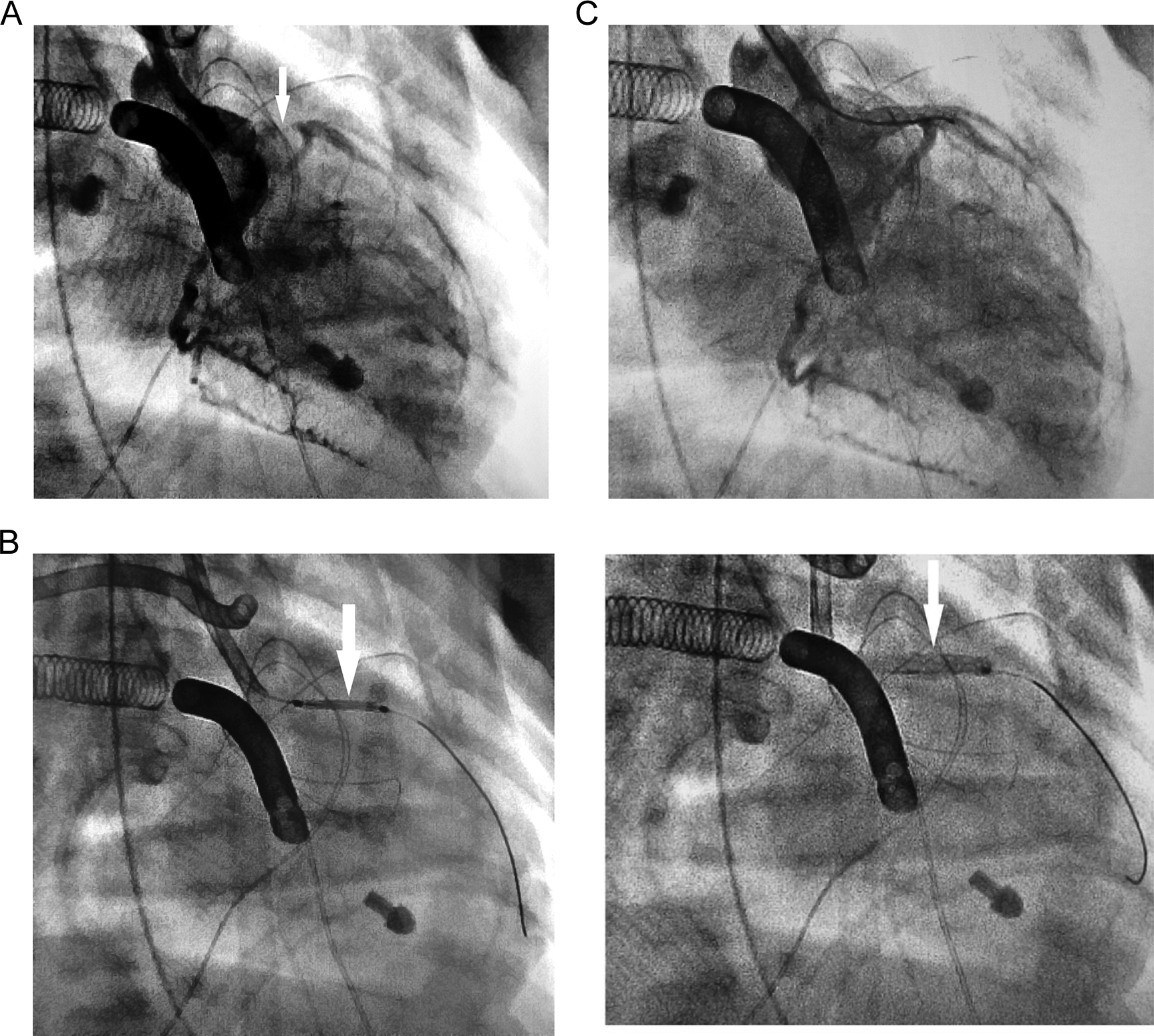
A, Partial occlusion of the left coronary artery (arrow). B, Left coronary artery stenting (arrows). C, Restoration of blood flow in the coronary arteries.
On the fifth postoperative day, echocardiography showed increased LVEF and elimination of the hypokinetic sites in the LV. Postoperative dynamics of the ejection fraction are shown in Figure 4. Because of increased LVEF and after trial weaning from LV venting on the 11th postoperative day, ECMO cannulae were repositioned in the neck vessels, the vent was removed from the left atrium, and the sternotomy wound was closed. The patient’s hemodynamics were generally stable thereafter. On the 19th postoperative day, the patient was weaned from ECMO support while on a low-dose epinephrine infusion (0.001 μg/kg/minute) with LVEF of 51% to 57% by echocardiography.
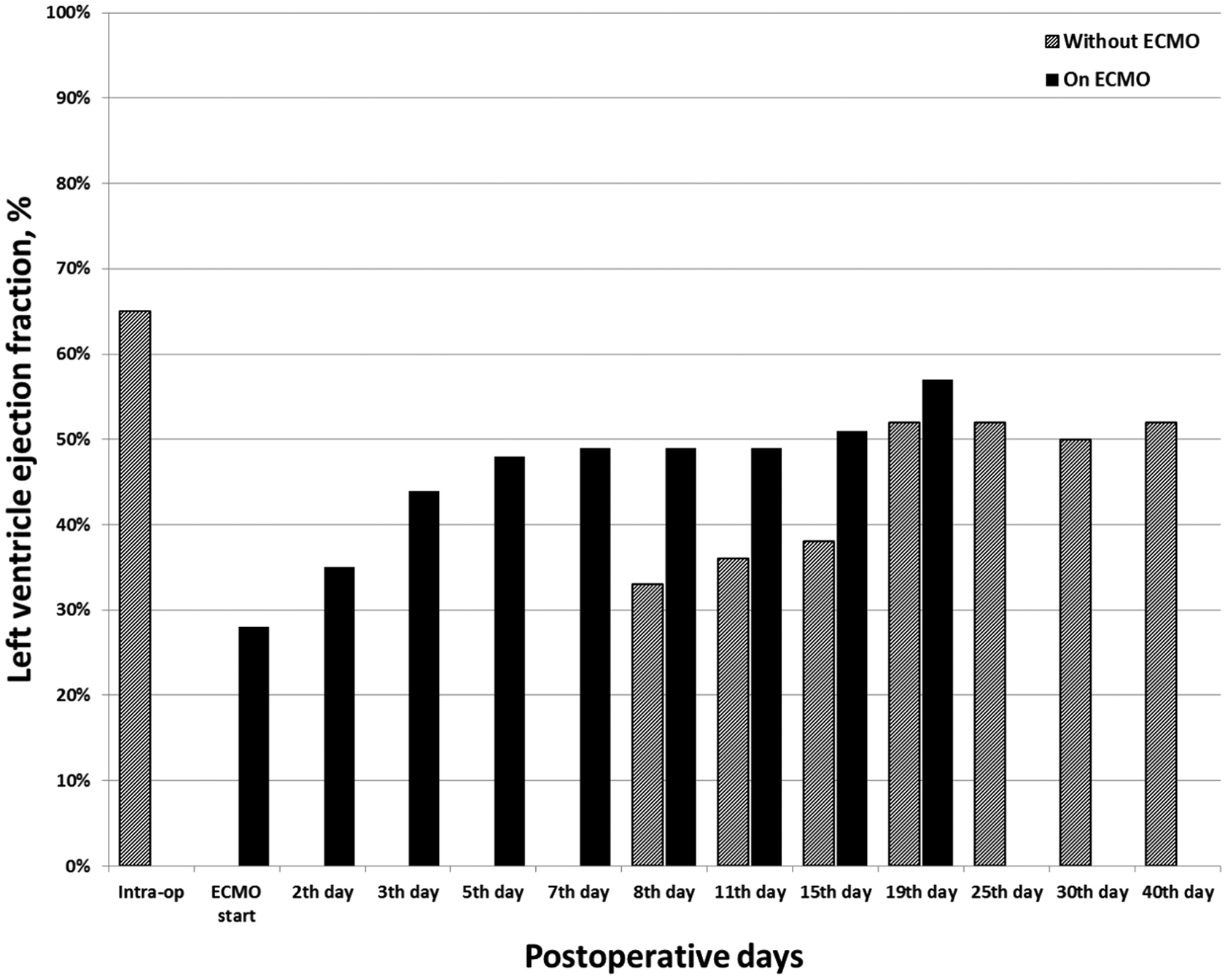
Postoperative dynamics of the left ventricle ejection fraction. ECMO indicates extracorporeal membrane oxygenation.
Unfortunately, the immediate postoperative period after ASO revision and the first several days on ECMO support had been complicated by recurrent bleeding from the chest, which required several mediastinal explorations. The bleeding finally stopped only after ECMO cannulae were repositioned in the neck, and the chest was closed. We believe that the eventual development of mediastinitis, pneumonia, and sepsis (Pseudomonas aeruginosa and Klebsiella pneumonia) was likely sequellae of the early events. Later, during the period following successful separation from ECMO support, the patient’s cardiac condition was relatively stable with an LVEF of 50% to 52%. However, his procalcitonin level increased to ≥10 ng/mL, and leukocyte count decreased to 3.6 × 109. By the 25th postoperative day, the patient had developed renal failure. During the late follow-up period, the patient’s condition deteriorated with signs of sepsis and multiple organ dysfunction. On the 43rd postoperative day, the patient died. Autopsy showed neither gross nor histological signs of myocardial infarction. The ventricles had no signs of hypertrophy or dilation. The coronary arteries were patent, including the stented segment of the LCA and the “jailed” origin of the circumflex artery.
Discussion
Intramural course of a major branch associated with single sinus origin of both coronary arteries in the setting of TGA is a rare abnormality with an incidence of 4.5% to 13.3%. 1,2 Anatomical correction of intramural coronary arteries in TGA is associated with high risk of coronary complications such as vessel injury and stenosis. 3,4 In our patient, separation of the vessels was impossible, because only one coronary ostium was present. The aortocoronary flap technique was used to reposition the coronary artery. The theoretical advantage of this technique is preservation of the in situ geometry of the coronary artery, which should decrease vessel flexion, torsion, and tension. However, this technique may be associated with myocardial ischemia as the child grows because of compression of the coronary artery origin between the great vessels. Metton et al 4 used this technique when the left and right coronary arteries were very close. During the follow-up period, patients who underwent the aortocoronary flap technique were likely to have coronary artery-related complications.
An important consideration in arterial switch surgery is to presume, unless proven otherwise, that any cardiac problem is of coronary artery origin and requires consideration of immediate surgical revision. We used a patch from the aortic wall to repair the injured left coronary trunk. We believe that thrombosis or severe edema of the vessel led to acute coronary syndrome, although perhaps this may have been related to geometric deformation of the repaired left main coronary artery. Performing coronary artery bypass in this complicated case would have been challenging, but an intracoronary stent proved helpful. We inserted a stent in the coronary artery trunk to treat the acute coronary syndrome.
Despite extensive experience with percutaneous coronary intervention procedures in adults, this type of intervention is seldom performed in children because of limitations such as the patient’s age and coronary artery size. Moreover, follow-up outcomes of this procedure remain unclear, especially due to the possible changes in the coronary artery at the repaired segment during growth. However, sporadic cases of stenting in infants with good follow-up outcomes have been described. 5 The stent used in the current study was oversized for this patient’s coronary artery anatomy, with the circumflex artery originating proximal to the distal end of the stent. However, the cells of the stent were large enough that there were no angiographic signs of disturbed circumflex artery flow. Evidence of sufficient blood flow was confirmed by the absence of signs of myocardial infarction on autopsy examination and by histology. Venoarterial ECMO is a commonly used form of extracorporeal life support that provides temporary cardiac support to neonates and infants and is associated with relatively good survival rates. The ECMO is a highly invasive procedure that may be associated with such complications as hemorrhage and infections that significantly increase mortality rates.
Conclusion
Transposition of the great arteries with anomalous origin of the coronary arteries can complicate ASO and may be associated with acute coronary syndrome. Stenting of the damaged vessel is technically possible in neonates. In this case, stenting resulted in recovery of left ventricular ejection fraction (as indicated by echocardiography) and the absence of myocardial infarction signs according to autopsy data.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.