
Abstract
An anomalous origin of the entire coronary circulation from the right pulmonary artery is a very rare congenital malformation. We report on a male newborn presenting with hypoplastic aortic arch and coarctation of the aorta in whom a previously undetected single coronary artery originating from the right pulmonary artery was detected at the time of corrective surgery. The patient underwent a resection of the coarctation with a patch enlargement of the aortic arch and a successful reimplantation of the coronary artery into the aorta.
Keywords
Introduction
An anomalous coronary artery arising from the pulmonary artery is a rare anomaly, with an incidence of 0.01% in the general population. 1 A few cases of a left or a right coronary artery arising from the right pulmonary artery are reported in the literature. 2,3 We describe a rare case of a single coronary artery originating from the right pulmonary artery. To our knowledge, only one similar postmortem case was described in the literature. 4
Case Description
The first child of a 34-year-old mother was born at 39 weeks of gestation with a birth weight of 3230 g. The child was born after an uncomplicated pregnancy by spontaneous vaginal delivery in cephalic presentation. The Apgar scores were 8, 9, and 9 after 1, 5, and 10 minutes, respectively.
Fetal echocardiography at 32 weeks of gestation showed a hypoplastic aortic arch, an aortic coarctation, a bicuspid aortic valve, and multiple atrial septal defects.
The newborn was transferred to our pediatric cardiac intensive care unit and intravenous prostaglandin E1 was commenced immediately. The preoperative echocardiography confirmed the diagnosis: aortic coarctation and hypoplastic aortic arch with a diameter of 5 mm. The coronary arteries were not described.
Surgical correction was scheduled at three days postpartum. The chest was opened through a midline sternotomy and cardiopulmonary bypass was initiated through aortic and bicaval canulation. After cooling down to a core temperature of 20°C, the aorta was clamped and cold crystalloid cardioplegic solution was instituted directly into the ascending aorta. This proved to be difficult and infusion of the solution was somewhat slow but this was thought to be a technical problem due to the small aorta. In the end, the infusion of cardioplegia was abandoned, because the heart was thought to be protected enough with deep hypothermia and total circulatory arrest. The reconstruction of the aorta was performed with a patch of autologous pericardium and the atrial septum was closed with a polytetrafluoroethylene (PTFE) patch. After rewarming and declamping of the aorta, the myocardial function was found to be reduced on transesophageal echocardiography. Inspection of the situs revealed that no coronary arteries were arising from the aorta, but a tiny single coronary artery from the middle part of the right pulmonary artery, at its inferior wall. The aorta was clamped again and the right pulmonary artery was incised longitudinally (Figure 1). The coronary artery was explanted with a button and reinserted into the lateral wall of the ascending aorta. After excision of the button, the pulmonary artery lumen was very small and a PTFE patch was inserted. After a long bypass time, weaning was initially not possible. Under extracorporeal membrane oxygenation (ECMO) support the postoperative period was uncomplicated. Angiography confirmed successful reimplantation of the single coronary artery (Figure 2). The ECMO was weaned after 3 days with stable hemodynamics and a good myocardial function.
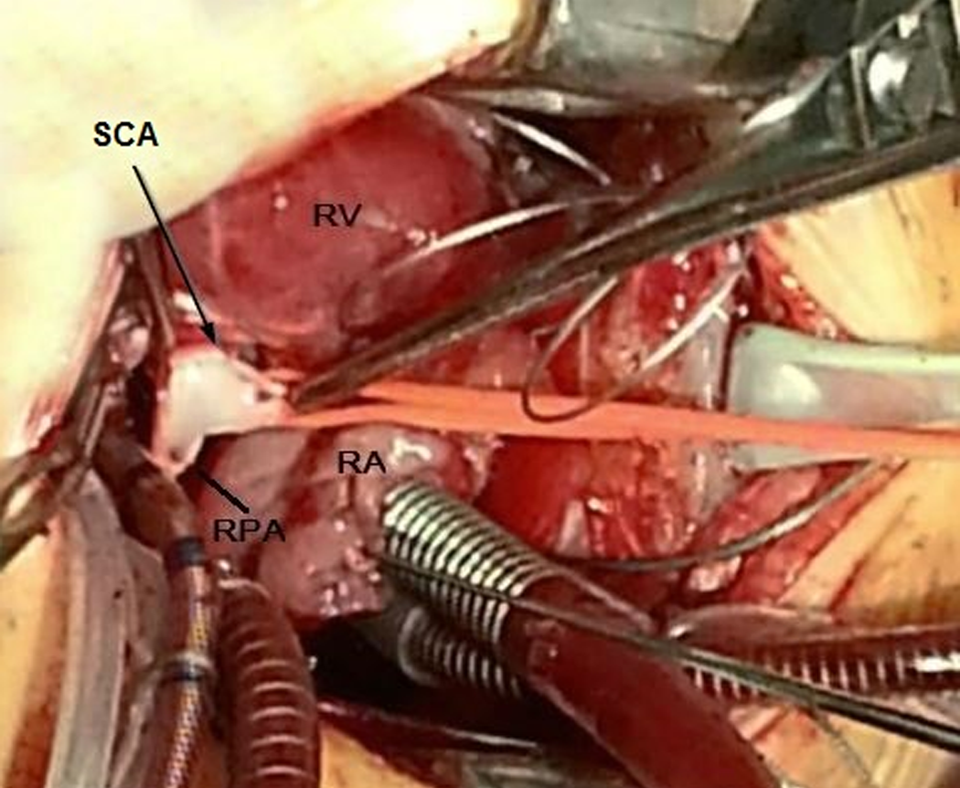
Intraoperative view of the anomalous origin of the single coronary artery originating from the right pulmonary artery. SCA indicates single coronary artery; RV, right ventrical; RA, right atrium; RPA, right pulomnary artery.
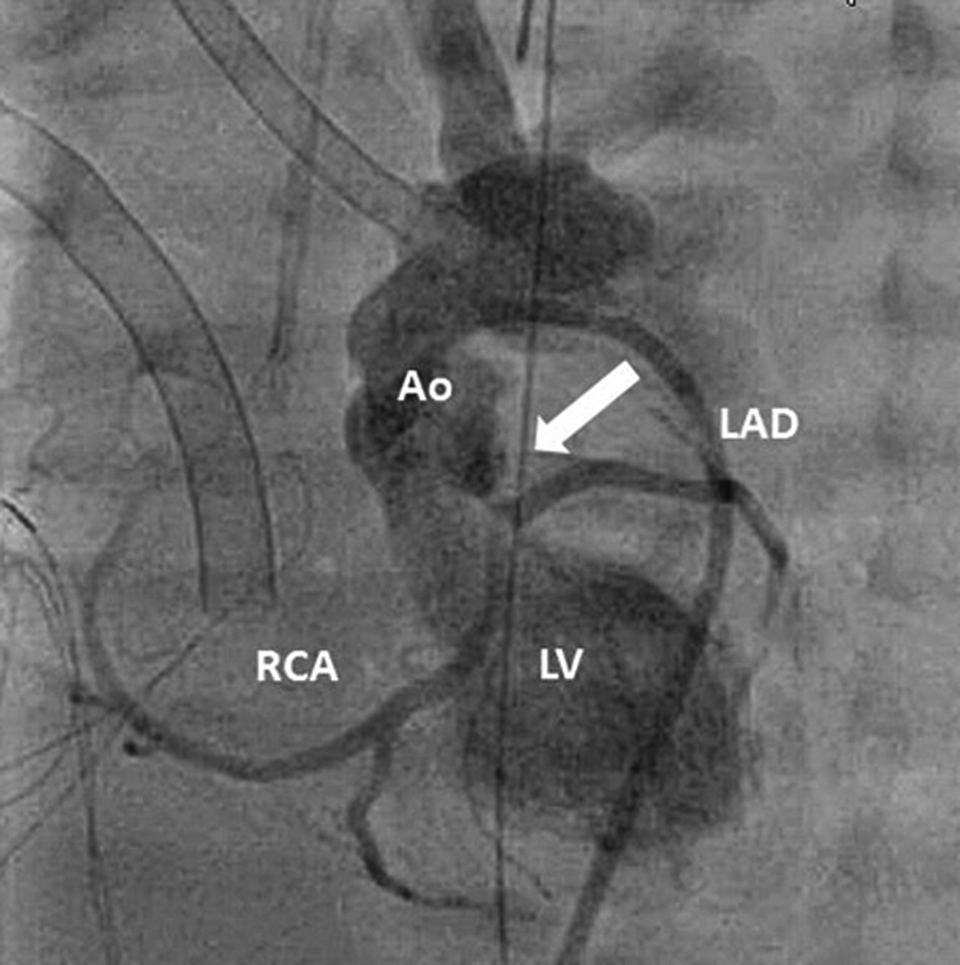
Postoperative angiography showing the successful reimplantation of the single coronary artery into the aorta ascendens. Ao indicates aorta; LAD, left arterior descending artery; LV, left ventricle; RCA, right coronary artery.
On fourth postoperative day, the patient developed acute rhythm disturbances, suddenly required increased inotropic support, and consequently needed cardiopulmonary resuscitation. The ECMO was immediately reinserted and the patient was brought to the catheterization laboratory for angiography. The angiography revealed a thrombotic occlusion of the mid portion of the left arterior descending artery, probably due to a coagulopathy (Figure 3). This development was sudden and unexpected. The patient consequently died from acute myocardial infarction.
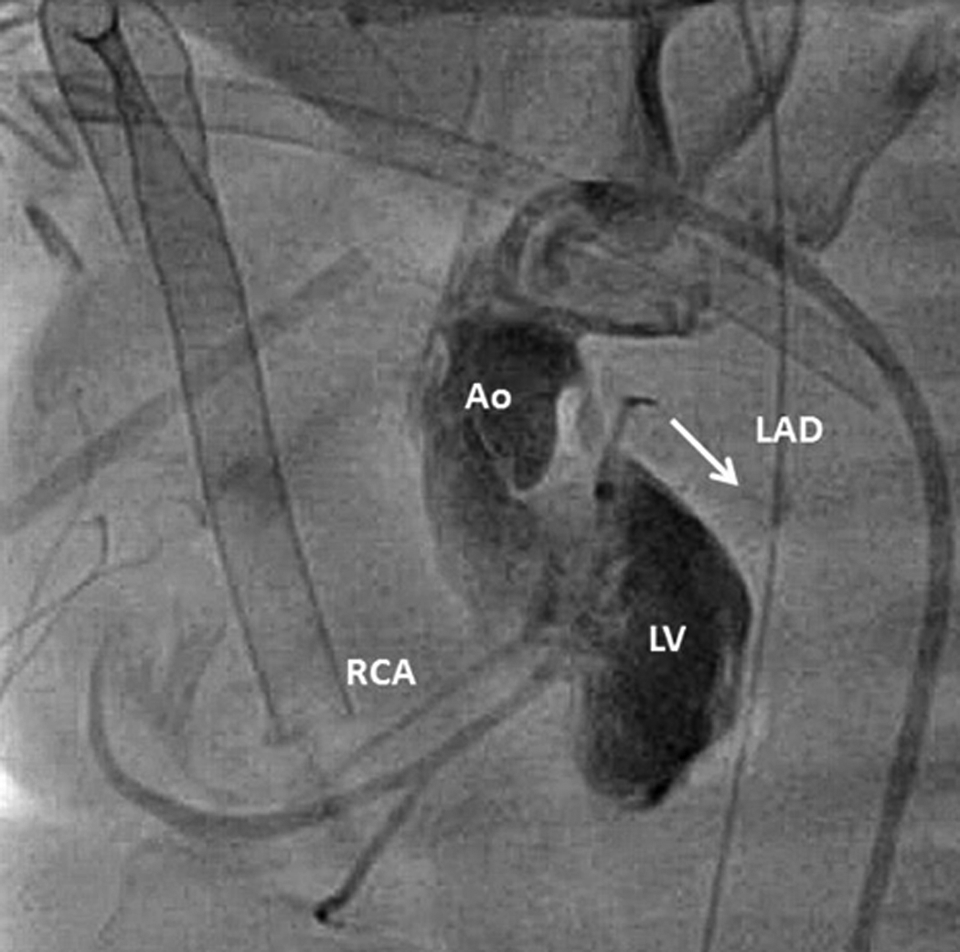
Angiography showing the occlusion of the LAD due to thrombosis. Ao indicates aorta; LAD, left anterior descending artery; LV, left ventricle; RCA, right coronary artery.
Discussion
An anomalous origin of a single coronary artery from the right pulmonary artery has, to our knowledge, only been described once in the literature. 4 It was found in the postmortem of a child with sudden death.
Today, decisions on the surgical management of patients with congenital heart disease are often based on a diagnosis made by echocardiography alone. 5 Our case illustrates that the sole echocardiographic assessment was not sufficient to detect the anomalous coronary pattern. In our opinion, coronaries should always be described preoperatively in echocardiography. If that cannot be achieved, angiography might be advisable.
Although our patient underwent an early and successful reimplantation of the anomalous single coronary artery, a subsequent thrombosis led to a complication. Thrombosis of a coronary artery leading to myocardial infarction in neonates is a rare and life-threatening condition. The suggested treatment consists of inotropes, diuretics, angiotensin-converting enzyme inhibitors or ECMO implantation. 6 The ECMO support may have beneficial effects on myocardial recovery. 7 It is, however, difficult to identify an underlying cause for the infarction in our patient. We think that the cause was a complication due to a coagulopathy.
In conclusion, in complex heart diseases, a rare coronary anomaly can be present. Even if only detected during the heart operation, a successful reimplantation of the coronary artery can be performed. The early diagnosis of an anomalous origin of a coronary artery is advantageous and upon echocardiography inspection of the aortic root is advisable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.