
Abstract
Objective:
Patients who have undergone a previous bidirectional superior cavopulmonary anastomosis and have hypoxemia and anatomy considered unsuitable for the Fontan completion present a difficult subset. We performed common carotid artery-to-internal jugular vein (CCA-IJV) shunt in these patients.
Methods:
Between January 2010 and January 2015, eight patients underwent a CCA-IJV shunt. Their records were analyzed retrospectively.
Results:
There were no early deaths. The baseline arterial saturation prior to the shunt procedure was median 67% (range 60%-72%), which increased to median 83% (range 80%-90%) after the procedure. The preoperative arterial oxygen partial pressure (Pa
Conclusions:
In a selected group of patients who are considered to be unsuitable for completion of Fontan circulation following superior cavopulmonary anastomosis, creation of a CCA-IJV shunt may be helpful to improve saturations and improve ventricular function.
Keywords
Introduction
Children with univentricular physiology and reduced pulmonary blood flow have traditionally been treated with staged surgical palliation culminating in completion of the Fontan circulation. The first stage is a classic or modified Blalock-Taussig shunt or any other systemic-to-pulmonary-artery shunt. Subsequently, they undergo a superior cavopulmonary anastomosis, most often in the form of a bidirectional Glenn (BDG) anastomosis. 1 After a variable period of time, most of these patients will undergo the final palliation by way of establishment of total cavopulmonary connection, also known as the Fontan operation.
The BDG anastomosis ameliorates the volume overload on the functional single ventricle and generally provides adequate pulmonary blood flow, resulting in decreased cyanosis and improved the functional capacity of the patient. 2 After a BDG procedure, the superior vena cava (SVC) and pulmonary arterial systems are in continuity and with equal pressures. However, it has been noticed that the efficacy of this circuit may gradually decrease due to the development of venous collateral circulation between the superior and inferior vena caval systems. 2,3 In addition, in many patients there is a gradual and progressive development of intrapulmonary arteriovenous fistulae. In some patients, there is also the development of competitive flow to the upper lobes of the lungs by multiple small collateral vessels from the pleural surface. 2,3 Ultimately, the initially satisfactory physiology associated with the BDG may deteriorate, leading to hypoxemia and cyanosis, and eventually increased blood viscosity due to high hematocrit. To prevent or address these adverse effects, the principle management strategy at present is to add the total cavopulmonary connection (completion of Fontan procedure), which augments pulmonary blood flow, thereby decreasing cyanosis and related risks. The completion of Fontan procedure also directs hepatic venous blood to the lungs. Delivery of a “hepatic factor” into the pulmonary circulation is postulated to prevent or ameliorate the formation of pulmonary arteriovenous malformations (PAVMs). 4 However, the Fontan physiology is not a benign one and in the long term may be fraught with multiple complications that for some patients may necessitate cardiac transplantation as a final resort.
The early success of palliation by means of superior cavopulmonary anastomosis led clinicians to question the role of the right ventricle. 5 However, the recognition of the above-mentioned complications which may occur in the long run led to renewed interest in the role of the right ventricular pump. There is evidence that suggests pressure developed by the pulsatile pumping action of the right (subpulmonary) ventricle not only drives blood into the pulmonary circulation but helps in recruitment of pulmonary capillaries, thus bringing down the pulmonary vascular resistance, improving gas exchange, and potentially improving lymphatic drainage. 6 Moreover, the pulsatile flow generated by the right ventricle provides the stimulus for growth of pulmonary arteries.
A complication profile similar to that which can occur following superior cavopulmonary anastomosis may also exist with Fontan circulation, and it has been postulated that inclusion of pulsatility in the cavopulmonary circulation would be of immense benefit in maintaining the low pulmonary vascular resistance.
As early as 1972, Glenn and Fenn 7 described satisfactory early results after creation of an axillary arteriovenous fistula to increase pulmonary blood flow in a patient with worsening hypoxemia after the BDG. Various studies 3,8 –10 have highlighted the implied advantage of such an arrangement such as increased recruitment of pulmonary capillaries, regression of PAVMs, providing pulsatile flow to the pulmonary arteries, improvement in ventricular function, and overall improvement in the oxygen saturation of these patients.
In situations where Fontan completion could not be achieved either because of failed attempt (poor surgical exposure) or because of unfavorable anatomy, we created a central systemic artery-to-central systemic venous shunt to ameliorate the systemic hypoxemia and poor exercise tolerance. We first performed this operation in 2010 and reported on our initial experience with this technique in 2012. 11,12 Our experience has grown since then and we now present detailed results.
Materials and Methods
Between July 2010 and January 2015, eight patients (Table 1) underwent a common-carotid-artery to internal jugular vein (CCA-IJV) shunt, the “All India Institute of Medical Sciences (AIIMS) shunt”; one of these patients later underwent takedown of this shunt and conversion to left brachial artery-to-basilic vein shunt. All these eight patients had undergone a previous palliative procedure in the form of BDG. The majority of these patients were, at the time, deemed unsuitable for the completion of Fontan operation after evaluation by echocardiography, cardiac catheterization, and computed tomography (CT) angiography (the latter being used to rule out the presence of major aortopulmonary and systemic venovenous collaterals). Patients 1 and 5 in the series were proposed for Fontan completion but underwent the systemic artery-to-systemic vein shunt procedure as a “bailout” procedure after failure to clearly define the anatomy, even after successful sternal reentry following establishment of cardiopulmonary bypass through the femoral route. This retrospective review was duly approved by the institute ethics committee.
Preoperative, Intraoperative, and Postoperative Course of Each Patient.
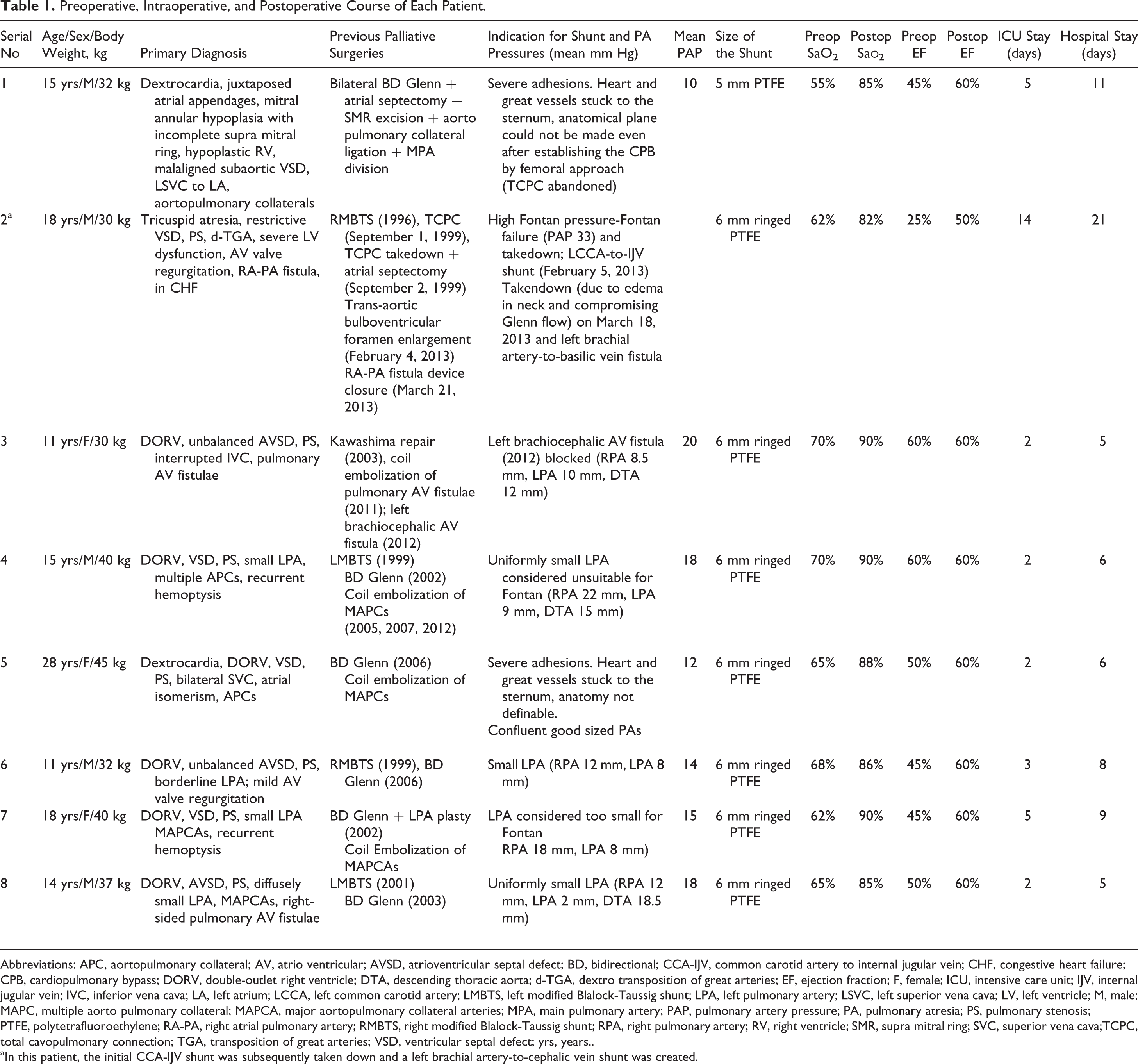
Abbreviations: APC, aortopulmonary collateral; AV, atrio ventricular; AVSD, atrioventricular septal defect; BD, bidirectional; CCA-IJV, common carotid artery to internal jugular vein; CHF, congestive heart failure; CPB, cardiopulmonary bypass; DORV, double-outlet right ventricle; DTA, descending thoracic aorta; d-TGA, dextro transposition of great arteries; EF, ejection fraction; F, female; ICU, intensive care unit; IJV, internal jugular vein; IVC, inferior vena cava; LA, left atrium; LCCA, left common carotid artery; LMBTS, left modified Blalock-Taussig shunt; LPA, left pulmonary artery; LSVC, left superior vena cava; LV, left ventricle; M, male; MAPC, multiple aorto pulmonary collateral; MAPCA, major aortopulmonary collateral arteries; MPA, main pulmonary artery; PAP, pulmonary artery pressure; PA, pulmonary atresia; PS, pulmonary stenosis; PTFE, polytetrafluoroethylene; RA-PA, right atrial pulmonary artery; RMBTS, right modified Blalock-Taussig shunt; RPA, right pulmonary artery; RV, right ventricle; SMR, supra mitral ring; SVC, superior vena cava;TCPC, total cavopulmonary connection; TGA, transposition of great arteries; VSD, ventricular septal defect; yrs, years..
aIn this patient, the initial CCA-IJV shunt was subsequently taken down and a left brachial artery-to-cephalic vein shunt was created.
Surgical Technique
Under general anesthesia, the patient was positioned supine with the neck extended and turned to the side opposite that of the shunt to be performed. An oblique incision was made along a line corresponding to the anterior border of the sternocleidomastoid muscle. Platysma was separated, and the sternocleidomastoid muscle was retracted laterally to expose the common carotid artery and the internal jugular vein. Proximal and distal control on both the vessels were obtained. Systemic heparinization was achieved by administration of heparin injection 1 mg/kg body weight. A side-biting clamp was applied on the common carotid artery, an optimum sized polytetrafluoroethylene (PTFE) graft was chosen, and an end-to-side anastomosis was performed between the graft and the artery. Similarly a side-biting clamp was applied on the vein, and an anastomosis was fashioned between the graft and the internal jugular vein in an end-to-side fashion. After deairing the graft, the distal clamp was released first followed by the proximal clamp, while the operating table was maintained in the Trendelenburg’s position. The wound was closed in layers after securing hemostasis. In the immediate postoperative period, all these patients were weaned from mechanical ventilator support within four to six hours. A pressure dressing applied to the neck was changed after 24 hours. Oral aspirin was prescribed to help ensure graft patency (Figure 1).
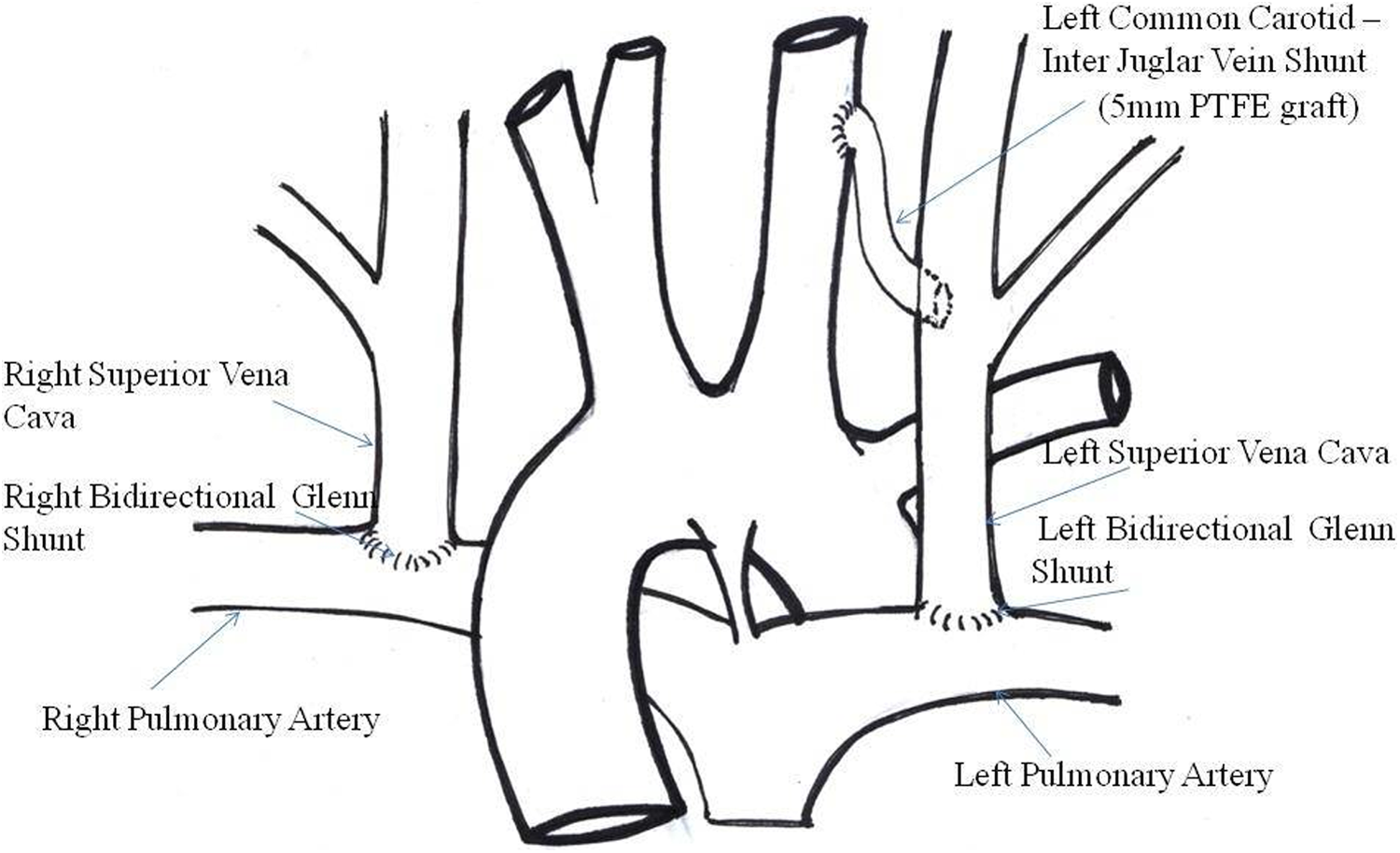
Line diagram showing bilateral bidirectional Glenn shunt in situ with left common carotid artery to left internal jugular vein shunt. Reproduced with permission from Garg et al. 11
Results
There were no early deaths. All patients underwent creation of a left-sided CCA-IJV shunt with 6 mm ringed PTFE graft except patient # 1, in whom a 5-mm PTFE graft was used. The baseline arterial saturation prior to the procedure was median 67% (range 60%-72%), which increased to median 83% (range 80%-90%) after the procedure. The preoperative Pa
The median postoperative intensive care unit (ICU) stay was 2.5 days, and the median hospital stay was 7 days. Echocardiograms prior to discharge from the hospital revealed patient shunt and preservation/improvement in ventricular function in all patients. In patient #2, who had severe ventricular dysfunction prior to the procedure, there was significant improvement in the ventricular ejection fraction.
Follow-up includes all patients and currently ranges from 6 months to 5 years (median 24 months). At the last follow-up, these patients were classified in New York Heart Association class II. The two patients (patients 1 and 5) in whom it was impossible to define the structures even after peripheral cannulation, resternotomy, and establishment of cardiopulmonary bypass are not currently considered to be candidates for any future surgical intervention. Future plans for other patients are uncertain, at this time. Further follow-up will determine whether they will eventually be considered for a Fontan completion.
No patient other than those mentioned above have developed any local complication related to the shunt. None has any evidence of cerebral steal phenomenon. Follow-up CT angiograms (Figure 2) in the first two patients have demonstrated satisfactory shunt architecture and flow.
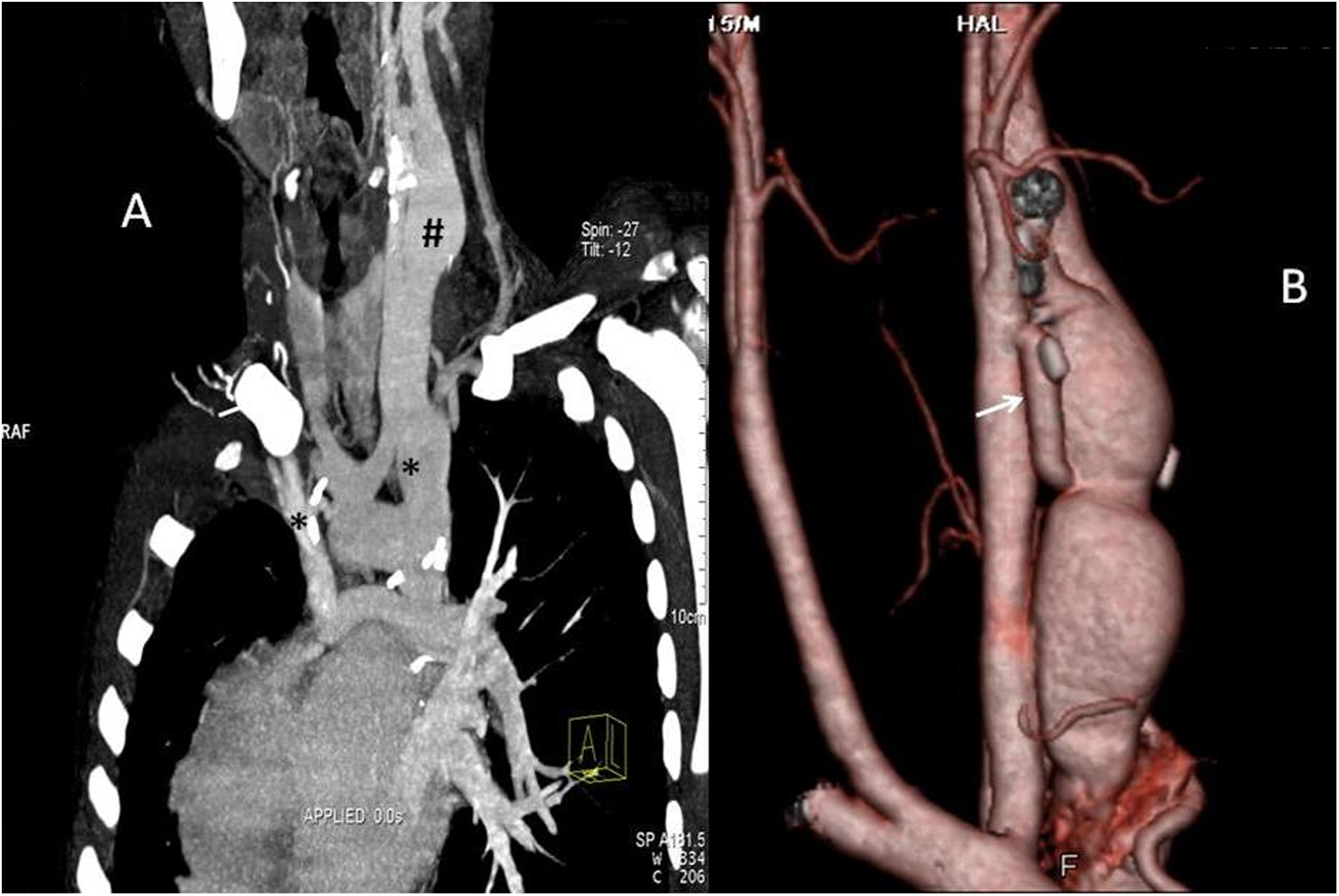
Computerized tomographic angiogram: Coronal thick multiplanar reconstruction. A, * indicates the right and left bidirectional Glenn. # indicates the dilated left internal jugular vein. B, Volume-rendered reconstruction, showing the shunt placed between the left carotid artery medially and the dilated internal jugular vein laterally. Reproduced with permission from Garg et al. 11
Discussion
In our series of patients, in view of their persistent hypoxemia and decreased exercise tolerance due to high hematocrit and cyanosis, the logical option was to increase the pulmonary blood flow. However, for a variety of indications listed in Table 1, these patients were not considered to be suitable candidates for a Fontan procedure. In two patients (patients 1 and 5), the Fontan completion was abandoned intraoperatively because the anatomy could not be defined even after sternal reentry and the institution of cardiopulmonary bypass by the femoral route. In four patients (patients 4, 6, 7, and 8), the left pulmonary artery was uniformly small and we considered them to be unsuitable for Fontan completion. In these cases, we felt that the left pulmonary artery was not amenable to an augmentation procedure. In one patient (patient 3), the pulmonary artery pressure was too high for the Fontan completion. Finally, one patient (patient 2) had a previous Fontan takedown (see subsequently). Hence, we elected to perform a CCA-IJV shunt. Various studies indicate that creation of systemic artery-to-systemic venous shunts in patients with superior cavopulmonary connection increases pulmonary blood flow, decreases the development of pulmonary arteriovenous fistulae, and improves systemic oxygen saturation. 3,8 –10 All of our patients have been under close follow-up since their surgery, and all have showed improvement in oxygen saturation from 35% to 50% to 80% to 85% and reduction in polycythemia. Follow-up CT angiography of the neck and chest confirmed increase in pulmonary blood flow and no intrapulmonary collaterals, and none of them had any neurological complication. One patient (patient 2) developed severe head and neck edema and proptosis due to lymphedema surrounding the shunt caused by lymphadenopathy. In this one case, we needed to take down the shunt and recreate another shunt between the left brachial artery and cephalic vein. This patient also had severe left ventricular (LV) dysfunction and needed longer ICU stay due to inotropic requirement. He had previously undergone an unsuccessful Fontan completion with enlargement of the bulboventricular foramen and had required Fontan takedown. At the time of this admission for CCA-IJV shunt, he had persistent hypoxemia. He also had a history of long-standing tuberculosis. It is unclear what relationship this may have had to the development of cervical lymphadenopathy, as mentioned earlier.
The appropriate size and site for the shunt are a matter of debate. 12 We have preferred to perform these shunts in the neck because many of these patients have undergone previous thoracotomies and it is therefore technically easier to construct the CCA-IJV shunt as compared to thoracotomy shunts. This approach also prevents damage to any previous cavopulmonary shunts. When compared to peripheral sites, the vessels are much bigger, and shunts are easier to construct and less likely to kink. Also there may be an increased risk of infection of grafts at peripheral sites because of indwelling peripheral venous lines. The shape and length of the graft should be just adequate to make a “sinus” curve, with the carotid anastomosis higher than the internal jugular vein anastomosis. We believe that it is advantageous to use ringed PTFE grafts because the chances of kinking are much less. There should not be too much redundancy in the graft, which may lead to stasis and thereby thrombus formation. In previous canine experiments, 13 it has been shown that a shunt size of 0.9 to 1.0 mm/kg body weight is probably ideal to control the pulmonary blood flow. Whether these findings hold true in humans is at best a matter of speculation. According to such a formula, a very large shunt would be needed in large patients. Notwithstanding this, we prefer to place a shunt of size 6 mm, as the central vessels are larger than this and our experience suggests that a 6 mm graft provides adequate flow without unnecessary volume loading of the single ventricle. However, this issue is debatable and needs further evaluation.
Study Limitations
This is a retrospective analysis of only eight patients and thus suffers from the limitations of any small retrospective study. We do not have any objective evidence of regression/failure of progression of PAVMs, and CT angiography may be a useful tool to assess this in the long term. As of now, it may not be justifiable to compare the routine use to this technique to a Fontan with or without fenestration in borderline conditions.
Although the CCA-IJV cannot satisfy all the traditional characteristics of an ideal shunt (ease of performance and takedown, should not worsen the LV function or overload the pulmonary circulation, and should grow with the patient), 2 our experience suggests that in a selected group of patients who at the time are considered unsuitable for Fontan circulation, creation of a CCA-IJV shunt may be helpful to improve saturations and improve ventricular function. Only further follow-up will demonstrate the longevity of palliation afforded by this technique and resolve the question of whether such an interim palliation may alter the chances of successful Fontan completion in the future. More objective evidence of the role of these shunts in prevention/regression of established PAVMs is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.