
Abstract
We present the case of a 60-year-old female with pulmonary artery aneurysm (PAA) associated with an atrial septal defect and pulmonary arterial hypertension. There is no standard therapeutic approach for PAA at the present time. We performed a novel surgical repair of a 67-mm PAA consisting of internal plication of the pulmonary artery to reduce the diameter and approximation of remnant unfolding pulmonary artery to reinforce the stability of the pulmonary artery and prevent bleeding.
Introduction
Pulmonary artery aneurysm (PAA) is a rare disease that is commonly associated with pulmonary hypertension. 1 Pulmonary artery aneurysm can lead to mortality due to the development of dissection and rupture, but there are currently no standard guidelines for its management or treatment, including surgical methods. In this report, we present the novel surgical repair of a 67-mm PAA in a 60-year-old female patient with an atrial septal defect (ASD) and pulmonary arterial hypertension.
Technique
A 60-year-old female patient with an ASD was admitted to hospital to undergo surgery. The patient had been healthy until dyspnea on exertion developed. A chest radiograph revealed cardiomegaly with prominent pulmonary conus (Figure 1A). Her preoperative systolic pulmonary artery pressure was 88 mm Hg when systolic blood pressure was 130 mm Hg and pulmonary vascular resistance was 12.33 Wood units, which was responsive to acute vasodilator challenge using oxygen and iloprost. The size of the main pulmonary artery was 67 mm, and right and left pulmonary artery size was 51 and 41 mm, respectively. Because of high pulmonary artery pressure, we planned to close the ASD with a fenestrated patch and to perform pulmonary artery reduction plasty.
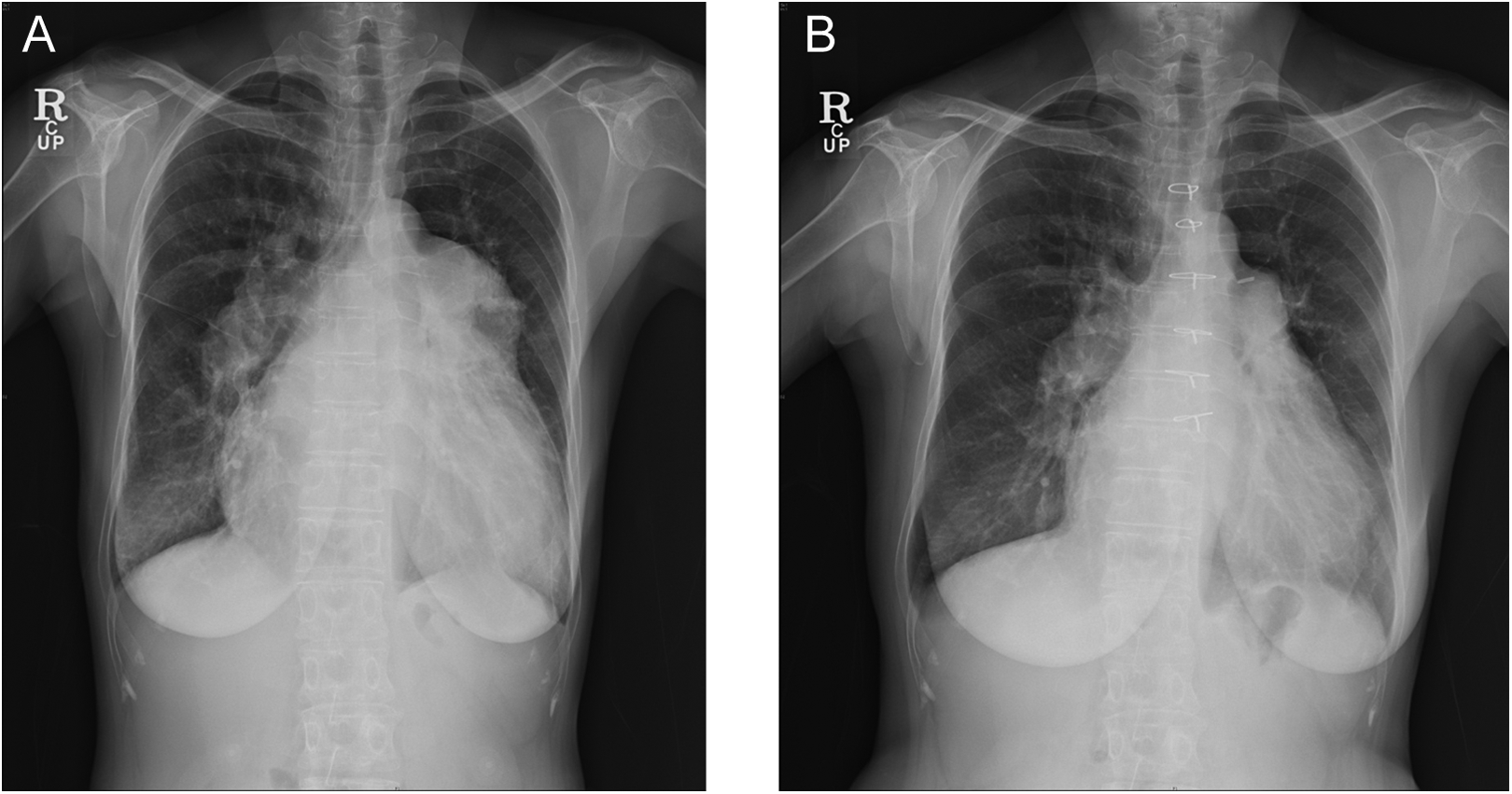
A, Preoperative chest X-ray. B, Follow-up chest X-ray 12 months after the operation.
The operation was performed using median sternotomy. Under routine cardiopulmonary bypass, the right and left pulmonary arteries were mobilized from the main pulmonary artery to both hilar portions. After aortic cross clamping, we performed a bilateral maze operation for atrial fibrillation and an ASD patch repair with fenestration due to pulmonary arterial hypertension (mean pulmonary arterial pressure, 55 mm Hg). Tricuspid annuloplasty was also performed using the DeVega method to correct moderate tricuspid regurgitation. After the intracardiac procedures, the right pulmonary artery was longitudinally incised from beneath the aorta to the superior vena cava. The left pulmonary artery incision was made separately, from the sinotubular junction of the main pulmonary artery to the left pulmonary artery up to the left hilum (Figure 2A). After the pulmonary artery was open, we placed continuous internal plication sutures to reduce the diameter. The remnant unfolding pulmonary artery was closed with a 5-0 polypropylene suture to reinforce the stability of the pulmonary artery and prevent bleeding (Figure 3). Trivial to mild tricuspid regurgitation and decreased diameter of both pulmonary arteries were observed on intraoperative transesophageal echocardiography. After weaning from bypass, the measured pulmonary arterial systolic pressure was 30 mm Hg when the systolic blood pressure was 100 mm Hg. The cardiopulmonary bypass time was 137 minutes, and the aortic cross clamp time was 73 minutes. Computed tomography (CT) imaging showed a remarkable reduction in both pulmonary arteries (Figure 2B).
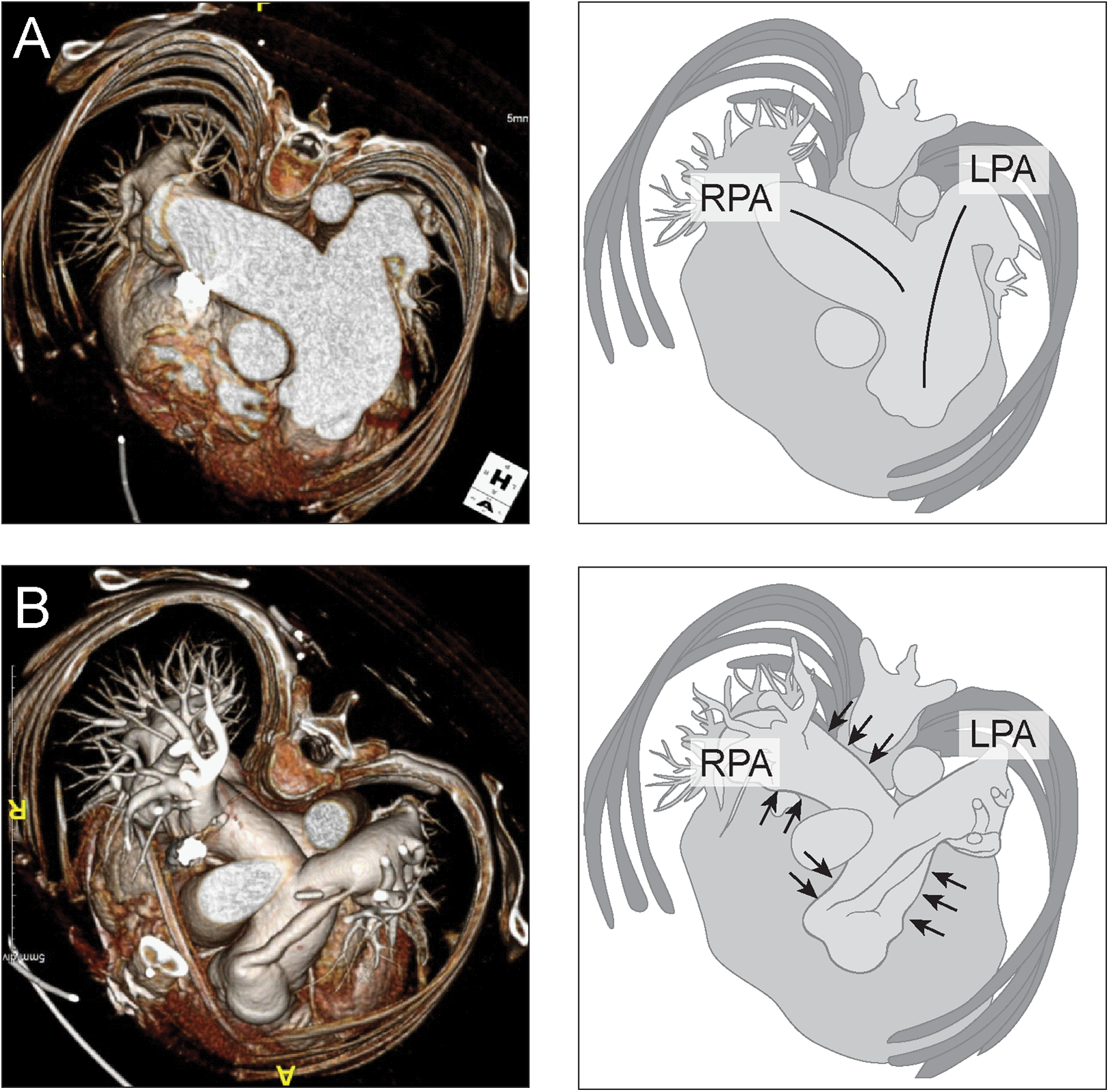
A, Preoperative computed tomogram showing a huge dilated pulmonary artery (left) and the incision lines of both pulmonary arteries (right). The right pulmonary artery (RPA) was longitudinally incised from beneath the aorta to the superior vena cava. The left pulmonary artery (LPA) incision was made separately, from the sinotubular junction of the main pulmonary artery to the left pulmonary artery up to the left hilum. B, Reduced size of the pulmonary artery shown in the postoperative computed tomogram (left) and diagram (right).
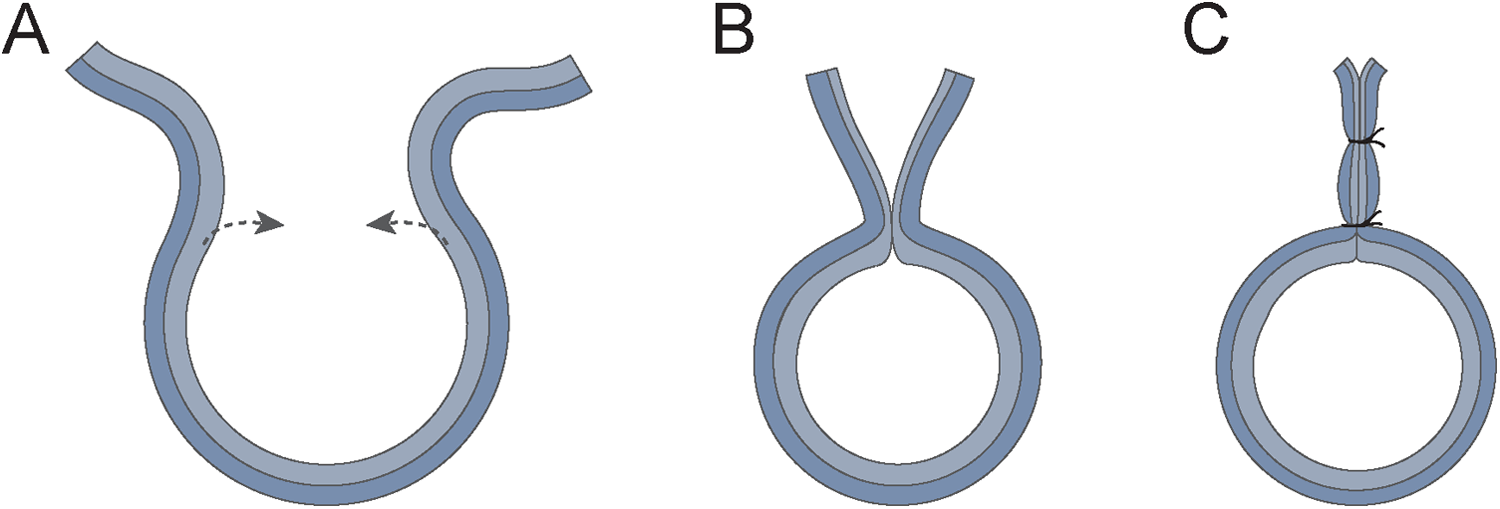
A, Opening of the pulmonary artery lumen. B, Continuous internal plication suture to reduce the diameter. C, The unfolding remnant pulmonary artery was closed with a 5-0 polypropylene suture.
A follow-up echocardiogram 12 months later showed size decreases of 31 mm in the right pulmonary artery and 24 mm in the left pulmonary artery. The patient is well at follow-up with no sign of dyspnea. The follow-up chest X-ray showed decreased heart size (Figure 1B).
Discussion
There is no standard therapeutic approach for PAA because of the rarity of information about its natural history and long-term outcome following medical or surgical intervention. Especially, idiopathic PAA can be found in only a few case reports. 2 –4 However, if the patient has an acceptably low operative risk, surgical repair should be recommended for PAA regardless of its etiology and underlying disease in order to prevent fatal rupture. 5
In this case, because we were unable to predict normalization of pulmonary artery pressure with certainty, we felt it would be unwise to leave the aneurysmal main pulmonary artery of 67 mm untreated. If we had planned to close the ASD totally, we may have felt less strongly about the need to perform a pulmonary angioplasty. However, because we planned partial closure of the ASD, we did a pulmonary reduction plasty to prevent possible further dilatation of the pulmonary artery. Our treatment was consistent with the recommendations of Deb et al, that enlarged aneurysms (>6 cm) and those that are symptomatic of any size should be repaired, particularly in patients with right ventricular dysfunction or elevated pulmonary artery pressures. 4
To date, a few surgical techniques have been performed to repair PAA, including aneurysmorrhaphy, 5,6 Dacron graft replacement, 5,7 and replacement by the combined use of a stentless bioprosthesis and Dacron prosthesis. 8
Aneurysmorrhaphy is a relatively quick and simple procedure, but it can lead to recurrent dilatation due to the continued presence of the aneurysmal wall, especially in patients with associated pulmonary hypertension or structural cardiac lesions. In one case, late progressive redilatation of the PAA was observed 9.5 years after aneurysmorrhaphy. 5 A Dacron graft replacement can prevent redilatation, but it uses foreign material and can be associated with difficulty controlling bleeding in the deep anastomosed site, as it is difficult to expose areas such as the left pulmonary artery hilum. According to the Laplace law, wall stress is directly proportional to the vascular pressure and radius of the vessel and is inversely related to the wall thickness. Thus, we attempted to decrease the radius and increase the wall thickness using a novel pulmonary artery reduction plasty, including internal plication and outer layer reinforcement. This technique has several advantages, as there is no use of foreign material, it easily controls bleeding, and the wall thickness is increased to reduce the pressure.
We think this different pulmonary artery reduction plasty can be effective to treat PAA with concomitant congenital heart disease with elevated pulmonary artery pressure.
Footnotes
Acknowledgments
The authors would like to thank Dong-Su Jang, MFA (Medical Illustrator, Medical Research Support Section, Yonsei University College of Medicine, Seoul, Korea) for his help with the illustrations and Han Ki Park (Severance Cardiovascular Hospital) for suggesting idea related to the surgical technique.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.