
Abstract
Background:
Parents of children having congenital heart diseases (CHDs) develop symptoms of depression, distress, anxiety, and hopelessness more frequently than parents of healthy children. Associated with the described symptoms, parents may experience a lack of control and disempowerment, which decreases the parent’s agency, a construct from development studies, and which may have negative consequences on adherence to treatment. The primary aim of this study was to assess the effect of medical treatment on well-being and agency in parents of children having CHDs, in Chile, and to compare it with reference values.
Methods:
Forty parents of children having CHDs (before surgery and before hospital discharge) and 115 parents of healthy children were surveyed. The following scales were applied to this population: the General Health Questionnaire, the Basic Psychological Needs Scales, the Self-Determination Scale, the Beck Hopelessness Scale, and a socioeconomic survey.
Results:
Children’s surgery decreased parents’ hopelessness (3.13 ± 0.35 and 2.18 ± 0.40, P = .04), and no significant differences were found in the remaining scales. Parents of children with CHDs scored significantly worse than parents of healthy children on the General Health Questionnaire (13.82 ± 1.03 and 9.21 ± 0.64, P = .001). This difference was not found using the others scales.
Conclusion:
Children’s surgery has a positive effect on parent’s hopelessness, but it does not have any impact on their well-being nor agency. Parents of children with CHD have a decreased well-being compared to parents of healthy children but have a similar level of agency. Socioeconomic level and gender may influence this association.
Introduction
Congenital heart disease (CHD) refers to a wide range of cardiac defects present at birth, from innocent murmurs to severe structural abnormalities. It is estimated that about 1% of children are born with a CHD, many of whom used to die during the first year of life. 1 However, due to improvements in health care, mortality has been reduced considerably in the last two decades, and it is estimated that 85% of these children now reach adulthood. 2
Besides the effects on the child’s health, the uncertainty associated with the diagnosis of a CHD and the high demand for care that a child with CHD has can lead parents to develop symptoms of depression, distress, anxiety, and hopelessness 3 –8 more frequently than parents of healthy children. 3 This occurs more often than with other chronic conditions, such as cystic fibrosis. 9 However, an explanation of this phenomenon has not been proposed so far. Studies exploring risk factors for the development of these symptoms have yielded diverging results: low socioeconomic level, 3 the severity of the CHD, 6 and the parent being female, independent of the marital status 3,8 have been identified.
Associated with these symptoms, many parents of children with CHD perceive their situation as uncontrollable, 4 and “mothers of these children attributed events to chance or luck and beyond their control.…” 7(p606) Although experiences of lack of control and disempowerment have been described more often in patients, they are also present in caregivers of children with chronic conditions, such as neurological degenerative diseases. 10 Empowerment has been defined as “the ability to exercise meaningful choices,” 11 (p437) and it depends on two main determinants: an external factor, called social agreement, made up of resources and opportunities, and an internal factor denominated agency, which is defined as “the ability to act on behalf of what you value and have a reason to value.” 12 (p383) Agency is a relevant concept for development studies, a branch of economy and social sciences dealing with “beneficial societal change,” 13 (p1) since this discipline aims at making assisted people not mere recipients of aid programs but engaged partners in their own development. 14 Some conditions of agency have been described: the agent performs the activity or at least has a role in performing it; that this activity has an impact on the world; that the agent chooses the activity; and that the agent deliberates on the activity in light of his or her values, judging it as valuable for its own sake. 15 This is not an all-or-nothing process but a gradual one in which people can exert more or less agency over their lives, according to their circumstances.
In the field of health care, it has been shown that the lack of agency affects recuperation because it has negative consequences not only on well-being, as some parents may feel overwhelmed when they face medical decisions, 7 but also on the adherence to treatment. 16 Hence, depression, distress, anxiety, and hopelessness are very severe issues because of the consequences not only for parental well-being but also for the child’s treatment.
In Latin America, there is a severe shortage of pediatric cardiac surgical teams, leading to a lack of appropriate medical treatment of children with CHD. The lack of health care providers makes this population highly vulnerable. To our knowledge, only one qualitative study has been conducted which explores the feelings and emotions of Latin American parents of children with CHD. In its conclusion it claimed, “The main feelings encountered during this time of crisis have been fear of death by heart disease, surgery and anaesthesia, guilt and powerlessness in the face of the different stages of treatment.” 17 (p41)
The primary aim of this study was to assess the effect of medical treatment on well-being and agency in this population, to compare it with reference values, and to identify other factors that may be associated with parental well-being and agency. The hypothesis is that parents of children with CHD have a decreased well-being and agency compared to parents of healthy children. A second hypothesis is that medical treatment of their children has a positive effect on parent’s well-being and agency.
Materials and Methods
Study
A quantitative prospective longitudinal study was conducted that included two measurements over time for the study group and one measurement for a control group. The local institutional review board had approved this study before its implementation.
Population
Parents of children younger than 5 years of age receiving medical treatment for CHDs (parents of sick children [P-SC]) at the Catholic University Clinical Hospital in Santiago de Chile, one of three reference centers for pediatric cardiac surgeries in Chile, were contacted to participate in the study. Parents of healthy children (P-HC) were included as control group to obtain reference values. Only parents currently living with their children were included. Exclusion criteria were parents younger than 18 years old, illiterate, emergency surgery, and parents whose children died after surgery.
Procedures and Measures
After their children’s admission for cardiac surgery, but before the procedure, P-SC completed a selection of psychological self-report scales and a socioeconomic survey questionnaire. An informed consent form was signed beforehand. Only the psychological scales were reapplied before discharge from hospital. The same scales were applied to the control group (P-HC) after routine checkup with the pediatrician (Figure 1).
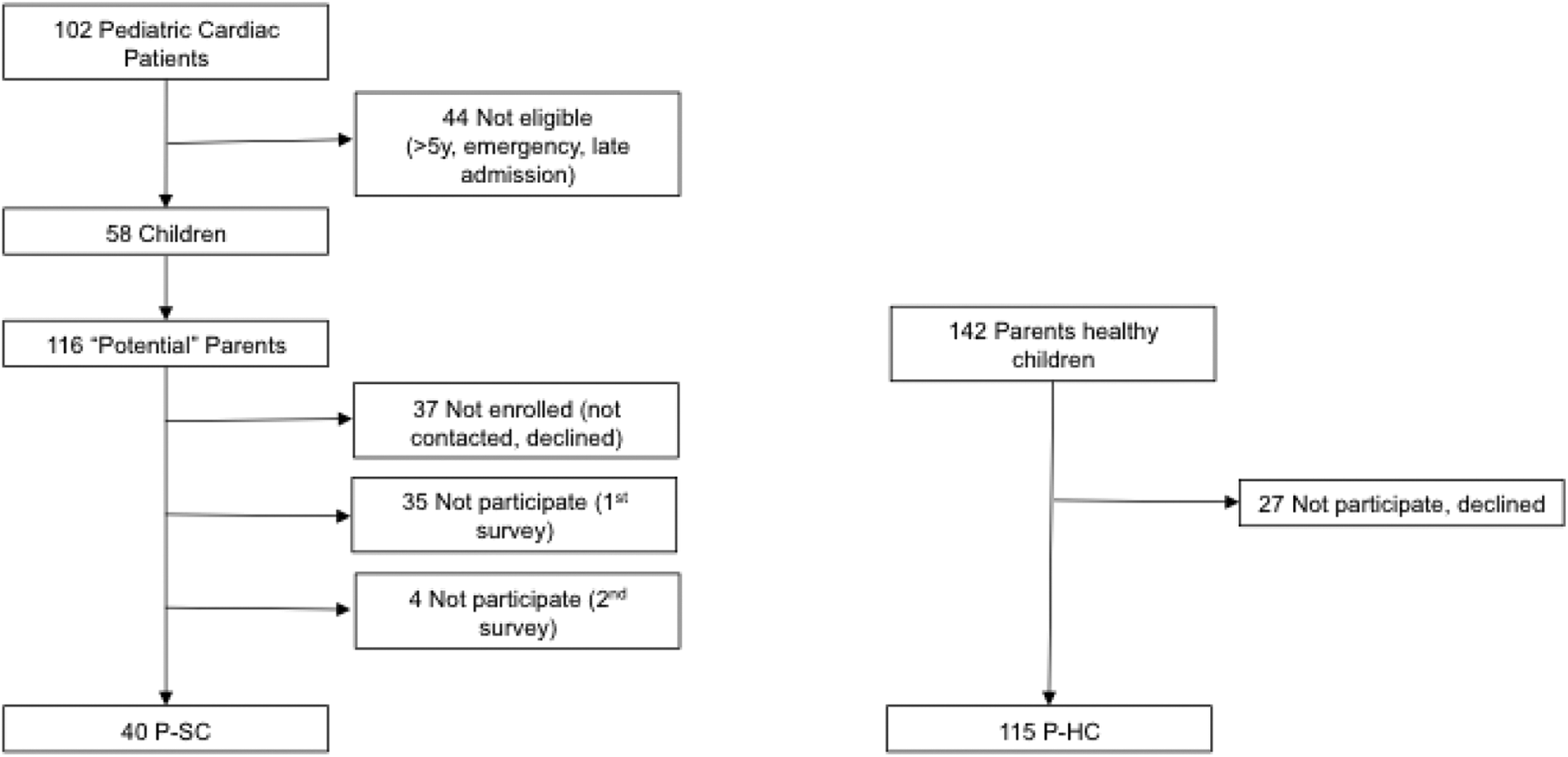
Procedures and samples size. P-SC indicates parents of sick children; P-HC, parents of healthy children.
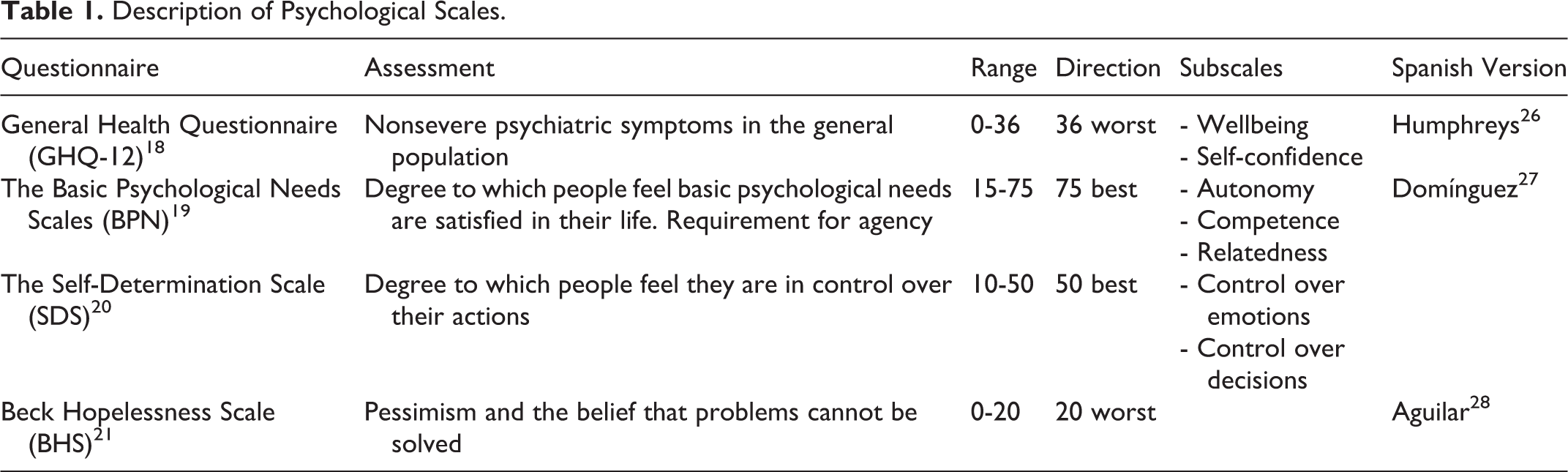
In order to assess well-being and agency, the following questionnaires were used: General Health Questionnaire (GHQ-12), 18 the Basic Psychological Needs Scales (BPN), 19 the Self-Determination Scale (SDS), 20 and the Beck Hopelessness Scale (BHS) 21 (Table 1).
Description of Psychological Scales.
Socioeconomic level (SEL), a relevant factor according to a previous study, 3 was measured by a sample of questions from the survey regularly conducted by the Chilean Ministry of Social Development. 22 The selected dimensions and indicators were age, marital status, education (literacy, highest degree obtained), work (employment, contract), health (insurance, perceived health status), and housing/neighborhood (number of people living in the house, social participation). These socioeconomic data were analyzed independently and also transformed into a dichotomous variable (poverty) according to the multidimensional poverty concept. 23
Severity of the child’s disease was registered according to RACHS-1 (Risk Adjustment for Congenital Heart Surgery score), 24 with expected mortalities ranging from 0.3% for group 1 to 40% for group 6. 25 Other measured variables included the child’s age, number of surgeries of the child, parental satisfaction with free time (1-10), and parental perception of own health status (1-7); the last variables may be relevant for variations in agency. 29
Statistical Analysis
The data were examined with analyses of variance, chi-square tests, and t tests, paired or unpaired according to the samples, and post hoc tests using the Bonferroni method. When the distribution did not pass normal distribution tests, the Kolmogorov-Smirnov test was performed.
Results
Data were collected from October 2013 to Mach 2014 on a consecutive basis. During that period of time, 102 pediatric patients underwent surgical treatment at our hospital. Eighteen children did not meet the inclusion criteria, and 26 were admitted during weekends or at night and their parents were not invited to participate because the researchers were not available. Of the 116 potential parents, the research team was not able to contact 22, and 94 P-SC were invited to participate. In total, 28 declined, 35 did not return the first survey, and 4 did not return the second survey (preoperative and before hospital discharge). The control group included 115 P-HC. Sample sizes are shown in Figure 1. The demographic characteristics of the participants are shown in Tables 2 and 3. The results of the psychological tests are shown in Table 4. Averages and standard deviations or percentages are presented.
Demographic Data.a
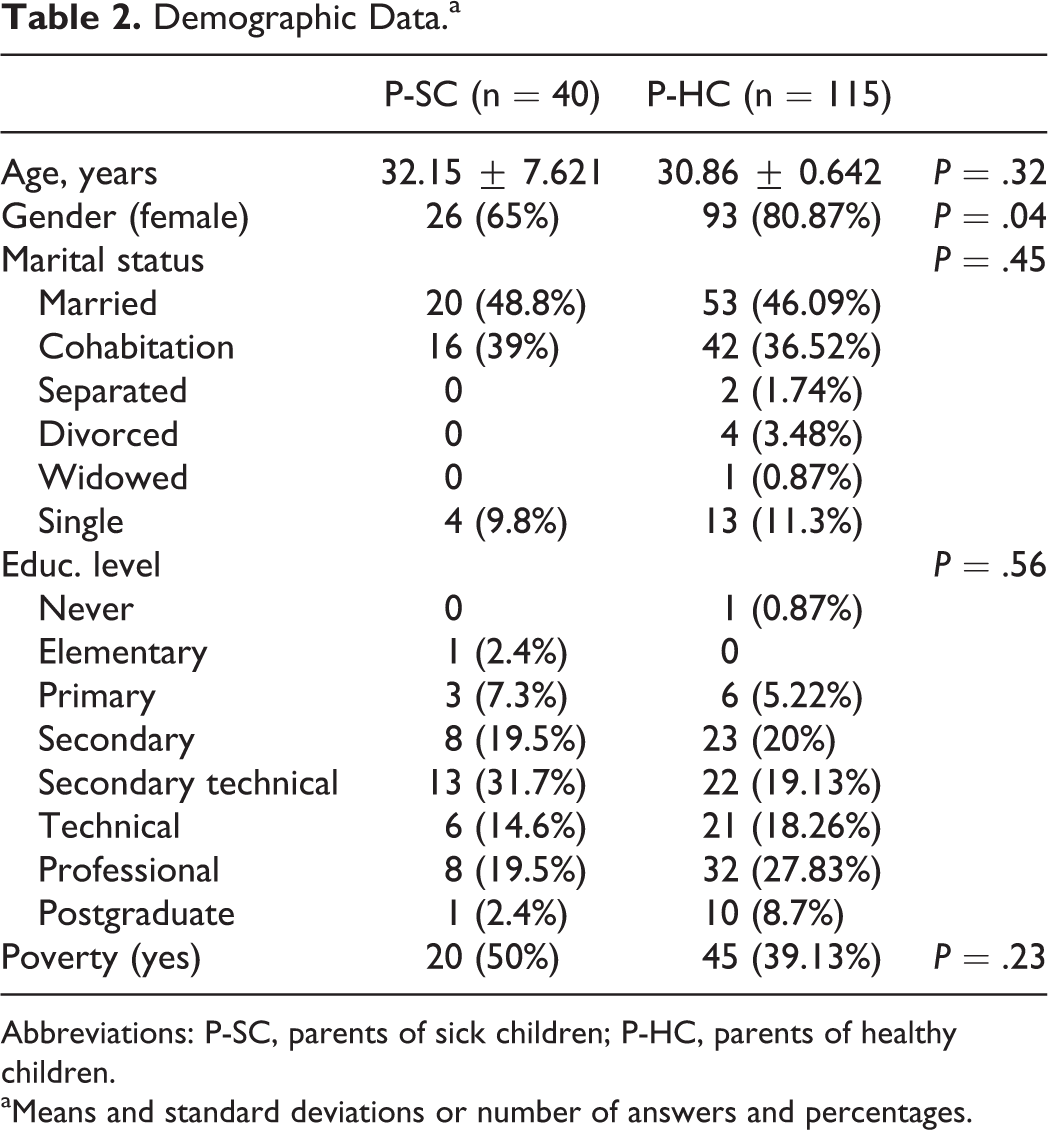
Abbreviations: P-SC, parents of sick children; P-HC, parents of healthy children.
aMeans and standard deviations or number of answers and percentages.
Characteristics of Children’s Disease.a
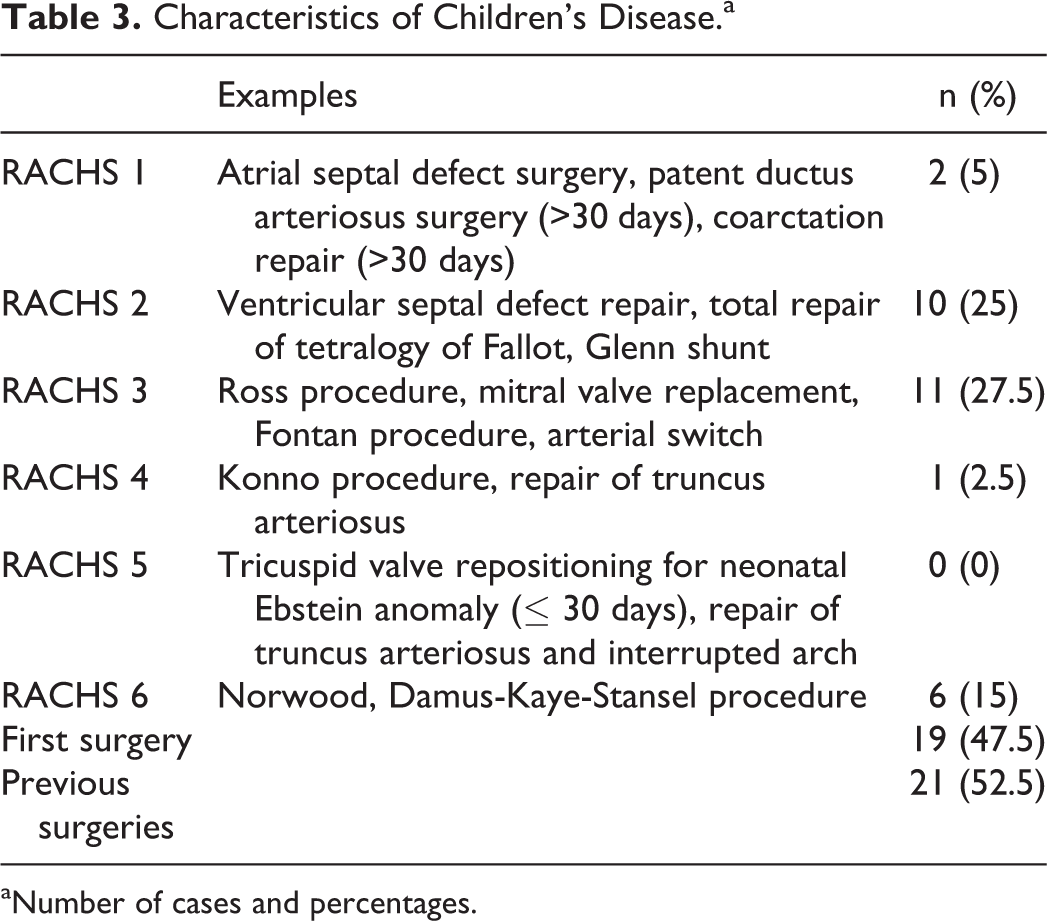
aNumber of cases and percentages.
Overall Results: Well-Being and Agency.a
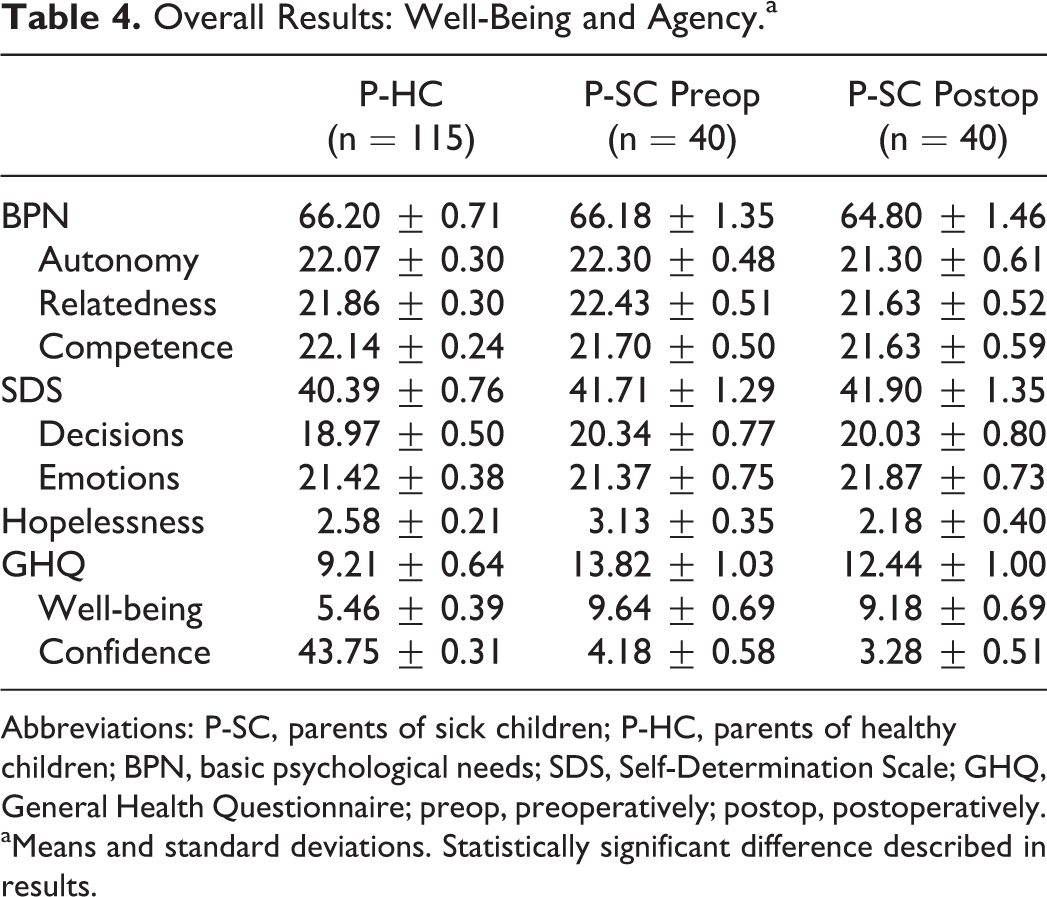
Abbreviations: P-SC, parents of sick children; P-HC, parents of healthy children; BPN, basic psychological needs; SDS, Self-Determination Scale; GHQ, General Health Questionnaire; preop, preoperatively; postop, postoperatively.
aMeans and standard deviations. Statistically significant difference described in results.
Well-Being and Agency of Parents of Children With Congenital Heart Diseases by Gender and by Socioeconomic Level.a
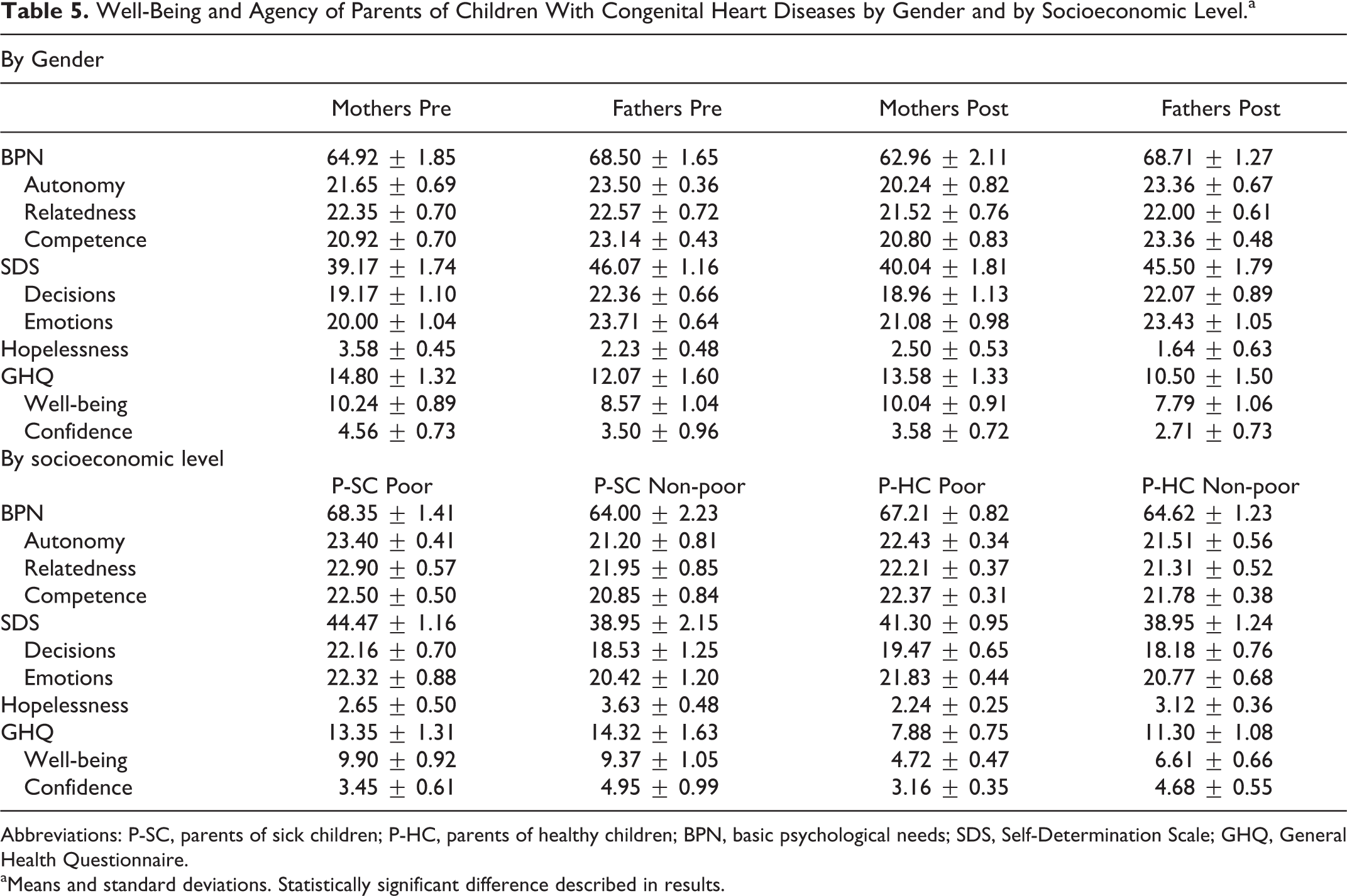
Abbreviations: P-SC, parents of sick children; P-HC, parents of healthy children; BPN, basic psychological needs; SDS, Self-Determination Scale; GHQ, General Health Questionnaire.
aMeans and standard deviations. Statistically significant difference described in results.
Disease, Well-Being, and Agency
Children’s disease was associated with lower well-being. The P-SC scored significantly worse than P-HC on GHQ-12 and its subscale well-being (P = .001 and P = 0, respectively). No difference was found among the study groups in the other applied scales, namely, in the BHS, BPN, and SDS. Hence, an association between CHD and decreased agency was not shown. Eight parents, four in each group, had hopelessness values higher than 8, which is associated with severe depression. All of them were referred to psychiatric consultation to confirm diagnosis and start treatment, if required.
Effect of Medical Treatment
Children’s surgery decreased their parents’ hopelessness (P = .04). No significant differences were found in the remaining scales (BPN, SDS, and GHQ-12).
Gender, Well-Being, and Agency
Fathers of healthy children showed similar values in all the selected scales compared to mothers of healthy children. In contrast, in the P-SC group, male parents showed higher perceived autonomy and competence (subscales of the BPN) than female parents before (P = .03, and P = .04, respectively) and after (P = .02 and P = .04, respectively) surgery. Fathers also scored better than mothers in the SDS and its subscales (control over decisions and control over emotions) before surgery (P = .02, P = .04, and P = .03, respectively), but no significant difference was found in this scale after surgery (Table 4).
Poverty, Well-Being, and Agency
In the P-HC group, poverty was associated with worse values on the GHQ-12 scale (P = .008) and both of its subscales, namely, well-being (P = .02) and confidence (P = .02). Before surgery, poor P-SC scored worse than nonpoor P-SC in many scales assessing agency, namely, autonomy (P = .02), SDS (P = .03), and control over decisions (P = .02). After surgical procedure, only the differences in the control over decisions scale (P = .02) between those groups persisted.
Discussion
As many other studies have shown, parents of children with CHD showed lower well-being compared to parents of healthy children. 3 These findings confirm one part of the first hypothesis that parents of children with CHD have a decreased well-being compared to parents of healthy children and that this association is affected by SEL and gender. Nevertheless, the present findings did not support the second part of this hypothesis, namely, that P-SC would also show lower agency values than P-HC, since such differences were not found by means of the selected scales.
As was commented, studies exploring risk factors for low well-being have yielded diverging results. One study reports that low SEL is a risk factor for increased anxiety and depression, 3 but these results were challenged by Uzark and Jones. 4 In our study, we did find an association between lower well-being and SEL. As it was the case for Spijkerboer et al 30 and Brosig, 31 we did not find a correlation between well-being and severity of illness. However, in contrast to Brosig, 31 our results showed a statistically significant difference for well-being according to parental gender, as Lawoko and Soares 3 and Franich-Ray et al 8 did.
Full evidence supporting the hypothesis regarding agency was not found. This could possibly be explained by an inappropriate selection of scales or a too small sample size. However, the pattern of the results permits some interesting insights: Significant differences in well-being (GHQ-12 and its subscales) were found when parents had one burden (diseases or poverty), but variations in agency (BPN and SDS) were found when more than one condition was present (diseases and poverty, and likely disease and female gender). These results echo Menahem et al’s findings, 7 showing that mothers of children with CHDs do not feel in “control.” This phenomenon could be related to mothers being more attached to their children or to gender issues in Latin American countries, but more research has to be done in order to solve this question. Is well-being more sensitive to external stressors than agency? Remarkably, all the different groups showed the same scores with regard to relatedness, which is known to be a powerful tool for coping with adverse situations. 32 More research has to be performed in order to support this preliminary result. Meanwhile, health care providers should pay attention to parental well-being when their children are sick. Furthermore, special care should be taken with those having a second burden, such as poverty or gender issues.
The scales used to test the second hypothesis concerning the effect of medical treatment on parents’ well-being only showed an improvement in the hopelessness scale, without any variation in the remaining scales. There was a small nonsignificant difference in the GHQ-12, suggesting an improvement in their well-being and confidence. These findings might be influenced by their previous personal experiences (first surgery vs multiple surgeries), but the present sample size was too small to perform a subgroup analysis.
The relationships between illness, poverty, gender, well-being, and agency seem to be complex in nature. Although the present findings suggest that this is a relevant issue, more research has to be performed in order to understand possible variations and causal relationships.
Strengths and Limitations
To our knowledge, the present study is the first in assessing the well-being of parents of children with CHD, in a Latin American country. The cultural variations between this context and those in which previous studies were carried out may produce relevant differences in people’s feelings and behavior that should be taken into account and make these results nonapplicable to other contexts. Illiteracy, for instance, could be deemed a relevant factor in compromising parent’s agency. In this study, it was not examined since its prevalence in Chile is extremely low and it would be difficult to include illiterate participants to make a conclusion with enough power. 26 Nevertheless, illiteracy could be surveyed as a relevant variable in other Latin American countries. The fact that this was a single-center study, the small sample size, the short time frame, and the limited availability of validated scales in Spanish can be seen as the most relevant limitations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.