
Abstract
Neonatal arterial switch operation for simple dextro-transposition of the great arteries (d-TGA) has almost eliminated the occurrence of pulmonary vascular obstructive disease compared to patients who underwent Mustard or Senning procedure at an older age. We report a case of a neonate with d-TGA and intact ventricular septum who underwent arterial switch operation and yet developed severe pulmonary vascular obstructive disease within two months.
Keywords
Introduction
Several factors are associated with persistent pulmonary vascular obstructive disease (PVOD), or pulmonary hypertension (PH), in patients with congenital heart disease; these include prolonged exposure to increased pulmonary blood flow, elevated pulmonary arterial or venous pressure, changes in pulmonary arterial hemoglobin oxygen saturation, acidosis, and high hemoglobin concentration. 1 Neonatal arterial switch operation (ASO) for simple dextro-transposition of the great arteries (d-TGA) has all but eliminated the occurrence of PVOD compared to patients who underwent Mustard or Senning procedure for d-TGA at an older age, usually 6 to 12 months of age. 2 We report a case of a neonate with d-TGA and intact ventricular septum (IVS) who underwent successful ASO at three days of life and yet developed PVOD within two months of operation.
Case Presentation
In 2012, a full-term male infant with a birth weight of 3.25 kg and APGAR scores of 8 and 8 at one and five minutes, respectively, developed hypoxia (SpO2 40%-50%) very soon after birth. No fetal echocardiography was performed during the pregnancy stage. Arterial blood gas obtained at that time revealed pH 6.9 with a partial pressure of oxygen, arterial (PaO2) of 15 mm Hg; the infant was intubated, placed on mechanical ventilation with a fraction of inspired oxygen (FIO2) at 100% and inhaled nitric oxide (iNO) 20 ppm, and started on prostaglandin E (PGE) 1 infusion. An echocardiogram revealed d-TGA with IVS, and restrictive patent foramen ovale (PFO). Ductus arteriosus was not visualized. He was then transferred to our center after umbilical arterial and venous lines were placed. His preductal SpO2 was 48% to 53%, and postductal SpO2 was 57% to 66% during the transport and on admission. Echocardiography upon arrival showed the size of PFO as 2.5 mm with left to right shunting, and the ductus arteriosus as 2.4 mm with left to right shunting. He was taken to the catheterization laboratory at 10 hours of life for emergent balloon atrial septostomy (BAS), which resulted in immediate improvement in systemic oxygen saturation to 82% to 89%. SpO2 at arrival to cardiovascular intensive care unit after BAS was 81% to 84% on FIO2 35%, and PGE1 and iNO were discontinued. He was extubated next day, and both pre- and postductal SpO2 were 86% on O2 2 L/min (FIO2 30%). SpO2 before surgery was 77% on O2 2 L/min (FIO2 40%). The size of PFO was 5 mm by echocardiography both soon after BAS and one day prior to surgery.
At day 3 of life, this infant underwent an uncomplicated ASO. A transthoracic central line was placed in the right atrium at operation, and the umbilical arterial and venous lines were removed on postoperative day (POD) 1. He was extubated to high flow nasal cannula on POD2. His postoperative course was uncomplicated except for the development of bilateral chylothorax which resolved within a few days after transition to a medium chain triglyceride-based formula. Echocardiography showed no thrombus in the superior vena cava. At no time did he have a central line or peripherally inserted central line in the upper extremities. The postoperative echocardiogram demonstrated a good biventricular function and normal neoaortic and neopulmonary valve function. Pulmonary artery pressure (PAP) was estimated to be normal based on the trivial tricuspid regurgitation (TR) jet and mildly increased wall thickness of the right ventricle (RV). The repeated echocardiography also showed trivial TR, and no other signs of PH. The oxygen saturations were 98% to 99% on room air and he was discharged home on POD 24.
At two-month follow-up visit, this infant was noted to be thriving, but an echocardiogram revealed increased RV pressure (estimated at 85 mm Hg) with moderate right atrium enlargement and mild pulmonary regurgitation (Figure 1, echocardiogram in four-chamber view). A diagnostic cardiac catheterization revealed good biventricular function, normal coronary blood flow in both coronary arteries, and no ventricular outflow obstruction. However, there was severe PH with pulmonary vascular resistance (PVR) index of 20 WU m2 with no response to nitric oxide. In addition, there were significant aortopulmonary collaterals arteries, the two largest of which were subsequently coil occluded. The patient was then started on sildenafil and later required the addition of continuous prostacyclin infusion via a central venous access for PH.
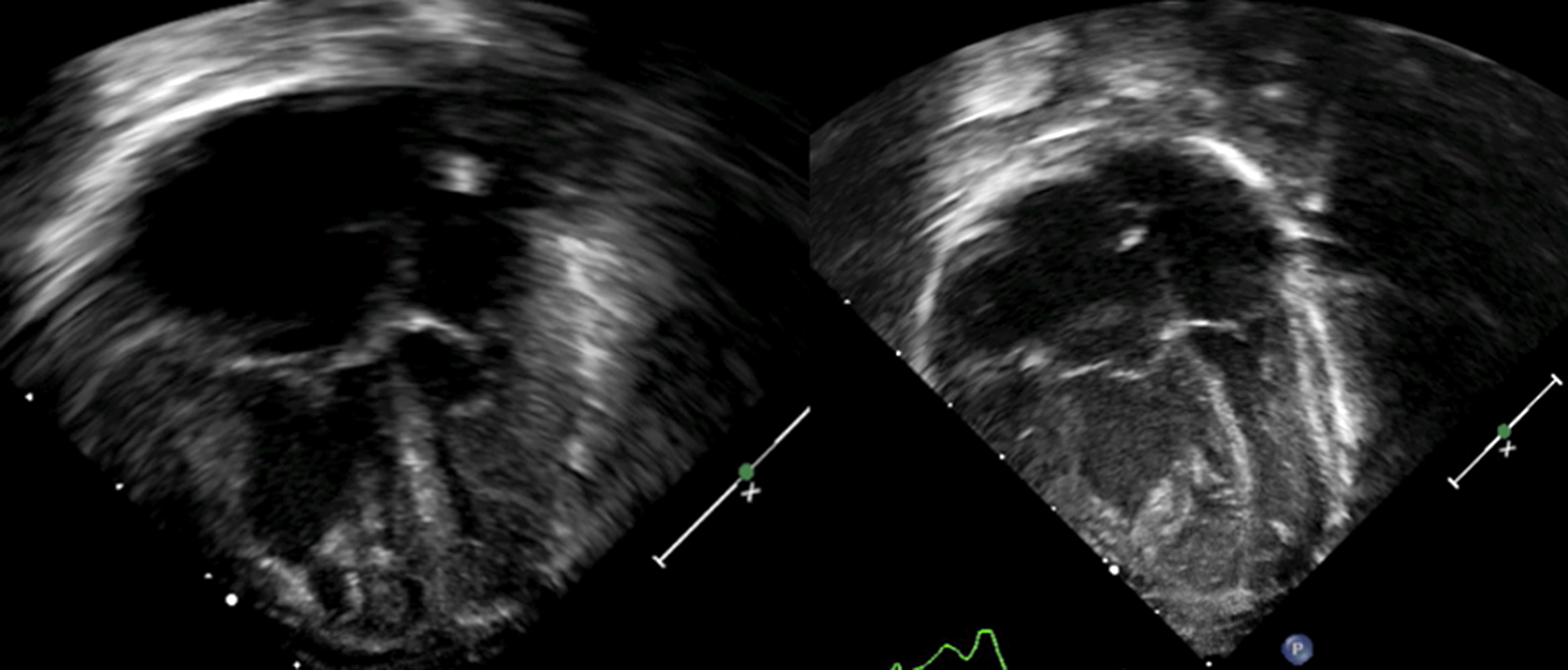
Left, Four-chamber view prior to the ASO repair, notice the ventricular septum with no deviation. Right, At two months of follow-up in clinic, notice the ventricular septum bowing into the left ventricle suggestive of elevated pulmonary pressures. ASO indicates arterial switch operation.
Although he continued to develop appropriately both physically and neurologically, his PVR continued to worsen, and bosentan was added to his regimen at 10 months of age. At 15 months of age, he was readmitted after syncope episodes. At repeat cardiac catheterization, he was found to have suprasystemic PAP (PAP 104/40 mm Hg, arterial blood pressure 80/47 mm Hg, PVR = 24 WU/m2) without any evidence of right ventricular outflow tract obstruction. A palliative interatrial communication was created by trans-septal radio-frequency puncture with balloon dilatation. He was sent home with home oxygen therapy, sildenafil, bosentan, and epoprostenol by continuous infusion. At 28 months of age, he died from hypoxic respiratory failure. Parents denied a request for an autopsy.
Discussion
It was not uncommon for patients with d-TGA to later develop PVOD in the era when the Mustard and Senning atrial switch procedures were widely performed for this condition. 3 –5 Furthermore, it is known that about 40% of untreated patients with d-TGA and ventricular septal defect (TGA/VSD) will develop severe PH within first year of life. 3 However, in untreated patients with simple d-TGA, only 4% of these patients will develop severe PH. 3 This observation led to the hypothesis that highly oxygenated pulmonary blood flow might be the cause of PVOD in this condition. 3 These clinical data were mainly from articles published before 1980. With advances in neonatal cardiac surgery, the ASO has become standard surgical treatment for d-TGA and this is usually done within the first two weeks of life. As a result, PVOD is rarely seen after ASO in the current era. 2
To our knowledge, there are very few reported cases of patients undergoing ASO repair during the neonatal period and later developing severe PVOD, and these cases were all reported before the year 20002,6–8 : In 1998, Rivenes et al reported one infant who underwent ASO at the age of four days and was found to have advanced PVOD at 42 months of age. 2 In 1993, Kumar reported one infant with d-TGA/IVS who had ASO at day 5 but developed persistent low cardiac output after surgery and died 24 hours later. 6 At autopsy, the lung showed Grade 2 PVOD with extensive occlusive intimal proliferation with mild muscular hypertrophy in the preacinar arteries. In 1993, Sreeram et al reported three cases of progressive PVOD after ASO, but all these cases had ASO after six weeks of life. 7 Finally, in 1989, Di Donato reported PVOD in 3 of 62 patients with d-TGA/VSD who had ASO after six months of age. 8 Since neonatal ASO did not protect the patients from PVOD in our case and the two other cases who underwent ASO in the neonatal period, 2,6 we speculate that intrautero developmental or genetic factors may be causally involved in the pathogenesis of PVOD in some patients with d-TGA, or some patients may develop significant PVOD rapidly after birth induced by perinatal or other factors.
The process leading to PVOD in patients with d-TGA remains unclear. Histological studies of the lung specimens from patients with TGA showed abnormal vascular changes including occlusive fibrosis and plexiform lesions as well as micro thrombus. 5 In the same study, patients with d-TGA/IVS had slower progression and with less frequency than patients with ventricular septal defect. Clinically these neonates may experience hypoxia after birth, sometimes with severe acidosis and hemodynamic instability. These stresses may cause hypoxic vasoconstriction, endothelial dysfunction, and activation of platelet and red blood cell factors, which may lead to progression of PVOD. In other situations, PVOD is reported to occur or progress even in infants with simple d-TGA who had minimal PH preoperatively. 3 This challenges the conventional wisdom that PH is usually a consequence of prolonged postnatal pulmonary overcirculation. Thus, one must question whether increased systemic inflammatory reaction and hypoxia during cardiopulmonary bypass may have contributed to the damage to the pulmonary endothelium and pulmonary vascular bed.
Conclusion
Persistent PH and PVOD is a rare complication of simple d-TGA even after neonatal ASO. These patients warrant careful serial follow-up monitoring for progression of PVOD. Further studies are necessary to better understand the pathophysiology of PVOD in neonates with d-TGA, in order to identify a subgroup of patients who are at higher risk of developing progressive PVOD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.