
Abstract
The field of cardiac intensive care continues to advance in tandem with congenital heart surgery. The focus of intensive care unit care has now shifted to that of morbidity reduction and eventual elimination. Acute kidney injury (AKI) after cardiac surgery is associated with adverse outcomes, including prolonged intensive care and hospital stays, diminished quality of life, and increased long-term mortality. Acute kidney injury occurs frequently, complicating the care of both postoperative patients and those with heart failure. Patients who become fluid overloaded and/or require dialysis are at high risk of mortality, but even minor degrees of AKI portend a significant increase in mortality and morbidity. Clinicians continue to seek methods of early diagnosis and risk stratification of AKI to prevent its adverse sequelae. Previous conventional wisdom that survivors of AKI fully recover renal function without subsequent consequences may be flawed.
Keywords
Introduction
The field of cardiac intensive care continues to advance in tandem with congenital heart surgery. The survival of patients with critical congenital heart disease is seldom in question. A protracted stay in the intensive care unit (ICU) after cardiac surgery is a risk factor for developing nosocomial infection and independently predicts late adverse cognitive outcome. 1 Acute kidney injury (AKI) after cardiac surgery is associated with adverse outcomes, including prolonged intensive care and hospital stays, diminished quality of life, and increased long-term mortality. 2 Acute kidney injury occurs frequently, complicating 30% to 40% of adult and pediatric cardiac surgeries. 3,4 Patients who become fluid overloaded and/or require dialysis are at high risk of mortality, 4 but even minor degrees of AKI portend a significant increase in mortality 5 and morbidity. 6
Acute Kidney Injury After Cardiopulmonary Bypass: Why Do We Care, How Do We Find It, and What Are We Going to Do About It?
As survival has improved in congenital heart surgery, more attention has been given to optimizing overall outcome and ensuring long-term well-being. With this, AKI has been increasingly recognized as a common and important complication after pediatric cardiac surgery. 7 Acute kidney injury has been shown to be independently associated with worse clinical outcomes, including longer intensive care and hospital stays, diminished quality of life, and increased long-term mortality. 8 –10 The etiology of AKI after cardiopulmonary bypass (CPB) has many contributing factors including renal ischemia and reperfusion injury, oxidative stress, and maladaptive inflammatory response. 11 All of these factors contribute to global endothelial dysfunction, leading to capillary leak and vasomotor instability. Established risk factors for pediatric cardiac surgery–associated AKI are younger age (neonates) and longer CPB time. 3,7,12 Neonates may be especially vulnerable to developing AKI, given their immature nephron system and the complexity of their cardiac surgeries, which may require long duration of CPB. 7
The study of AKI has been hampered by both the lack of a gold standard for diagnosis and the lack of consensus AKI definitions. 13,14 Traditionally, diagnosis of AKI has relied on elevation in serum creatinine (SCr), which is a late and ineffective method of determining injury, since not only is it nonspecific for kidney injury, but more than 50% of kidney function is lost before it begins to rise. 15,16 Creatinine elevation also represents functional changes in the glomerular filtration rate (GFR), lagging behind actual structural damage that occurs in early AKI. 17 The term “AKI” has also been used indiscriminately to describe injury ranging from a minimal rise in SCr all the way to anuric renal failure. As such, standardization of AKI diagnosis has been a focus of many groups, including the Acute Kidney Injury Network 14 and the Kidney Disease: Improving Global Outcomes initiative. 18
An AKI framework has been proposed, demonstrating its clinical continuum and highlighting areas for improved diagnosis and targeted intervention. 17 When functional injury occurs, biomarkers such as SCr or cystatin C become elevated. Preceding this stage is “kidney damage,” an intermediate state during which structural damage occurs without overt functional injury. Detection of injury at this stage is the focus of structural biomarkers such as neutrophil gelatinase–associated lipocalin (NGAL), interleukin 18 (IL-18), and more recently the cell cycle arrest biomarkers tissue inhibitor of metalloproteinase 2 (TIMP-2) and insulin-like growth factor binding protein 7 (IGFBP7). It is during this stage that potentially reversible changes can be detected. However, once functional injury has set in, more severe and irreversible changes, such as cell death and desquamation, occur. Although tubular cells do possess the ability to regenerate and repair after injury, interventions initiated at this stage have been largely unsuccessful.
Conventional urinary biomarkers such as casts, fractional excretion of sodium, or filtered tubular proteins are insensitive and nonspecific for the early recognition of AKI. The application of innovative technologies such as functional genomics and proteomics has uncovered several novel genes and gene products that are emerging as AKI biomarkers. 19,20 The most promising to date are NGAL, IL-18, liver fatty acid–binding protein (L-FABP), kidney injury molecule 1 (KIM-1), and, more recently, biomarkers of cell cycle arrest: TIMP-2 and IGFBP7.
Neutrophil gelatinase–associated lipocalin is a siderophore-binding protein normally expressed at low concentrations in the kidney, trachea, lungs, stomach, and colon. It has been identified as one of the earliest and most robustly induced proteins in the kidney after ischemic or nephrotoxic injury and is easily measured in plasma or urine very early after injury. 21 Validation studies have shown that, in AKI, NGAL is markedly upregulated within the two hours after the start of CPB, with high sensitivity and specificity, particularly in the relatively homogenous pediatric population. 3,12,22 Elevations in NGAL also occur with other forms of kidney injury, such as contrast nephropathy, nephrotoxic injury, and transplant graft dysfunction. 15,23 Neutrophil gelatinase–associated lipocalin has been shown to be a predictor of clinical outcomes such as hospital and ICU stays, duration of AKI, duration of mechanical ventilation, dialysis requirement, and mortality. 3,10,12,22 A potential therapeutic role of NGAL targeting renal tubule survival and recovery through its role of iron transportation is an area of ongoing research. 24 Although NGAL is arguably the most promising biomarker to date, it is most sensitive and specific in uncomplicated populations, and measurements may be influenced by a number of coexisting variables, such as preexisting renal disease and systemic or urinary tract infections. 25
Interleukin 18 is a proinflammatory cytokine induced and cleaved in the proximal tubule. Interleukin 18 is specifically elevated with renal tubular injury and functions to induce ischemic tubular necrosis through the initiation of apoptosis. 26 Urinary IL-18 is more specific to ischemic injury and is largely unaffected by nephrotoxins or urinary tract infections. 26 In pediatric models, this biomarker is elevated in urine as early as four to six hours postbypass and can be used to predict the duration of AKI. 10,27 Plasma IL-18 is less specific and may be increased in various pathophysiologic states.
Liver fatty acid–binding protein is an intracellular carrier protein that is expressed in proximal renal tubular cells and is involved in the transport of intracellular long-chain fatty acids. Ischemia induces free fatty acid overload in the proximal tubule, leading to increased secretion and decreased reabsorption of L-FABP. Urine L-FABP has been demonstrated to increase stepwise in worsening renal injury with early detection at four to six hours after CPB although with less sensitivity and specificity than other biomarkers. 10,28 Liver fatty acid–binding protein is also abundantly expressed in the liver, and urinary L-FABP may be influenced by serum L-FABP levels.
Kidney injury molecule 1 is a transmembrane glycoprotein expressed in proximal tubule epithelial cells and upregulated at times of kidney injury due to the increased production of epithelial cells. 29 Elevation at 12 to 24 hours after CPB has been shown to be predictive of worsening degrees of AKI, longer ventilation, and longer duration of AKI. 10 Kidney injury molecule 1 is felt to be the most specific biomarker, as no systemic source of KIM-1 has been described. 30 However, in addition to ischemia, KIM-1 can be induced by a number of injury mechanisms, including nephrotoxins and inflammatory states. 31
Both TIMP-2 and IGFBP7 are cell cycle arrest biomarkers that are expressed in tubular cells and in injury stimulate p proteins, which results in G1 cell cycle arrest. They have been shown to be elevated very early after ischemia. 32,33 Urinary levels are typically expressed as a product of the two biomarkers (TIMP-2 • IGFBP7). A recent study in pediatric patients with CPB demonstrated a marked increase in TIMP-2 • IGFBP7 at four hours after CPB. 34 A rise in these biomarkers significantly strengthened risk prediction when added to a clinical risk model. The measurement of the cell cycle arrest biomarkers is clinically available, with the newly US Food and Drug Administration–approved NephroCheck (Astute Medical, San Diego, CA, USA), the first point-of-care device approved for kidney injury biomarker testing. The approval of this device is an important milestone in AKI research. Table 1 summarizes the currently available biomarker assays.
Key Biomarkers and Sample Assays Available for Testing and Current Commercial Availability.
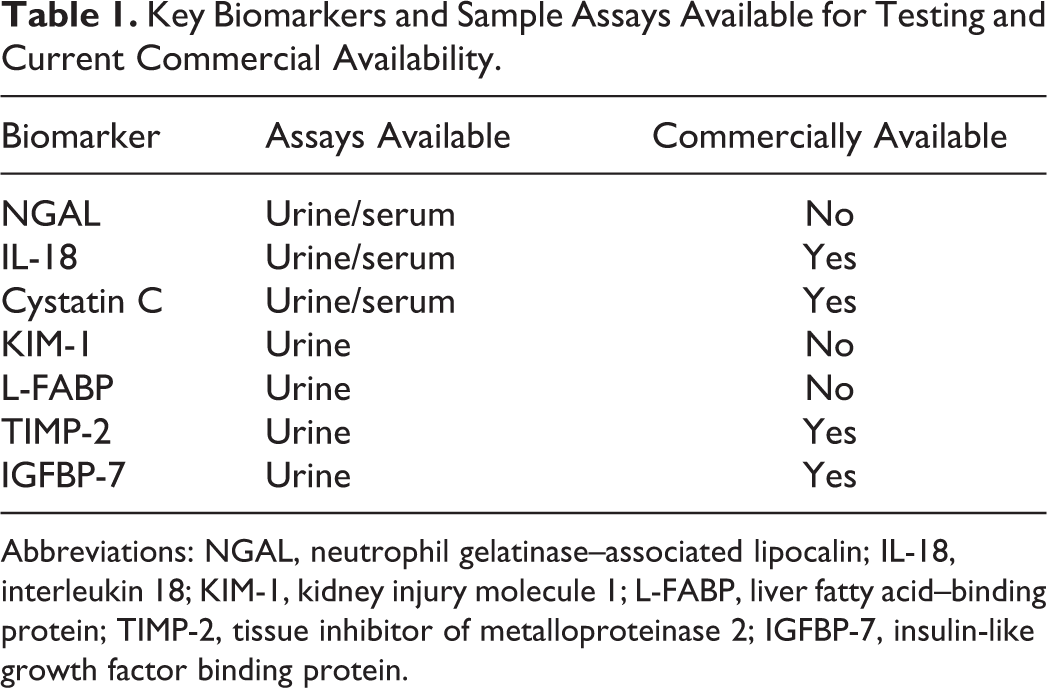
Abbreviations: NGAL, neutrophil gelatinase–associated lipocalin; IL-18, interleukin 18; KIM-1, kidney injury molecule 1; L-FABP, liver fatty acid–binding protein; TIMP-2, tissue inhibitor of metalloproteinase 2; IGFBP-7, insulin-like growth factor binding protein.
Since many pathways are involved in the pathogenesis of AKI, it is believed that combinations of biomarkers with different properties might prove most predictive. 10,27 In a recent study of biomarker combinations in pediatric CPB, the addition of a urine biomarker “panel,” consisting of NGAL, IL-18, L-FABP, and KIM-1, to a clinical model enhanced the prediction of AKI at 6 to 24 hours after surgery. 10 In this study, biomarkers rose in a predictable pattern in AKI, with significant NGAL elevations at 2 hours, IL-18 and L-FABP at 6 hours, and KIM-1 at 12 hours after CPB. The temporal sequence of biomarkers correlates with the phases of AKI and can be used to focus potential therapies. In the initiation phase during the ischemic insult, intracellular ATP depletion is profound, and generation of reactive oxygen molecules and labile iron is initiated. Vasodilator, ATP donor, antioxidant, and iron chelation therapies may be effective during this phase, and the appearance of NGAL may be used to guide such therapies. The extension phase is characterized by the prolongation of ischemia followed by reperfusion. Tubules undergo cell death and the injured endothelial and epithelial cells amplify the inflammatory cascades. This phase may be identified by the rise in biomarkers such as L-FABP and IL-18 and point to therapeutic intervention with antiapoptotic and anti-inflammatory strategies. During the maintenance phase, cell injury and regeneration occur simultaneously. Measures such as growth factors and stem cells, which accelerate the regeneration processes identified by later biomarkers such as KIM-1, may be most effective during this phase. The future use of “biomarker panels” will likely allow us to pinpoint the timing of injury and assist in selecting appropriate therapies. Table 2 summarizes the major studies looking at kidney biomarkers among pediatric cardiac patients.
Major Studies Looking at Kidney Biomarkers Among Pediatric Cardiac Patients.
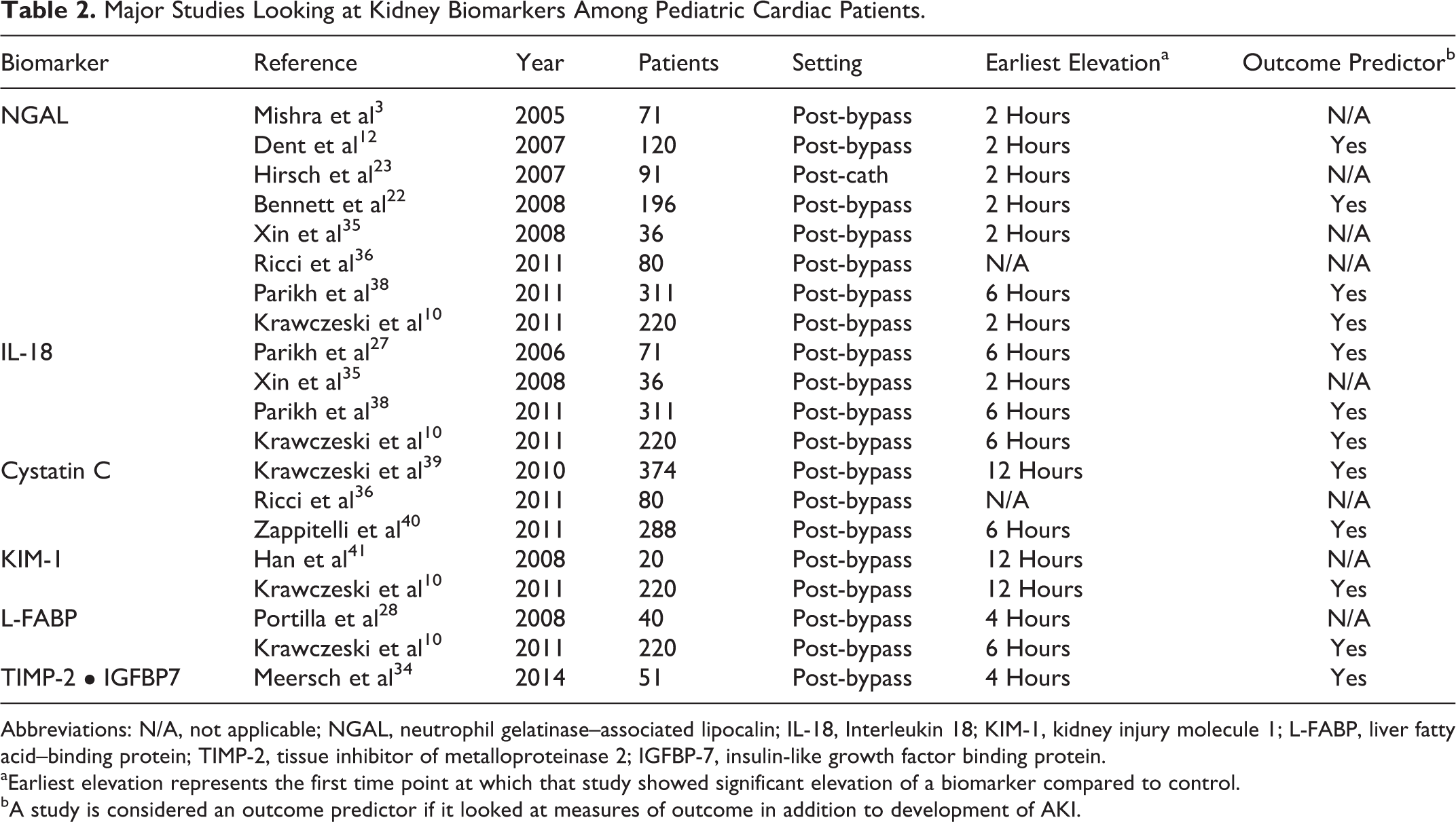
Abbreviations: N/A, not applicable; NGAL, neutrophil gelatinase–associated lipocalin; IL-18, Interleukin 18; KIM-1, kidney injury molecule 1; L-FABP, liver fatty acid–binding protein; TIMP-2, tissue inhibitor of metalloproteinase 2; IGFBP-7, insulin-like growth factor binding protein.
aEarliest elevation represents the first time point at which that study showed significant elevation of a biomarker compared to control.
bA study is considered an outcome predictor if it looked at measures of outcome in addition to development of AKI.
Although recently discovered biomarkers, most notably NGAL, have been validated as a superior mechanism of diagnosing AKI earlier than current modalities, little has been done to demonstrate clinical translation of these studies. Although animal data are abundant, there is currently no study, which demonstrates that clinical outcomes can be improved by earlier AKI diagnosis. Prospective studies that demonstrate improved outcomes with early, targeted therapy are needed. Additionally, since the majority of pediatric AKI studies have been performed in cardiac surgical patients, it is important to confirm results in populations with other mechanisms of kidney injury.
Fluid Overload: Ubiquitous and Problematic
Fluid accumulation occurs frequently in critically ill patients. Problematically, data from the adult and pediatric intensive care unit populations suggest that fluid overload (FO), particularly in mechanically ventilated patients, is associated with prolonged duration of ventilator support, higher risk of infection, longer hospital stay, and a high incidence of mortality. 42 –44 These trends mirror the associations of AKI with critical illness. Results from the Fluid and Catheters Treatment Trial suggest that higher fluid balance, seen in liberal resuscitation strategies, are associated with fewer ventilator-free days and longer ICU length of stay. 45 In pediatrics, increasing FO denoted as percentage is measured as Fluid in − Fluid out (mL)/Admit Weight and is similarly associated with prolonged mechanical ventilation and higher risk of in-hospital death. 46 There is a linear relationship between rising %FO and oxygenation index in mechanically ventilated patients. 42,43 The prospective pediatric continuous renal replacement therapy (CRRT) registry discovered over a period of 10 years and in nearly 400 patients that every 1% fluid increase at the time of RRT initiation was associated with a 3% increase in mortality. 47,48
Fluid overload following cardiac surgery is a silent killer. Although protocol-driven fluid removal is not a standard practice, the routine approach to dealing with early fluid accumulation is observation and, at an arbitrary point of time, initiation of diuretics. As FO tends to be transient, cardiac intensivists may argue that FO in the post-CPB population is common and inconsequential. The data suggest otherwise. Recent evidence suggests that early FO following bypass is associated with higher ventilation pressure requirements, fewer ventilator-free days, higher rates of infection, and increased mortality rates. 49 Further, a direct relationship exists between the time required to reach negative fluid balance, the corollary of high immediate postoperative fluid balance, and risk of poor outcome. 50 Table 3 summarizes the outcome of FO in critically ill children.
Fluid Overload is Associated With Poor Outcome for Critically Ill Children.
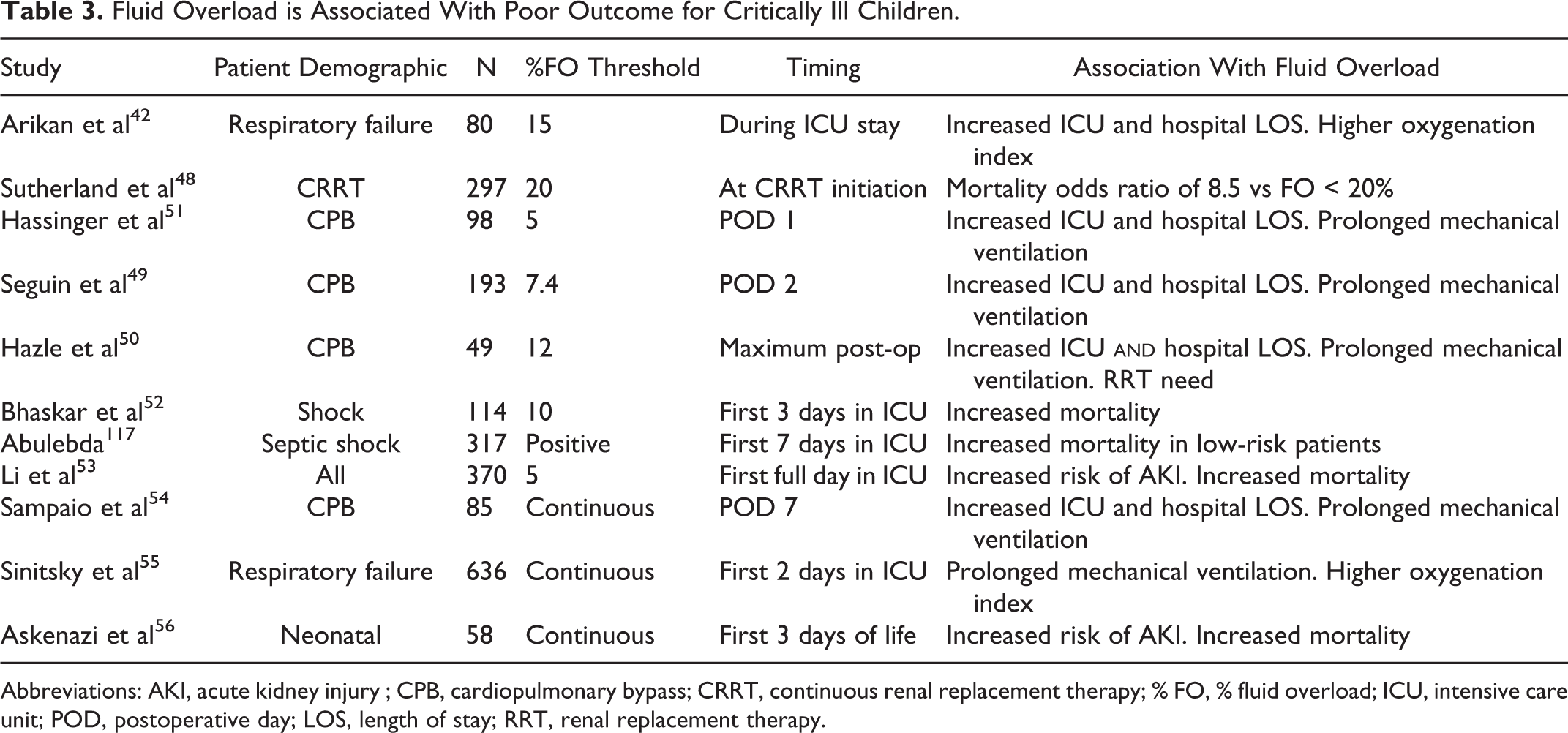
Abbreviations: AKI, acute kidney injury ; CPB, cardiopulmonary bypass; CRRT, continuous renal replacement therapy; % FO, % fluid overload; ICU, intensive care unit; POD, postoperative day; LOS, length of stay; RRT, renal replacement therapy.
Taken together, FO is a problem for cardiac surgery patients. Acute kidney injury is a clear risk factor for the accumulation of fluid. Interestingly, correction of SCr for degree of FO “unmasks” a higher incidence of AKI than previously estimated. 57 In small children undergoing corrective or palliative cardiac surgery, accounting for the dilutional effect of fluid on SCr may further support the negative associations between AKI, FO, and poor outcome. 58
Risk Stratification: The Renal Angina Index
Capricious use of biomarkers limits their utility. As described earlier, the traditional markers of kidney injury, SCr, and urine output (UOP) are limited in their sensitivity to injury, particularly in pediatric patients. Recent epidemiologic data suggest, however, that even early and small changes in SCr are associated with progression to severe AKI and poor outcome. Novel biomarkers for AKI such as NGAL, IL-18, L-FABP, and IL-18 offer exciting potential to be both sensitive and specific for AKI in the early phases of injury—potentially being the equivalent of a renal “troponin.” Unfortunately, AKI does not share a very useful clinical sign aiding detection of acute coronary syndrome. Simply stated, AKI does not hurt. 59,60 While the novel biomarkers perform exceptionally well in the population with CPB, all relatively clean of comorbidities and with a known timing and duration of injury, few have demonstrated robust efficacy in children with heterogeneous illness when tested in isolation. These biomarkers need context to be truly useful.
In response to the need of risk stratification, we proposed the renal angina clinical model. 61 The renal angina index (RAI), operationalizing the renal angina concept, is a numeric and easy to calculate the composite of clinical risk factors and early evidence of kidney dysfunction. 37 Using the RAI, biomarkers are directed toward the use in the most optimal patients—enhancing their utility. This model is akin to directed assessment of troponin I only in select patients with chest pain. Troponin tested in adults with critical illness, and not only chest pain and risk factors of heart disease, loses efficacy. 62 –64 The clinical incorporation of cardiac angina to identify patients in whom troponin testing is useful is modeled and quantified in kidney injury by the RAI. This model seeks a high negative predictive value (NPV) for AKI of not fulfilling renal angina. Further, unlike difficult to use, severity of illness scoring systems, which merely score existing injury, fulfillment of renal angina aids prediction of severe AKI. We have demonstrated that the RAI carries a superior discrimination for severe AKI versus any of the novel biomarkers in isolation, and RAI prediction improves after the incorporation of biomarkers. 65 This “targeting” of biomarker testing demonstrates a methodology to optimize the utility of novel diagnostics.
Improving the Precision of AKI Diagnosis: Biomarker Combinations for AKI Phenotype
Traditional nomenclature for classification of AKI is imprecise. Trainees are indoctrinated with the teaching of AKI as being “prerenal,” “intrinsic renal,” or “postrenal.” These descriptors are subsequently defined as simultaneous as reference for etiology, location, and duration of injury as well as suggestive of therapy. 66,67 For example, the classification of “prerenal” is often synonymous with AKI secondary to poor glomerular perfusion, that is, renal ischemia. Prerenal AKI is defined as transient, at the level of the glomerulus, and responsive to volume. A widened ratio between the blood urea nitrogen (BUN) and SCr is used to identify prerenal AKI. However, although a patient with hypovolemia from gastroenteritis and a patient with congestive heart failure may both have prerenal AKI defined by high BUN/SCr, their AKI is not the same and certainly would not and should not be treated in similar fashion. The 10th Acute Dialysis Quality Initiative (ADQI-X) consensus meeting recommended changing the nomenclature of injury from the previous designations to more pathophysiologic descriptions (functional and damage-associated/tubular AKI). 67,68
Novel biomarkers offer the opportunity to improve the granularity of AKI diagnosis. Biomarkers can be classified as representative of the location of injury within the nephron. 69 Additionally, as we mentioned earlier, the temporal profile of biomarkers in response to injury can vary and be indicative of different characteristics of AKI timing. The ADQI-X group recommended biomarkers be used in combination to identify AKI that is functional, damage associated, or both. We recently operationalized AQDI-X in a cohort of nearly 350 children after CPB and demonstrate the ability of novel biomarker combinations to improve the precision of AKI diagnosis. 70 Denoted as “positive” by exceeding derived cutoff values, combinations of the values of the functional biomarker plasma cystatin C and the damage marker urinary NGAL measured two hours after the start of CPB were superior to changes from baseline in SCr for the prediction of the development, severity, and duration of AKI. Remarkably, a combination of “positive cystatin C and negative uNGAL” offered the ability to identify functional and transient AKI to a significantly greater extent than any change in SCr. Incorporation of other biomarkers, such as the cell cycle arrest markers IGFBP7 and TIMP-2, into the biomarker combinations offers even more potential to heighten the classification of injury. 33 These findings are important both diagnostically but potentially therapeutically as well. Biomarker combinations may identify patients with certain AKI phenotypes facilitating testing of targeted AKI therapy.
Quantitative Assessments of Function: The Furosemide Stress Test
For practitioners caring for critically ill patients, tests reflecting real-time organ function are practical and needed. Although SCr and UOP, and novel biomarkers, reflect damage, they are poorly reflective of real-time kidney function. Real-time markers of GFR, such as serum inulin, would be a valuable adjunct to clinical management for patients at risk of or with AKI, however the measurement of such markers is laborious and impractical. However, a practical metric of kidney function might enhance biomarker performance.
A functional assessment of renal tubular injury is a valuable piece of clinical information. Furosemide, a loop diuretic, is often used as a first-line agent to help fluid removal. Interestingly, furosemide may not only be a therapy but a test of function. Furosemide is incompletely filtered at the level of the glomerulus and relies on proximal tubular cells for access to the tubular lumen and loop of Henle tubular cells for function to affect natriuresis. Therefore, a poor response to furosemide may actually be indicative of tubular damage. The furosemide stress test (FST) was therefore developed as a method to assess the integrity of the renal tubule during early AKI. 71,72 In 77 adult patients with early AKI, urine flow rates measured in the FST were highly predictive of progression to severe AKI. Further, FST outperformed any novel biomarker for prediction of the progression. Together, FST or other methodology able to identify renal function would be important in the management of AKI and FO in critically ill patients.
Cardiorenal Syndrome in Children With Heart Failure
Renal injury occurs commonly in patients with heart failure. Although the mechanisms are not fully understood, diminished cardiac function coupled with renal dysfunction, or the cardiorenal syndrome, has been observed in both the acute and the chronic care settings. Decreased UOP and resultant fluid retention can aggravate heart failure symptoms and contribute to clinical deterioration. Several studies have demonstrated the prognostic importance of increasing SCr concentrations for predicting morbidity and mortality in adult patients with heart failure. 73 –77 Among patients hospitalized for acute decompensated heart failure, worsening renal function (WRF) is associated with longer length of stay, higher in-hospital costs, and an increased risk of in-hospital mortality. 78 Even a modest increase in SCr (ie, >0.3mg/dL) can predict mortality in patients hospitalized for heart failure. 79 Similarly, asymptomatic patients with renal injury and left ventricular dysfunction are also at risk of pump failure and death. 80
The relationship of renal function and heart failure in children has not been well examined. Retrospective data have shown a high incidence of cardiac disease among children who develop renal insufficiency while hospitalized, and anecdotal experience suggests that like adults, WRF is associated with poor outcomes in children with heart failure. 81 A prospective study of children admitted to an intensive care unit with a wide range of diseases found a low incidence of AKI but a strong association with all-cause mortality. 82 That study, however, included all children admitted to a pediatric intensive care unit. An observational study of children admitted to an ICU who required mechanical ventilation and at least one vasoactive medication found a high prevalence of AKI (82%) and increased mortality among children with more severe AKI. 83 These studies further demonstrate our lack of understanding of the cardiorenal relationship, as cardiovascular dysfunction was found to be both a risk factor for and a complication of acute renal failure.
The largest study examining combined heart failure and renal dysfunction in children described the prevalence of WRF in 73 consecutive patient hospitalizations with a primary diagnosis of acute decompensated heart failure. 84 Worsening renal function was defined as an increase in SCr of ≥0.3mg/dL at any time during hospitalization. Renal failure at the time of admission was uncommon in this cohort, but SCr subsequently increased in 82% and WRF occurred during 48% of hospitalizations. These data are consistent with reports in adults with left ventricular systolic dysfunction and congestive heart failure. 85,86 Using the same SCr minimum increase of 0.3mg/dL, Gottlieb et al 76 reported a similar frequency of WRF in adults of 39%. In this cohort of children, WRF was found to be an independent predictor of death or the need for mechanical circulatory assistance during hospitalization and was associated with a longer observed length of stay.
The physiologic interaction of the heart and kidney is complex and not well understood. Renal insufficiency occurring in patients with heart failure is usually attributed to diminished cardiac output and renal perfusion or a prerenal state. This explanation of concomitant cardiorenal dysfunction oversimplifies the complex interrelationship of these two organs and fails to acknowledge the neurohormonal and vasoreactive elements of decompensated heart failure.
Arterial underfilling causes decreased baroreceptor activation in the left ventricle, carotid sinus, and afferent arterioles of the kidney. 87 Signals from the brain then activate efferent sympathetic nervous system pathways, which provoke upregulation of the neurohormonal system. The sympathetic nervous system’s direct vasoconstrictive stimulation of the peripheral vasculature and renal arteries as well as activation of the renin–angiotensin–aldosterone system and arginine vasopressin serves as an adaptive mechanism for restoring blood pressure and vascular volume. Over time, these adaptive mechanisms become maladaptive, leading to elevated systemic vascular resistance, FO, and decreased renal perfusion.
Additional factors such as persistent or aggravated systemic vasoconstriction, use of potentially nephrotoxic drugs, such as nonsteroidal anti-inflammatory drugs and angiotensin-converting enzyme inhibitors, contrast agents, renal artery stenosis, infection, or renal vein hypertension can lead to AKI during the treatment of heart failure. 88 Elevated filling pressures also play an important role. High central venous pressure is associated with reduced GFR even while other hemodynamic measurements (cardiac output and mean arterial pressure) are preserved. 89,90
Renal Replacement Therapy in the Cardiac Intensive Care Unit
The risk factors associated with the development of AKI after CPB include preoperative factors (hypotension, use of diuretics, ACE inhibitors, and need for ventilator support), intraoperative factors (hemodynamic changes during surgery, aortic clamp time and inflammatory response to CPB), and postoperative factors (cardiac output and hypotension). After cardiac surgery, patients of a young age, the presence of preexisting renal dysfunction, complex cardiac lesions, prolonged CPB, circulatory arrest, postoperative low cardiac output syndrome, central venous hypertension, hypotension, and hypoalbuminemia are also risk factors for the development of AKI.
The conservative management of AKI and its consequences are through the use of diuretics, most commonly furosemide ± chlorothiazide, in hopes of increasing UOP, improving fluid balance, and permitting the delivery of appropriate fluid (including nutrition) to the patient. However, in the setting of AKI, most ICU patients receive diuretics, but there has been no improvement in clinical outcomes. 91 The decision to initiate RRT is based on the presence of refractory electrolyte abnormalities, prevention/treatment of FO, or the need to provide adequate nutritional support or other large volume therapies. The choice of RRT modality, intermittent hemodialysis, peritoneal dialysis, or CRRT is based on physicians’ beliefs, patient characteristics, the goal of the therapy, and the availability of equipment, staff expertise, and cost.
The lack of consensus regarding the timing of initiation of RRT is most likely related to the uncertainty of success of standard therapy and the difficulty/inexperience with RRT in cardiac infants. Timing of RRT that is “early” or “late” has been defined either based on the time from ICU admission to CRRT initiation or on the severity of biochemical abnormalities present at CRRT initiation. In the Project to Improve Care of Acute Renal Disease (PICARD) study, Liu and colleagues found a better survival when RRT was initiated with a BUN < 73 mg/dL (P < .0001) and when CRRT was the initial RRT modality (P < .0001). 92
In the pediatric literature, there are no data regarding the timing of initiation of RRT based on a BUN level. Instead, in the last decade, we have recognized FO as an independent predictor of mortality in pediatric patients with AKI. Accordingly, this is the most common indication for initiation of RRT in pediatric patients. 93 Additionally, multiple studies have demonstrated that earlier initiation of RRT is associated with improved outcome. 48,94,95
Previously, peritoneal dialysis was reserved for patients who developed AKI and FO who did not respond to fluid restriction and diuretics. 96 –98 However, early initiation of peritoneal dialysis, particularly in infants at high risk of developing AKI after CPB, is now widely used to prevent FO. 99 –102 Kwiatkowski and colleagues demonstrated that use of a peritoneal dialysis catheter (even without active dialysis) was associated with earlier negative fluid balance, earlier extubation, reduction in inotrope requirements, and fewer electrolyte imbalances requiring correction. 103 Given the relative ease of placement and rare incidence of complications, this may prove to be a viable strategy to prevent FO in infants at high risk of AKI.
Long-Term Outcomes of Pediatric AKI
It was previously assumed that patients with a single episode of AKI would recover kidney function without long-term consequence. However, during the last decade, epidemiologic data from critically ill children 104 and adults 105,106 with AKI suggest that survivors are at considerable risk of developing chronic kidney disease (CKD). Obstacles to assessing for a potential AKI to CKD link have included lack of a standard pediatric AKI definition and reliance on SCr as the main biomarker to detect and diagnose AKI and CKD. The development of standardized AKI definitions has allowed for a more complete understanding of pediatric AKI epidemiology, but long-term renal clinical outcomes after AKI in critically ill children and neonates have not been well established.
Animal models first demonstrated the potential long-term consequences of AKI on kidney function. In these models, substantial damage to renal tubular and endothelial cells, including vascular injury, vascular dropout, and tubulointerstitial fibrosis, has been observed following ischemia–reperfusion injury. Vascular dropout and injury, which negatively affects endothelial cell differentiation and regenerative capacity, is thought to contribute to progressive CKD. 107 The damage induced by subclinical or manifested episodes of AKI may, in fact, produce irreversible loss of renal mass with deleterious effects on overall renal function. Clinically, this has been seen in long-term studies of adult patients, which show that those who survive an episode of AKI are at considerable risk of progressing to CKD. 105,108 In follow-up studies of pediatric AKI, the incidence of CKD ranges from 27% to 67%. 104,109 Coca and colleagues 110 showed in a meta-analysis that adults with all-cause AKI compared to those without AKI have a ninefold increased risk of developing CKD, a threefold increased risk of developing end-stage kidney disease, and a twofold increased long-term mortality risk. Mammen and colleagues examined the long-term risk of CKD in critically ill children with AKI and no preexisting CKD and found that 10% of children had developed CKD and almost half of the children were at risk of CKD. 111 However, the implications of post-CPB AKI are less clear.
Given the known limitations of traditional biomarkers to detect AKI early, attention has been focused on the utility of urinary biomarkers, such as NGAL, KIM-1, IL-18, and L-FABP, to not only improve AKI diagnosis but also follow and predict rapid CKD progression in both pediatric and adult CKD populations. Production of NGAL is significantly upregulated in the kidney after ischemic and nephrotoxic injury and may play a primary role in renal tubular survival and recovery via preservation of function, attenuation of apoptosis, and an enhanced proliferative response. 21 Kidney injury molecule 1 is a transmembrane protein that is overexpressed in dedifferentiated proximal tubule cells after ischemic or toxic injury. 29 Preliminary studies have reported on the potential utility of KIM-1 as a CKD biomarker. 112,113 Animal models of AKI-to-CKD transition have identified NGAL and KIM-1 as two of the most upregulated genes and proteins in the kidney, revealing a possible role for these proteins as potential biomarkers to predict risk of CKD following AKI. 114 While KIM-1 in the setting of AKI has been postulated to be protective, there is evidence for its role in the chronic injury as seen in CKD. 115 Inflammation is postulated as another mechanism for ongoing kidney injury, as CKD is associated with a chronic inflammatory process. Both IL-18 and L-FABP are urinary biomarkers whose production is more specific toward inflammatory pathophysiology within the renal environment. Interleukin 18 is a mediator of inflammation produced by the proximal tubules and appears to be more specifically upregulated following ischemic AKI 26 —a common mechanism for CPB-AKI. Liver fatty acid–binding protein, an inflammatory proximal tubular protein upregulated after a variety of acute kidney injuries 28 as well as in the setting of CKD, has been postulated to represent an endogenous antioxidant capable of suppressing tubulointerstitial damage in the kidney parenchyma. 116 Kamijo and colleagues showed that in a group of patients with nondiabetic CKD, L-FABP levels were significantly higher in the group of patients with mild CKD, with a more rapid rate of significant CKD progression. 118
The difficulty in utilizing classic signs of CKD, such as proteinuria and elevated creatinine, may be explained by changes in renal functional reserve (RFR) following AKI exposure. The concept of RFR is an indirect method of measuring renal mass by assessing how well the kidney can metabolically compensate under metabolic “stress.” Renal functional reserve is measured by the difference in the GFR before (baseline) and then following administration of a protein load (GFRmax). 119 Following an episode of AKI, there is likely variable injury to functional renal mass and RFR, increasing the risk of CKD development. Likewise, patients who experience AKI probably have reduced RFR, but given the kidney’s ability to sufficiently compensate for reduced renal mass, routine assessments of renal function in a normal physiologic, “nonstressed” state might not adequately reflect the actual anatomical and functional limitations of the kidney parenchyma.
With regard to AKI, Haase and colleagues demonstrated that patients with elevated NGAL levels but normal SCr (subclinical AKI) had a similar risk of adverse outcome in patients with elevated creatinine alone (manifest AKI). 120 Assessment of the prevalence of renal dysfunction in adults with congenital heart disease (mean age 36 years) found that 50% of the patients had some form of impaired GFR, even in patients classified with “simple” defects. 121 As in those with AKI, biomarker positivity during long-term follow-up in the absence of an elevated creatinine may portend a poor prognosis. Despite the growing evidence showing a strong association between AKI and CKD, further work is required to better understand the relationship between AKI and CKD in children following cardiac surgery utilizing CPB. Novel biomarkers of kidney injury measured at different times in the course of AKI might help risk stratify those who will progress to CKD. Likewise, clinical trials are needed to determine whether therapy aimed at attenuating or preventing AKI might decrease the future development of CKD. Previous conventional wisdom that survivors of AKI fully recover renal function without subsequent consequences may be flawed. Centers should consider long-term follow-up (at least annually) for patients with first episodes of AKI, even if they present with “normal kidney function.”
Conclusion
The reduction in morbidity following cardiac surgery remains challenging. Recent insights have allowed us to recognize the impact of perioperative AKI as a significant contributor to morbidity and mortality. Emerging science has provided promising novel biomarkers for AKI, with potentially high sensitivity and specificity that should facilitate early interventional trials to prevent or attenuate the effects of AKI. Adopting a strategy of anticipation, early recognition and aggressive prevention and/or treatment of AKI and FO should result in a decline in morbidity.
Medical therapies for the prevention and treatment of AKI and FO continue to evolve. It remains challenging to determine when medical therapy for AKI “fails.” The lack of consensus regarding the timing of initiation of RRT is most likely related to the lack of a standardized definition of AKI.
However, it is clearly recognized that FO is an independent predictor of mortality in pediatric patients with AKI, and improvement in survival and morbidity are seen when RRT is initiated early. The optimal delivery of RRT, particularly in the smallest of patients, remains a challenge, but peritoneal dialysis holds promise as both a prevention and a treatment strategy. There is growing evidence showing a strong association between AKI and CKD. Novel biomarkers of kidney injury measured at different times in the course of AKI might help risk stratify those who will progress to CKD. Previous conventional wisdom that survivors of AKI fully recover renal function without subsequent consequences may be flawed. Centers should consider long-term follow-up for patients with first episodes of AKI, even if they present with “normal kidney function.”
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.