
Abstract
Background:
High-fidelity simulation using patient-specific three-dimensional (3D) models may be effective in facilitating pediatric cardiac intensive care unit (PCICU) provider training for clinical management of congenital cardiac surgery patients.
Methods:
The 3D-printed heart models were rendered from preoperative cross-sectional cardiac imaging for 10 patients undergoing congenital cardiac surgery. Immediately following surgical repair, a congenital cardiac surgeon and an intensive care physician conducted a simulation training session regarding postoperative care utilizing the patient-specific 3D model for the PCICU team. After the simulation, Likert-type 0 to 10 scale questionnaire assessed participant perception of impact of the training session.
Results:
Seventy clinicians participated in training sessions, including 22 physicians, 38 nurses, and 10 ancillary care providers. Average response to whether 3D models were more helpful than standard hand off was 8.4 of 10. Questions regarding enhancement of understanding and clinical ability received average responses of 9.0 or greater, and 90% of participants scored 8 of 10 or higher. Nurses scored significantly higher than other clinicians on self-reported familiarity with the surgery (7.1 vs 5.8; P = .04), clinical management ability (8.6 vs 7.7; P = .02), and ability enhancement (9.5 vs 8.7; P = .02). Compared to physicians, nurses and ancillary providers were more likely to consider 3D models more helpful than standard hand off (8.7 vs 7.7; P = .05). Higher case complexity predicted greater enhancement of understanding of surgery (P = .04).
Conclusion:
The 3D heart models can be used to enhance congenital cardiac critical care via simulation training of multidisciplinary intensive care teams. Benefit may be dependent on provider type and case complexity.
Keywords
Introduction
Three-dimensional (3D) printing technology is rapidly expanding in usage and application in the medical field. Analogous to developments in 3D imaging, including cross-sectional and 3D echocardiographic images, 3D-printed cardiac models offer a high-fidelity representation of complex 3D structure that is generally more readily understood by the user. Specific to cardiovascular surgery, the value of 3D models of the heart has been demonstrated for preoperative planning, 1 –3 transcatheter procedural planning, 4,5 anesthesia management, 6 and clinician training. 7,8 The 3D printing can produce high-fidelity, hands-on models of complex human anatomy, allowing for the design of simulation-based training programs utilizing these models to prepare intensive care clinicians for postoperative management of rare congenital cardiac anomalies and postsurgical structural changes. 9,10 Postoperative critical care following congenital heart surgery necessitates a multidisciplinary team of caregivers, each providing different perspectives and expertise to complex clinical cases. Following surgery, transfer of patient care to the pediatric cardiac intensive care unit (PCICU) relies heavily on communication from the operating team to the critical care team who are often less familiar with the anatomical nuances of the individual patient anatomy. Harnessing the benefit of 3D models in simulation of potential postoperative complications can enhance PCICU conceptualization by the nonoperative team; however, clinicians with different backgrounds and levels of expertise may receive dissimilar benefits from the same conveyance of structural detail. Furthermore, the complexity of surgical cases may influence the benefit received from 3D model simulation. Here we evaluate the effects of clinician expertise and case complexity on application of 3D model “Just-In-Time” postoperative care simulation training in a PCICU setting.
Materials and Methods
With Institutional Review Board approval, 10 consecutive congenital cardiac surgery cases were selected for 3D-printed cardiac model-based simulation training. Deidentified images were obtained in Digital Imaging and Communications in Medicine (DICOM) format from each patient’s preoperative radiographic images (either magnetic resonance imaging or computed tomography scan). Mimics Innovation Suite software (Materialise HQ, Leuven, Belgium) was used to visualize and segment the images. The heart was isolated and segmented to create a 3D digital model. An in-house Objet500 Connex 3D polyjet printer (Stratasys Ltd, Eden Prairie, Minnesota) was used to print the 3D heart models. Material costs for the opaque rigid plastic materials were approximately US$200 per model (Figure 1). Time interval for segmentation, printing, and cleaning of each model was two to seven days. Models were printed with articulating parts, which opened along a plane to display the anatomic region of interest (eg, ventricular septal defect or aortic valve). The cardiac anomalies in the study group included various single-ventricle anatomies undergoing staged palliation, ventricular outflow anomalies, and anomalous pulmonary venous connections (Table 1).

3D-Printed Cardiac Model.
Cases’ Descriptions and Complexity Scores.
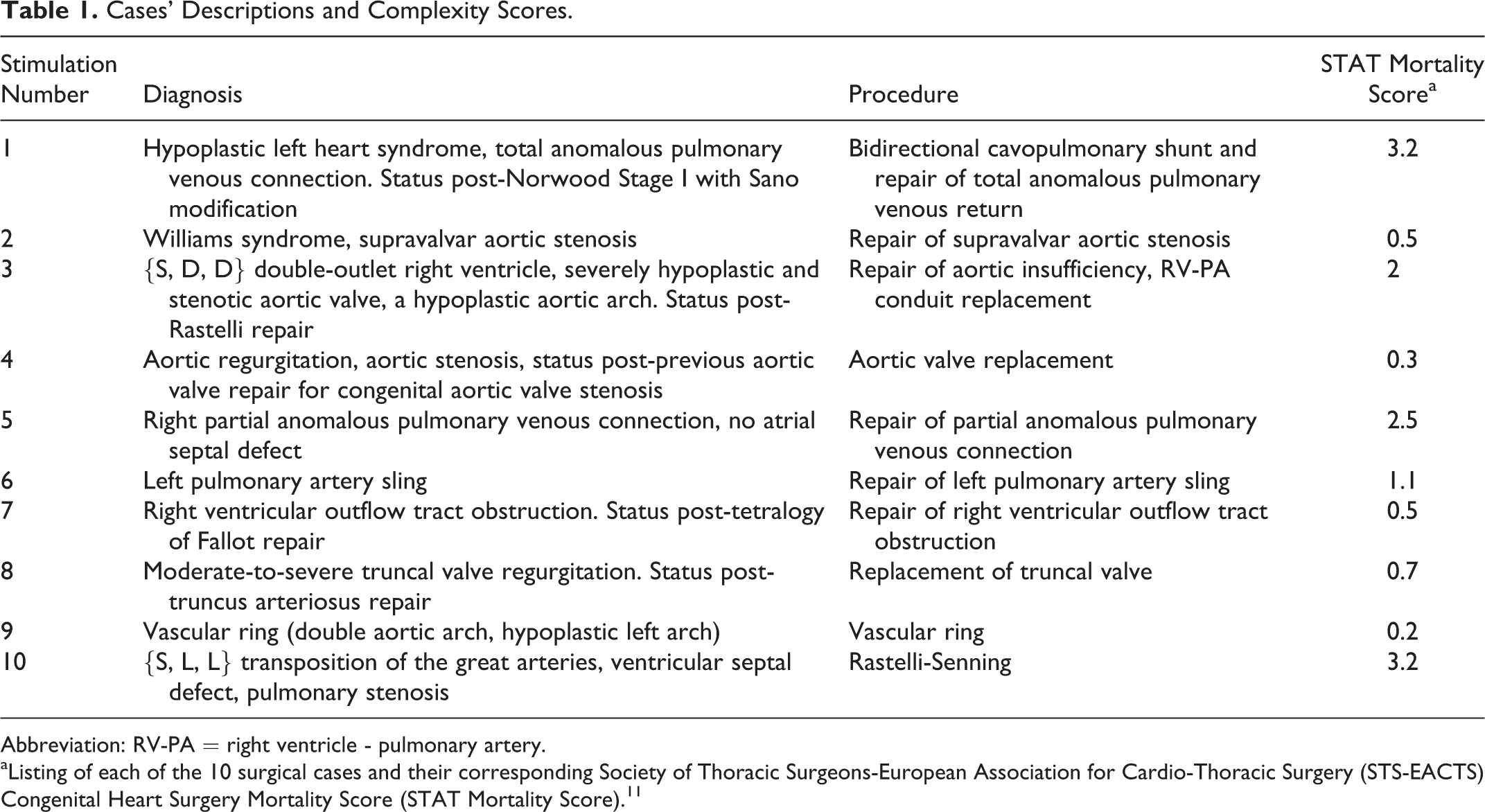
Abbreviation: RV-PA = right ventricle - pulmonary artery.
aListing of each of the 10 surgical cases and their corresponding Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery (STS-EACTS) Congenital Heart Surgery Mortality Score (STAT Mortality Score). 11
Near the completion of each surgery, approximately 30 minutes prior to arrival in the PCICU from the operative room, a congenital cardiac surgeon and an intensive care physician conducted a training session simulating patient-specific intra- and postoperative care utilizing the patient-specific 3D model for the PCICU team. Participants in the simulation included physician trainees, PCICU nurses, and ancillary care providers (included respiratory therapists and nurses with limited critical care experience). In each session, the patient’s preoperative anatomy was demonstrated with the 3D model, and the procedural details were demonstrated with the model in hand, utilizing the articulating segments to enhance the presentation of complex cardiac phenomena. Following the presentation, the group reviewed the more commonly anticipated complications and issues expected to require management, taking cues from the anatomic model as a starting point for discussion.
The basis for evaluation of the simulation models by participants was their experience with the conventional hand-off proceedings routinely used by the providers in our PCICU. Conventional postsurgical hand off entails succinct presentation of pertinent intraoperative findings, procedures performed, and perioperative therapies required in the operating room. Two-dimensional pictures are utilized in the conventional hand-off process. A clinical “snapshot” of the current status of the patient is also discussed, including amount of cardiorespiratory support required and pertinent laboratory values to indicate hemodynamic status. These details can be anchored to any type of imaging or visual aid as this reviewer suggests; however, an in-depth understanding of the patient’s anatomy prior to this discussion is key to a shared mental model of the patient anatomy and therefore expected clinical course.
After the simulation, using a 10-point Likert-type scale, each participant completed an eight-question survey assessing their perception of their knowledge acquisition and the impact of the training session. Each case was rated for complexity using the Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery (STS-EACTS) Congenital Heart Surgery Mortality Score 11 (STAT Mortality Score).
Univariate analysis comparing participant responses was carried out using t test, stratifying by provider type. Multivariable linear regression models were created to determine the predictive value of case complexity on participant responses, controlling for provider type (nurse, physician-in-training, and ancillary provider). Statistical analysis was performed with IBM SPSS Statistical software (version 21.0; IBM, Armonk, New York). Two-tailed P < .05 was considered statistically significant.
Results
Seventy PCICU providers enrolled in the study, including 22 physicians-in-training, 38 critical care nurses, and 10 ancillary providers. All participants completed one simulation session and completed the postsimulation questionnaire. Provider types were evenly distributed across each case simulation, with 5 to 12 participants per case.
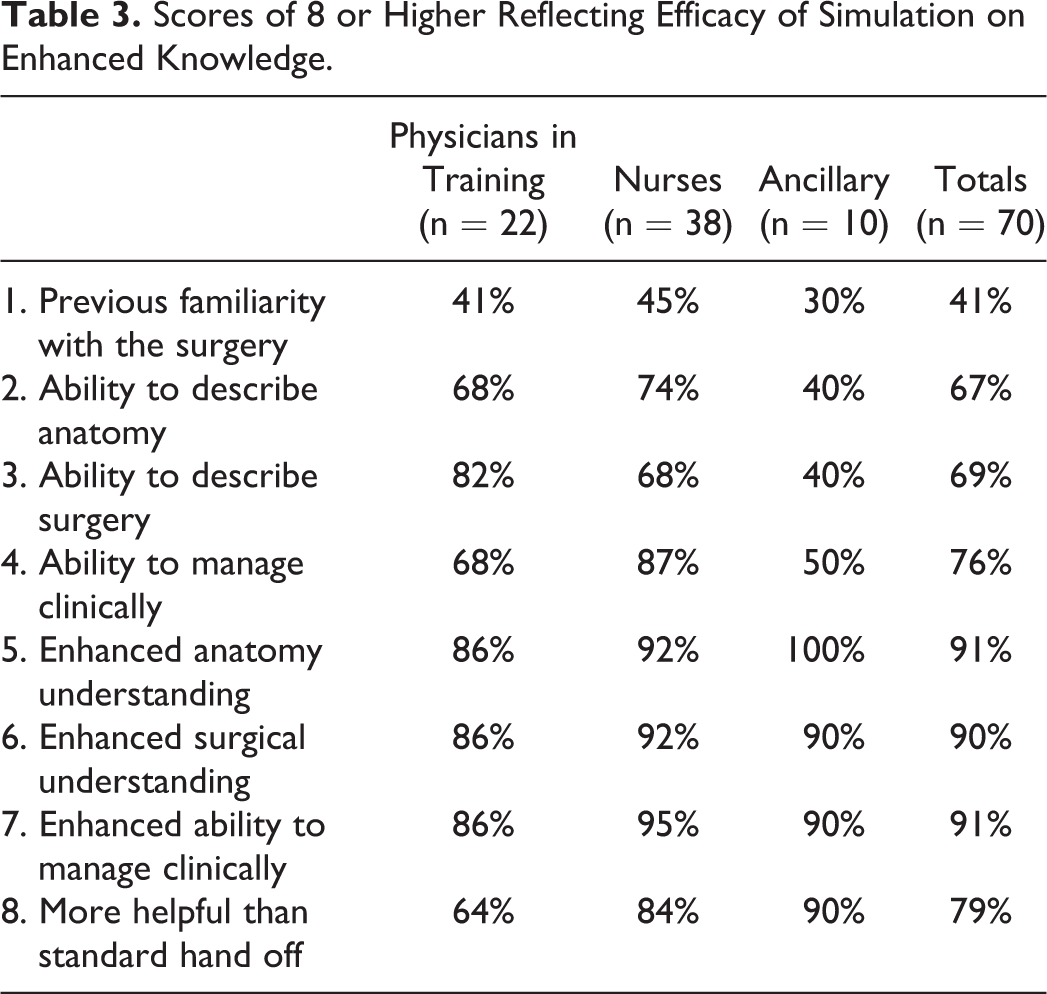
Univariate analysis of responses to each of the eight survey questions grouping by provider type is summarized in Table 2. Previous familiarity with the surgical cases was overall moderate, with nurses reporting higher compared to all other clinicians (7.7 ± 2.2 vs 5.8 ± 3.1; P = .04). Nurses scored significantly higher in self-reported confidence in their ability to clinically manage the patient postoperatively compared to physicians and ancillary providers (8.6 ± 1.1 vs 7.7 ± 2.0; P = .02). Taken together, physicians and nurses scored higher than ancillary providers in their ability to describe the anatomy (8.1 ± 1.5 vs 6.8 ± 2.3; P = .02), describe the surgical procedure performed (8.3 ± 1.5 vs .71 ± 2.1; P = .03), and to clinically manage postoperative complications (8.3 ± 1.3 vs 7.1 ± 2.6; P = .02) following the simulation. Nurses scored significantly higher in their perception that the 3D model simulation training directly enhanced their ability to clinically manage patients (9.5 ± 1.0 vs 8.7 ± 1.7; P = .02). Overall average response to whether simulation training was more effective than standard verbal hand off was 8.4 ± 2.1. Nurses and ancillary providers scored higher than physicians on this question (8.7 ± 1.9 vs 7.7 ± 2.2; P = .05). Table 3 summarizes the number of participants who scored 8 of 10 or higher for each questionnaire response. Ninety percent of participants score this highly for enhancement of anatomic understanding, enhancement of surgical understanding and enhancement of ability to clinically manage.
Mean Questionnaire Responses.a
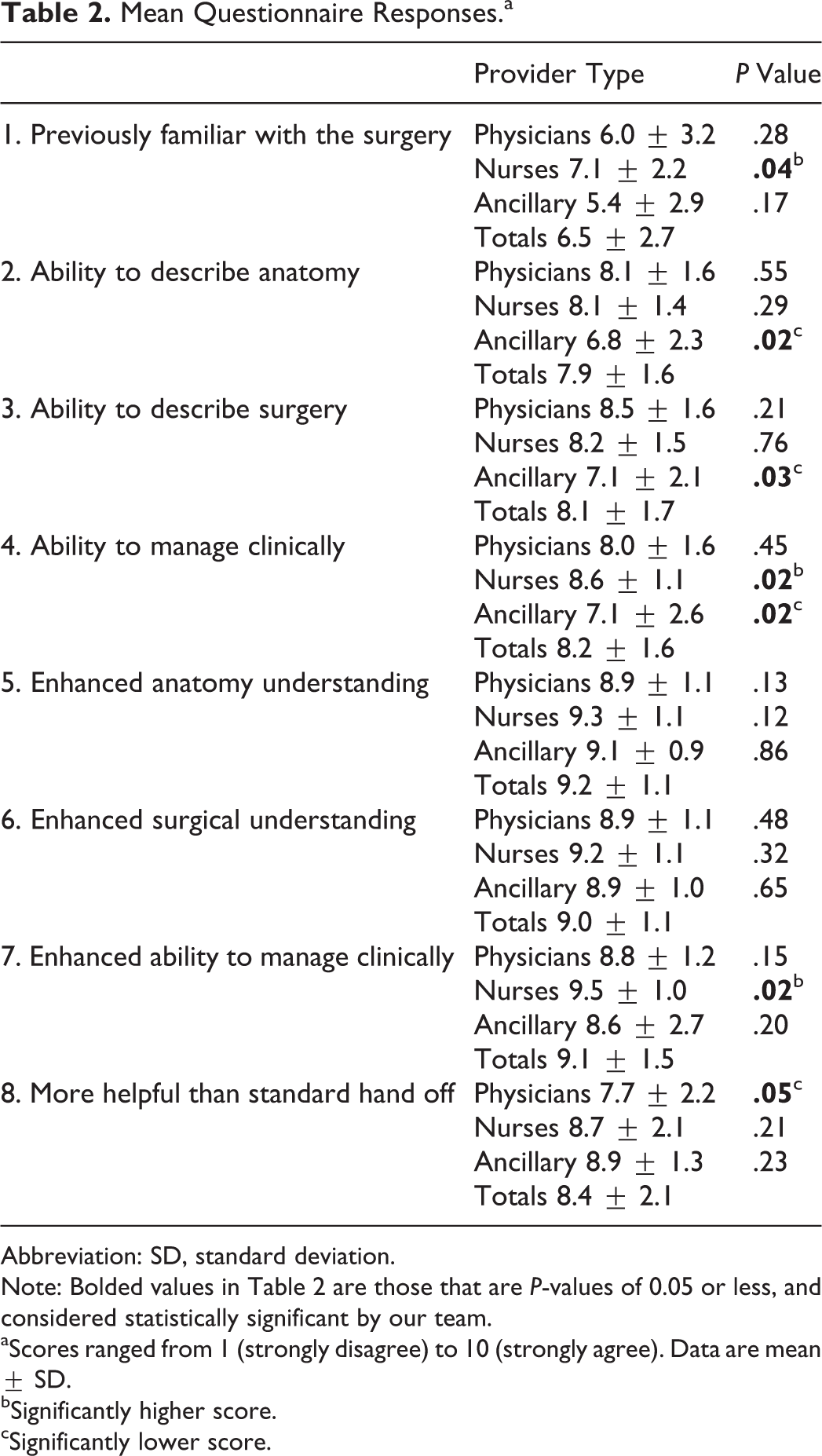
Abbreviation: SD, standard deviation.
Note: Bolded values in Table 2 are those that are P-values of 0.05 or less, and considered statistically significant by our team.
aScores ranged from 1 (strongly disagree) to 10 (strongly agree). Data are mean ± SD.
bSignificantly higher score.
cSignificantly lower score.
Scores of 8 or Higher Reflecting Efficacy of Simulation on Enhanced Knowledge.
The STAT Mortality Scores for the 10 surgeries ranged from 0.3 to 3.2 (Table 1). Multivariable linear regression analysis of questionnaire responses controlling for case complexity as a continuous variable and provider type found higher response scores, indicating 3D simulations were more helpful than standard hand off as complexity increased (P = .06, regression coefficient B = .43). This suggests that for each increase in complexity score by 1, the questionnaire response increased by 0.43. In addition, high complexity was a significant predictor of higher response scores indicating the 3D models enhanced understanding of the surgical procedure (P = .04, regression coefficient B = .55).
Comment
Progressive developments in simulation training offer expanding opportunities to enhance clinical readiness and problem solving; bolster limited clinical experience; 12,13 and improve communication, 14 quality, and costs. 15 Further opportunity to enhance transfer of clinical information across disciplines has the potential to optimize patient care and measurable outcomes. Patient hand off represents a critical moment in the hospital course when improvement can significantly impact efficiency, completeness of information transfer, and number of technical errors. 16 Similar 3D models have been utilized extensively at our institution for trainee education in a wide range of specialties, including pediatric residents, postdoctoral students, allied health providers, nurses, and adult congenital cardiology providers. Critical analyses of these training programs have shown 3D congenital cardiac models can significantly improve acquisition of knowledge and conceptualization of patient surgical anatomy in nonoperative pediatric residents 10 as well as medical students. 13 Complex congenital cardiac surgery cases are reviewed preoperatively using these models in select cases. We have previously reported on endovascular device deployment planning and success by performing the procedure on such models. 5 We believe the present study is the first report of the use of these models to facilitate transfer of patient care in a congenital cardiac surgery intensive care postoperative setting.
Our results echo previous findings that 3D model-based simulation training can influence provider care, 10 particularly in the form of clinician knowledge acquisition, self-assessment, and confidence. In the prior study, trainees were found to significantly improve in each of these areas following a simulation seminar regarding ventricular septal defect repairs in general, which we expanded upon by assessing these benefits when applied to specific patient anatomy and real-time patient care. Perceptions about efficacy and practicality greatly influence the institution and acceptance of simulation models by trainees, and our study focused on these aspects of communication and training. Traditional provider hand off focuses on verbal transfer of information, often in parallel between providers of the same specialty at each care location (eg, operating room to PCICU). That model of communication emphasizes efficient delivery of specialized information and clinical perspectives but conveys a limited assimilation of broader surgical concepts, including clinically relevant anatomic nuances. Our results demonstrate that a practical benefit from simulation training with 3D cardiac models is perceived by providers of all types and also suggest that different training backgrounds affect the degree of this benefit in certain respects.
In particular, nursing staff reported the highest enhancement of their ability to provide clinical care and also scored highest in their perceived management ability following the training sessions. These findings may suggest that nurses benefit greatly from the 3D conceptualization provided by the models that they would otherwise not receive during standard hand off and that this could improve the care they deliver. Physicians, though scoring highly with regard to enhancement of understanding and clinical ability following the simulations, reported statistically lower in response to the question of whether this type of hand off was better than standard verbal methods, even despite scoring lower on previous familiarity with the surgery. This may highlight differences in training background that prepares physicians to conceptualize anatomy and physiology with fewer visual cues but, importantly, reflects the clinicians’ perception of these questions and presently remains to be elucidated with respect to the impact on clinical outcomes.
In general, all three clinician groups indicated a benefit in perception of improved hand off using simulation training compared with standard hand off. Higher complexity score is a point that requires further investigation and could impact provider benefit. Complexity may have an association with enhancement of understanding of surgical details, independent of differences in provider anatomical and surgical background that can be better communicated via 3D model simulation. The application of a complexity score cutoff is designed for clinical utility and could have value to allocation of resources with regard to simulation training protocol development.
The value of this study is that we have utilized high-fidelity simulations that precisely represent the individual patient anatomy in a way that can be feasibly reproduced and adjusted for other clinical care settings. Limitations of this study included small sample size of patients as well as the use of end points that do not clearly translate to clinical end points. The necessary next step in evaluation of simulation training based on 3D-printed cardiac models is to measure clinical outcomes in a large prospective randomized controlled trial, evaluating parameters before and after the simulation. There is also a need to evaluate methods of tailoring training to optimize the benefit for providers depending on educational background. Lastly, incorporating a complexity threshold could prove clinically useful if externally validated in a larger sample. In conclusion, 3D printed cardiac model-based simulation training is a high-fidelity training technique that is clinically applicable to a high-volume, high-acuity congenital cardiac intensive care setting and measurably enhances interdisciplinary communication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an institutional grant from the Board of Visitors at Children’s National Health Systems.