
Abstract

O-1 Rapid, Simplified Technique for Surgical Atrioventricular Valve Replacement With the Melody Transcatheter Pulmonary Valve
J. Hammel1, J. Delaney2
1Department of Surgery, University of Nebraska Medical Center, Omaha, Nebraska USA, 2Department of Pediatrics, University of Nebraska Medical Center, Omaha, Nebraska USA
The Melody transcatheter valve has been adopted for replacement of the mitral or tricuspid valve. Previously demonstrated techniques for Melody atrioventricular valve implantation require time-consuming preparation of the prosthesis. This video demonstrates a rapid, simplified technique for Melody atrioventricular valve implantation.
In this technique, the annulus is sized, and a similar-sized ePTFE tube graft, 16 to 24 mm, is selected. A 15 mm long cuff of tube graft is cut, and one end is sutured to the annulus, so that the cuff sits in the atrium. Meanwhile, the valve is prepared by folding over the last row of stent wire spaces at each end, to shorten the valve from 33 to 23 mm length, and reduce projection into the atrium or ventricle. The valve is mounted to a balloon of equal diameter to the tube graft, and then deployed by dilation at the desired depth within the tube graft. If there is a concern for impingement on the ventricular outflow tract, the ventricular end of the stent can be bent inward slightly. The stent is tacked to the tube graft.
The video consists of a demonstration of these techniques during mitral valve Melody implantation in the arrested heart. For extra clarity, the steps will also be demonstrated in a porcine cardiac specimen. This technique reduces the time from decision to completed implantation to approximately 20 minutes, making the procedure particularly applicable as rescue after a long ischemic time for complex attempted native valve repair.
O-2 Cylinder Reconstruction of Severe Primary Tricuspid Valve Defects Using Tissue-Engineered Bovine Pericardium
D. Mazzitelli1, C. Noebauer1, J. S. Rankin1, R. Lange1
1German Heart Center Munich, Munich, GERMANY
O-3 Ross-Konno Procedure With Cylinder Mitral Valve Replacement in 49 Days Old Infant: Surgical Video
O. M. Fedevych1, O. F. Yachnik1, Y. B. Mykychak1, O. V. Ostras2, Y. Y. Ivanov1, I. M. Yemets1
1Department of Cardiac Surgery, Ukrainian Childrens Cardiac Center, Kyiv, UKRAINE, 2Department of Cardiology, Ukrainian Childrens Cardiac Center, Kyiv, UKRAINE
O-4 Repair of Tetralogy of Fallot Through a Right Axillary Incision
E. Williams1, A. Michael1, K. Nguyen1
1Icahn School of Medicine at Mount Sinai - Department of Cardiovascular Surgery, New York, USA
O-5 Cardiac Prosthetic Valvar Labelling Is Obfuscating, While Effective Orifice Area Is Flawed by Misconception of the Gorlin Formula
T. Ebels1, H. Pragt1, J. P. van Melle1
1University Medical Center Groningen, Groningen, NETHERLANDS
O-6 Double Inlet Left Ventricle: Quantitative Anatomy and Potential for Streaming of Blood Flows With Disparate Oxygen Saturations
S. Meyer1, M. M. Bartelings2, S. Y. Ho3, M. R. Jongbloed2, H. Uemura4, T. Ebels1
1University Medical Center Groningen-Center for Congenital Heart Diseases, Department of Cardiothoracic Surgery, Groningen, NETHERLANDS, 2Leiden University Medical Center-Department of Anatomy & Embryology, Leiden, NETHERLANDS, 3Royal Brompton Hospital-Cardiac Morphology, London, UNITED KINGDOM, 4Royal Brompton Hospital-Heart Division, London, UNITED KINGDOM
O-7 Rationale for a Stem Cell Trial in Hypoplastic Left Heart Syndrome Patients
S. Kaushal1, B. Wehman1
1University of Maryland Medical Center, Baltimore, USA
O-8 A Technique for Obtaining Fresh Autologous Blood in Small Children During Cardiac Surgery and Its Effects in Hemodilution and Coagulopathy
A. Weiss1, T. R. Lee1, A. J. Mittnacht2, I. Hollinger2, C. A. Rodriguez-Diaz2, K. H. Nguyen1
1The Icahn School of Medicine at Mount Sinai - Department of Cardiovascular Surgery, New York, USA, 2The Icahn School of Medicine at Mount Sinai - Department of Anesthesia & Critical Care, New York, USA
Intraoperative Blood Products.
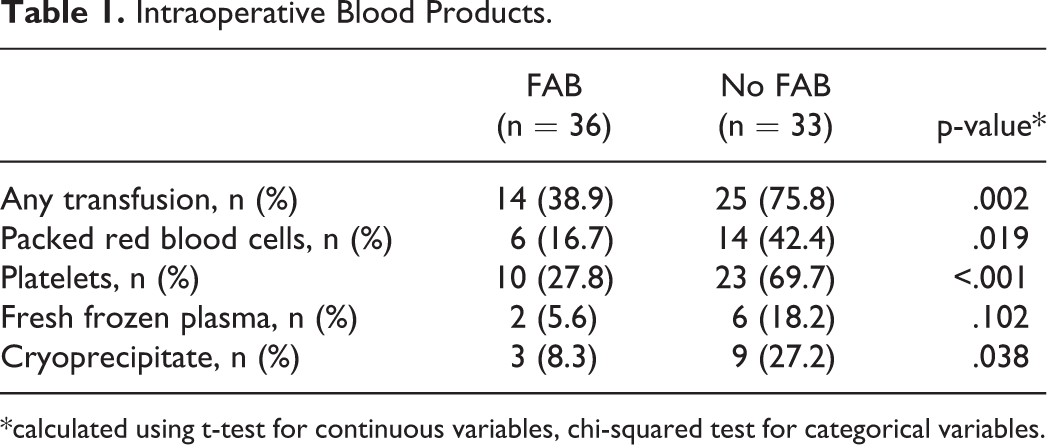
*calculated using t-test for continuous variables, chi-squared test for categorical variables.
O-9 Initial Results of a Program For Routine Standardized Longitudinal Follow-Up After Congenital Heart Surgery
S. Pasquali1, C. Ravishankar2, J. Hirsch-Romano1, K. Kane2, S. Viers1, A. Kennedy2, N. Burnham2, R. Lowery1, K. Uzark1, J. Rome2, J. Rossano2, J. Charpie1, R. Ohye1, T. Spray2, J. W. Gaynor2
1University of Michigan C.S. Mott Children’s Hospital, Ann Arbor, USA, 2The Children’s Hospital of Philadelphia, Philadelphia, USA
O-10 Supracardiac Total Anomalous Pulmonary Venous Return: Repair Using the Superior Extracardiac Technique (Video)
A. Fiore1, M. Hohenberg1, C. Bako1, C. Huddleston1
1Saint Louis University, Saint Louis, USA
O-11 The Optimal Timing of Stage 2 Palliation for Hypoplastic Left Heart Syndrome: An Analysis of the Pediatric Heart Network Single Ventricle Reconstruction Trial Public Database
J. Meza1, E. Hickey1, E. Blackstone2, S. Cai1, R. Jaquiss3, B. Anderson4, W. Williams1, G. Van Arsdell1, B. McCrindle5
1Hospital for Sick Children - Division of Cardiac Surgery, Toronto, CANADA, 2Cleveland Clinic - Departments of Thoracic and Cardiovascular Surgery and Quantitative Health Sciences, Cleveland, USA, 3Duke University Hospital - Division of Thoracic and Cardiovascular Surgery, Durham, USA, 4New York Presbyterian Morgan Stanley Childrens Hospital - Division of Cardiology, New York, USA, 5Hospital for Sick Children - Division of Cardiology, Toronto, CANADA
O-12 Health Care Costs of Hybrid and Norwood Strategies
A. Mazine1, R. Vanderlaan1, J. Meza1, A. M. Guerguerian2, S. Schwartz2, B. McCrindle3, G. S. Van Arsdell1, C. Caldarone1
1Division of Cardiovascular Surgery, Labatt Family Heart Centre, The Hospital for Sick Children, Toronto, CANADA, 2Department of Critical Care Medicine, The Hospital for Sick Children, Toronto, CANADA, 3Department of Pediatrics, Labatt Family Heart Centre, The Hospital for Sick Children, Toronto, CANADA
O-13 “Two Ventricle” Fontans – How Do They Perform?
R. Cerejo1, S. Laranjo2, R. Rodrigues1, C. Trigo2, I. Fragata3, F. Pinto2, J. Fragata1
1Hospital de Santa Marta - Centro Hospitalar Lisboa, Cardiothoracic Surgery Department, Lisboa, PORTUGAL, 2Hospital de Santa Marta - Centro Hospitalar Lisboa, Pediatric Cardiology Department, Lisboa, PORTUGAL, 3Centro Hospitalar Lisboa, Anesthesiology Department, Lisboa, PORTUGAL
O-14 Early and Late Outcomes of One and Half Ventricle Repair
M. Padalino1, A. Guariento1, M. Carrozzini1, B. Castaldi2, O. Milanesi2, G. Stellin1
1Pediatric and Congenital Cardiac Surgery, Universiti of Padova, Padova, ITALY, 2Pediatric Cardiology, University of Padova, Padova, ITALY
O-15 Single Pulmonary Artery Support for the Failing Fontan Circulation in Sheep
J. Van Puyvelde1, F. Rega1, C. Nix2, M. G. Hazekamp3, F. Rijnberg3, T. Siess2, P. Claus4, B. Cools5, M. Gewillig5, B. Meyns1
1University Hospital Leuven - Department of Cardiac Surgery Leuven BELGIUM, 2Abiomed Europe GmbH Aachen, GERMANY, 3Leiden University Medical Center - Department of Cardiothoracic Surgery, Leiden, NETHERLANDS, 4KU Leuven - Department of Cardiovascular Imaging and Dynamics, Leuven, BELGIUM, 5University Hospital Leuven - Department of Paediatric Cardiology, Leuven, BELGIUM
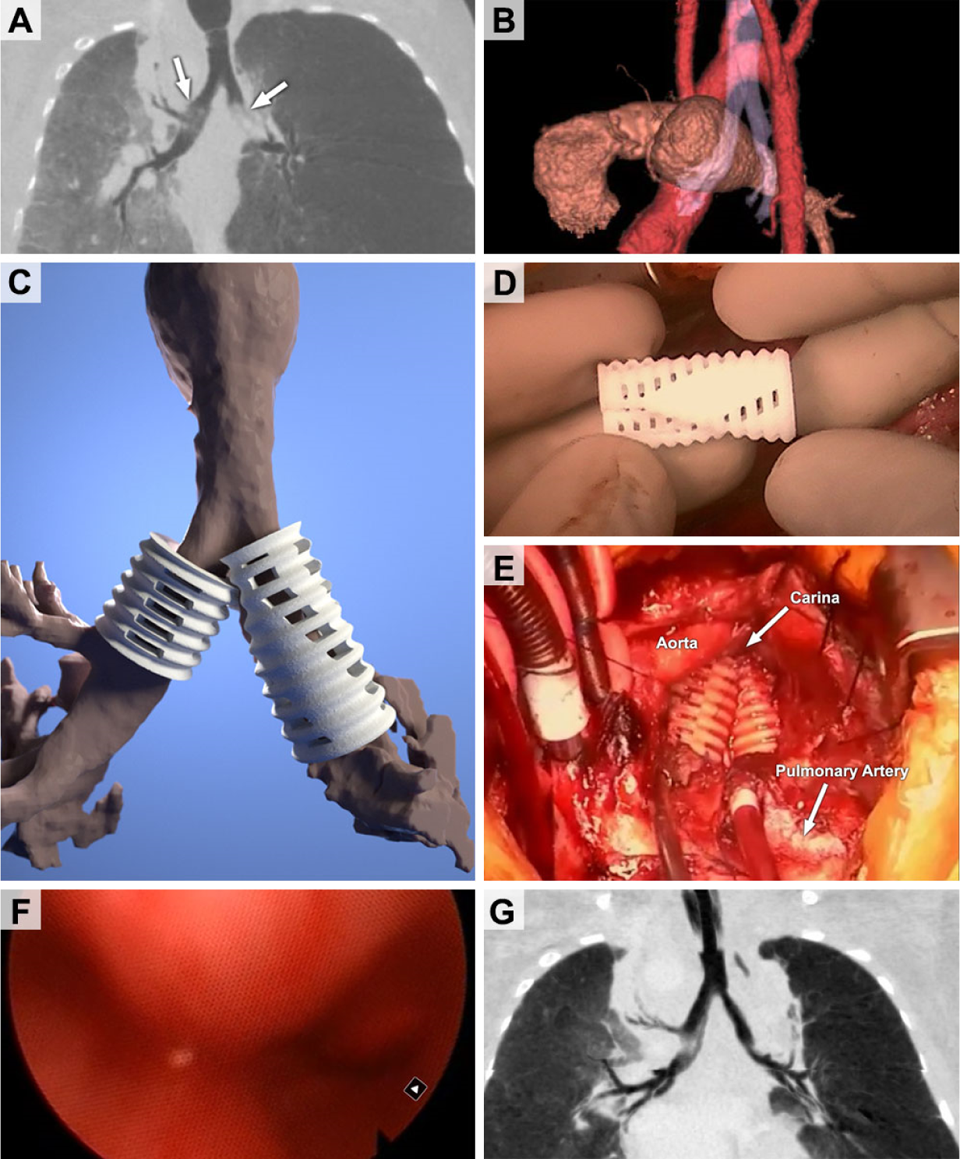
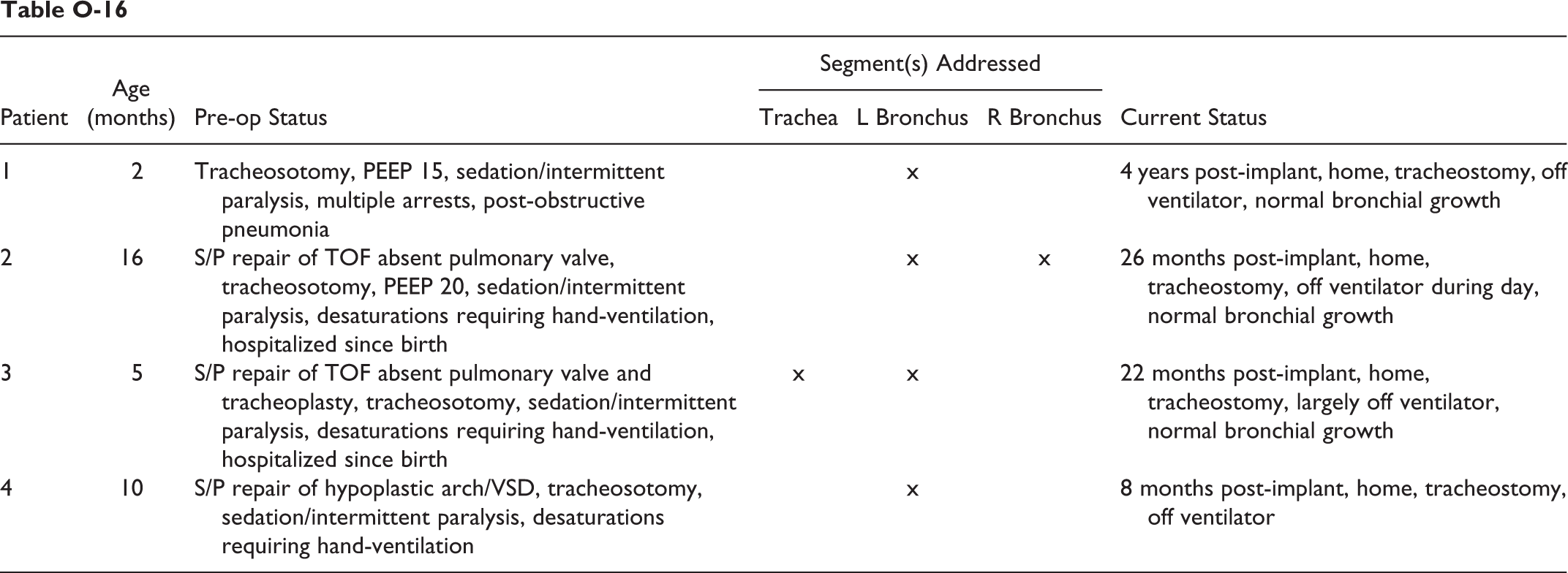
O-16 A Novel, 3-D Printed, Bioresorbable Tracheobronchial Splint for Pediatric Patients With Severe Tracheobronchomalacia
R. Ohye1, S. Hollister2,3, G. Green4
1University of Michigan Medical School, Department of Cardiac Surgery, Ann Arbor, USA, 2University of Michigan Medical School, Department of Surgery, Ann Arbor, USA, 3University of Michigan, Departments of Biomedical and Mechanical Engineering, Ann Arbor, USA, 4University of Michigan Medical School, Department of Otolaryngology, Ann Arbor, USA
O-17 Evaluation and Risk Stratification of Concomitant Cardiovascular Procedures With Slide Tracheoplasty for Combined Cardiac and Airway Defects
N. Muthialu1, M. Nakao1, L. Bezuska1, J. Marek1, I. Sullivan1, M. Kostolny1, V. Tsang1
1Great Ormond Street Hospital, London, UNITED KINGDOM
O-18 Reverse Subclavian Flap Repair of Hypoplastic Transverse Aorta in Infancy
K. Kanter1
1Emory University School of Medicine, Atlanta, USA
O-19 Right Aortic Arch: The New Paradigm
C. Backer1, O. Eltayeb2, M. Monge3, J. Rastatter4, C. Rigsby5
1Ann & Robert H Lurie Children’s Hospital of Chicago, Division of Cardiovascular-Thoracic Surgery, Chicago, USA, 2Ann & Robert H Lurie Children’s Hospital of Chicago, Division of Otolaryngology, Chicago, USA, 3Ann & Robert H Lurie Children’s Hospital of Chicago, Division of Medical Imaging, Chicago, USA
O-20 Surgery for Diseases of the Aortic Arch With a Minimum of 15 Years Follow-Up
T. Hoel1, H. Lindberg1
1Rikshospitalet University Hospital, Oslo, NORWAY
O-21 Neuropsychological and Psychosocial Outcomes in Adults Two Decades After a Neonatal Arterial Switch Operation
D. Kalfa1, L. Kasmi2, M. Montreuil2, N. Geronikola2, V. Lambert3, E. Murzi2, E. Belli3, D. Bonnet4
1Pediatric Cardiac Surgery, Morgan Stanley Childrens Hospital of New York-Presbyterian, Columbia University, New York, United States Minor Outlying Islands, 2Laboratoire de psychopathologie et neuropsychologie, Université Paris 8 Saint Denis, FRANCE, 3Centre de Référence Malformations Cardiaques Congénitales Complexes - M3C, Centre Chirurgical Marie Lannelongue, Plessis Robinson, FRANCE, 4Centre de Référence Malformations Cardiaques Congénitales Complexes - M3C, Hôpital Necker Enfants Malades, Paris, FRANCE
O-22 Neurodevelopmental Outcomes of Children Undergoing Congenital Heart Disease Repair Complicated by Post-Operative Thrombosis: A Prospective Observational Study
B. McCrindle1, L. Brandao, M. Rolland, S. O’Shea, S. Schwartz, J. Russell, V. B. Sivarajan, C. Manlhiot
1The Hospital for Sick Children, University of Toronto Toronto CANADA
O-23 Right Vertical Axillary Mini-Thoracotomy for Correction of Ventricular Septal Defects and Complete Atrioventricular Canal Defects in Infants and Children
A. Kadner1, P. Heinisch1, M. Veit1, O. Loup1, B. Eberle3, D. Hutter2, J. P. Pfammatter2, T. Carrel1
1University Hospital Bern, Center for Congenital Heart Disease, Department of Cardiovascular Surgery, Bern, SWITZERLAND, 2University Hospital Bern, Center for Congenital Heart Disease, Department of Cardiology, Bern, SWITZERLAND, 3University Hospital Bern, Center for Congenital Heart Disease, Department of Anesthesiology, Bern, SWITZERLAND
O-24 Aortic Valve Reconstruction in Children and Young Adults: Initial Experience With Ozaki Technique
P. del Nido1, M. Borisuk1, C. Baird1
1Department of Cardiac Surgery, Boston Childrens Hospital, Boston, USA
O-25 Revisiting the Two-Staged Repair in ‘Simple’ TGA
O. Kornoukhov1, V. Ilyn1
1Filatov Children’s Hospital, Moscow, RUSSIA
O-26 Surgical Management of Symptomatic Tetralogy of Fallot in Young Infants: Primary Repair Vs. Palliation – A Propensity Matched PHIS Database Analysis
K. Ramakrishnan1, D. Zurakowski2, R. Jonas1, P. Sinha1
1Children National Medical Center, Washington DC, USA, 2Boston Childrens Hospital, Boston, USA
O-27 Coronary Artery Translocation and Direct Reimplantation: An Effective Method for Management of AAOCA Without Intramural Segment and Inter-Arterial Course
D. Mauchley1, D. Campbell, M. Mitchell, J. Jaggers
1Children’s Hospital Colorado, Aurora, USA
O-28 Increased Surgical Mortality Associated With Partial Pulmonary Venous Obstruction in Patients With Type IV Total Anomalous Pulmonary Venous Connection
J. St. Louis1
1Children’s Mercy Hospital and Clinics, Kansas City, USA
O-29 Geographic Distribution of Congenital Heart Surgery Programs in the United States and Potential Impact of Regionalization
T. Karamlou1, S. Pasquali2, D. Overman3, C. Backer4, J. Hirsch-Romano2, K. Welke5
1UCSF Benioff Children’s Hospital, San Francisco, USA, 2C.S. Mott Children’s Hospital, University of Michigan, Ann Arbor, USA, 3Children’s Hospital of Minnesota, Minneapolis, USA, 4Ann and Robert H. Lurie Children’s Hospital, Chicago, USA, 5Children’s Hospital of Illinois, Peoria, USA
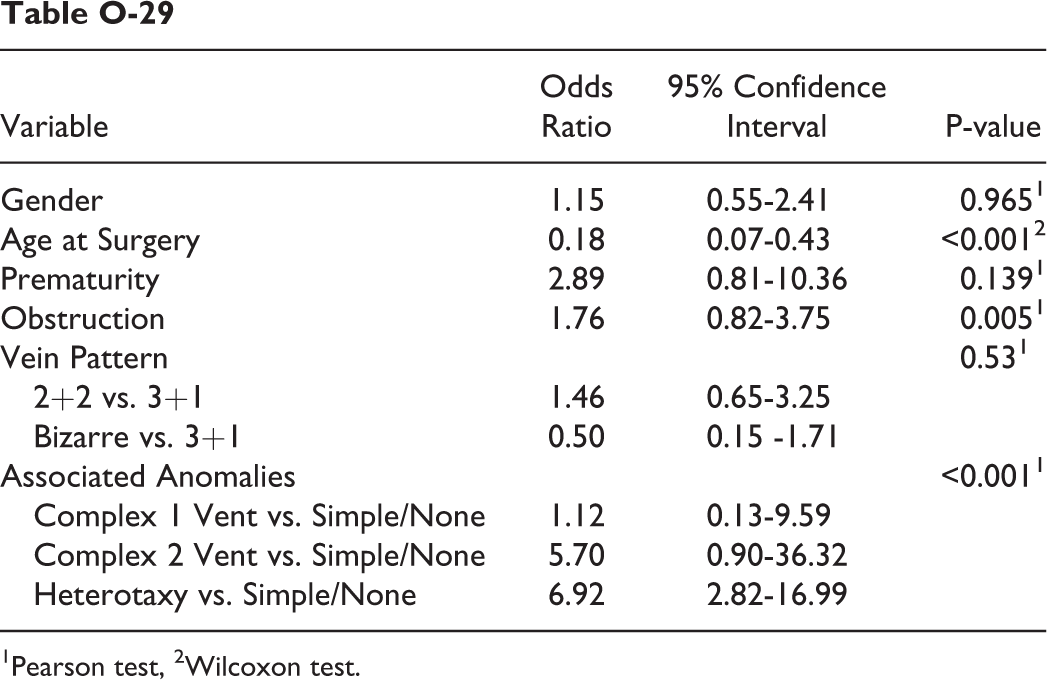
1Pearson test, 2Wilcoxon test.
O-30 Setting up, Monitoring and Self-Audit for New Pediatric Heart Programs in Emerging Healthcare Systems
A. Marath1, V. Nina2, E. Farkas1, J. Henson1, V. Nguyen1, L. Lundeen3, G. Bozzetti4, A. Akinyemi5
1CardioStart International, Tampa, USA, 2Federal University of Maranhao, Cardiac surgery, Sao Luis, BRAZIL, 3Oregon Health & Sciences University, Cardiac Surgery, Portland, USA, 4Golden Jubilee National Hospital, Cardiac Anesthesia, Glasgow, UNITED KINGDOM, 5University College Hospital, Cardiac Anesthesia, Lagos, NIGERIA
O-31 Surgical Intervention for Adults With Vascular Rings: A Multi-Center, 32-Year Experience
L. Vricella1, N. Hibino1, S. Collica1, C. L. Backer2, E. Bacha3, J. A. Dearani4, C. Caldarone5, R. Vanderlaan5, D. E. Cameron1
1Johns Hopkins University School of Medicine, Baltimore, USA, 2Lurie Childrens Hospital, Chicago, USA, 3Columbia University, New York, USA, 4Mayo Clinic, Rochester, USA, 5Hospital for Sick Children, Toronto, USA
O-32 The First Large-Animal, Gene-Targeted Model of Congenital Heart Disease and the Future of Surgical Training
P. Gruber1, K. Wells2, A. Spate2, E. Walters2, A. Firment3, A. Kashyap1, G. Baccam1, R. Prather2, A. Moon3
1University of Iowa, Iowa City, IA, USA, 2University of Missouri, Columbia, MO, USA, 3Weis Center for Research; Geisinger Clinic, Danville, PA, USA
O-33 Posterior Aortic Translocation: The Original Nikaidoh Technique Is Easier and Better
M. Hazekamp1, F. Villagra2, L. Galetti3, R. Hosseinpour4
1Leiden University Medical Center, Leiden, Netherlands, 2Hospital La Paz, Madrid, Spain, 3Ospedale Papa Giovanni XXIII, Bergamo, Italy, 4Hospital Virgen del Rocio, Sevilla, Spain
P-1 Repair of Truncus Arteriosus With Interrupted Aortic Arch, Using Continuous Mildly-Hypothermic Whole-Body Perfusion
J. Hammel1
1Department of Surgery, University of Nebraska Medical Center, Omaha, Nebraska, USA
Repair of persistent truncus arteriosus with interrupted aortic arch is typically carried out at deep hypothermic temperature with some combination of selective cerebral perfusion and circulatory arrest. This video demonstrates the repair of this lesion in a newborn girl, at 32 deg C, with continuous full-flow cardiopulmonary bypass to the upper and lower body achieved through simultaneous cannulation of the innominate artery and the descending aorta above the diaphragm.
The author has previously shown the Society the performance of the Norwood operation at mild hypothermia, incorporating the descending aortic cannulation. In this video, the versatility of this cannulation and perfusion technique is demonstrated. Special emphasis is given to the easy exposure and secure cannulation of the descending aorta. Using the same cannulation technique, all operations involving reconstruction of the aortic arch can be performed. Hypoperfusion of the kidney and other abdominal organs is obviated; this patient was non-oliguric in the day following surgery and achieved negative fluid balance in the subsequent day. Potentially deleterious effects of profound cooling, e.g. on coagulation, are avoided. In addition to red cells in the bypass prime, this patient received a platelet transfusion, but no other blood products were required. Immediate chest closure is routine.
Aortic arch reconstruction with dual, innominate artery and descending aortic arterial cannulation and whole-body, continuous, full-flow cardiopulmonary bypass is a potentially important contribution in the continuing refinement of surgical techniques and the reduction of morbidity resulting from the most complex neonatal operations.
P-2 End-of-Life in Children With Complex Congenital Heart Disease: Perspectives on Suffering and Quality of Life
C. Agosto1, F. Benedetti1, F. Benini1, V. De Tommasi1, O. Milanesi2, G. Stellin3, M. Padalino3
1Center for Pediatric Palliative Care, Dept. of Woman and Child’s Health, University of Padova, Padova, ITALY, 2Pediatric Cardiology Unit, Dept. of Woman and Child’s Health, University of Padova, Padova, ITALY, 3Pediatric and Congenital Cardiac Surgery Unit, Dept. of Cardiac, Thoracic and Vascular Sciences, University of Padova, Padova, ITALY
P-3 Pulmonary Valve-Sparing Techniques During Repair of Tetralogy of Fallot: The Delamination Plasty
V. Vida1, F. Zucchetta1, A. Guariento1, M. Padalino1, O. Milanesi2, G. Stellin1
1Pediatric and Congenital Cardiac Surgery Unit, Padua, ITALY, 2Pediatric Cardiology Unit, Padua, ITALY
P-4 Right Ventricle-to-Pulmonary Artery Connection Reconstruction for Patients With Truncus Arteriosus: 19 Years of Experience
Y. Y. Ivanov1, Y. B. Mykychak1, O. M. Fedevych1, K. S. Chasovskyi2, I. M. Yemets1
1Department of Cardiac Surgery, Ukrainian Childrens Cardiac Center, Kyiv, UKRAINE, 2Department of Perfusiology, Ukrainian Childrens Cardiac Center, Kyiv, UKRAINE
P-5 Surgical Decision-Making Improved By 3D Modelling
S. Speggiorin1, S. Durairaj2, B. Mimic1, A. F. Corno1
1Department of Paediatric Cardiac Surgery - East Midlands Congenital Heart Centre, Leicester, UNITED KINGDOM, 2Department of Paediatric Cardiology - East Midlands Congenital Heart Centre, Leicester, UNITED KINGDOM
Long-segment tracheal stenosis. Tetralogy of Fallot - Absent Pulmonary Valve, status/post Ventricular Septal Defect (VSD) closure, right ventricle-pulmonary artery conduit and Lecompte manoeuvre, with severe airway compression. The 3D modelling allowed to choose the best approach for Lecompte take-down and relief of airway compression. Status/Post aortic arch enlargement, with the clearest identification of the morphology responsible for the obstruction Apical muscular VSD Multiple muscular VSDs, with one opening in the left ventricle and two separate and distant openings into the right ventricle. The 3D modelling allowed to plan hybrid approach for all VSDs closure Double Outlet Right Ventricle with remote VSD, where 3D printed cast showed a potential additional VSD
P-6 Mid-Term Outcome for Repair of Congenital Heart Defects Using Tissue Engineered Bovine Pericardium
S. Prabhu1,2,3, D. Bell2, R. Justo1,2,3, B. Anderson1,2,3, T. Karl2,4, N. Alphonso1,2,3
1Queensland Paediatric Cardiac Services, Brisbane, AUSTRALIA, 2UQ School of Medicine, University of Queensland Brisbane, AUSTRALIA, 3Mater Medical Research Institute, Brisbane, AUSTRALIA, 4Cardiac Surgery, John Hopkins All Childrens Hospital, Florida, USA
P-7 Superior Vena Cava Banding in Preparation for Unilateral Bidirectional Glenn in Single Ventricle Patients With Bilateral Superior Vena Cavae
K. Pourmoghadam1, D. Nykanen1, M. Schwartz1, M. O’Brien1, M. Ruzmetov1, W. DeCampli1
1Arnold Palmer Hospaital for Children, Orlando, USA
P-8 Patterns of Treatment and Early Outcomes in Children With Functionally Single Ventricle. Data From ECHSA Congenital Database
B. Maruszewski1, A. Kansy1, Z. Tobota1, T. Ebels2, G. Sarris3, J. P. Jacobs4, J. Fragata5
1Childrens Memorial Health Institute, Warsaw, POLAND, 2University Medical Center Groningen, Groningen, NETHERLANDS, 3Athens Heart Surgery Institute, Athens, GREECE, 4Johns Hopkins All Childrens Heart Institute, St. Petersburg, USA, 5Hospital de Santa Marta, Lisbon, PORTUGAL
P-9 Centennial of the Du Bois and Du Bois Formula for Body Surface Area: Reappraisal and Appropriateness in the Era of Obesity
T. Ebels1, G. Bocca1, B. Bartelds1, J. P. van Melle1
1University Medical Center Groningen, Groningen, NETHERLANDS
P-10 Scimitar Vein Translocation Using an Off-Pump Right Thoracotomy Approach
J. W. Brown1, H. Al Kindi1
1Indiana University, Indianapolis, USA
P-11 Dilatable Main Pulmonary Artery Banding for Successful Postponement or Avoidance of Surgical Repair
J. Van Puyvelde1, F. Rega1, B. Cools2, B. Eyskens2, M. Gewillig2, B. Meyns1
1University Hospital Leuven - Department of Cardiac Surgery, Leuven, BELGIUM, 2University Hospital Leuven - Department of Paediatric Cardiology, Leuven, BELGIUM
P-12 Pulmonary Valve Replacement With the Biopulmonic™ Conduit: Early Disappointing Results
A. Quarti1, E. Merlino1, F. Iezzi1, G. Santoro1, C. Surace1, M. Colaneri1, M. Pozzi1
1Paediatric and Congenital Cardiac Surgery and Cardiology, Ospedali Riuniti, Ancona, ITALY
P-13 Fontan Conversion in Double-Inlet Single Ventricle: An Alternative Approach With In-Situ Total Cavopulmonary Connection and Systemic Venous Atrial Exclusion
A. Polimenakos1, A. Gupta1, B. Shafer1, V. Kamath1
1Children’s Hospital of Georgia / Medical Collge of Georgia, Augusta, USA
P-14 Use of the Berlin Heart Excor™ as a Total Artificial Heart in Infants
H. Kato1, S. Gandhi1
1BC Children’s Hospital, Department of Cardiothoracic Surgery, Vancouver, CANADA
P-15 Tissue Engineering of the Right Heart Outflow Tract by a Biofunctionalized Bioresorbable Polymeric Valved Tube: Mid-Term Results of the TEH-TUBE Program
D. Kalfa1, M. Pontailler2, B. Ahmad3, P. Pouponneau4, M. Blanchy5, K. Thibaut6, P. Hommes-Schattmann7, A. Neffe7, V. Vanneaux8, P. H. Menasché(2,9)
1TEH-Tube scientific coordinator, New York, United States Minor Outlying Islands, 2INSERM U970, PARCC & Laboratoire de Recherches Biochirurgicales, Hôpital Européen Georges Pompidou, Paris, FRANCE, 3UCL School of Pharmacy, Department of Electrospinning, University College London, London, UNITED KINGDOM, 4Statice SAS Besançon, FRANCE, 5Rescoll Bordeaux, FRANCE, 6Celyad SA Mont-Saint-Guibert, BELGIUM, 7HZG Berlin, GERMANY, 8APHP, Hôpital Saint-Louis, Laboratory of Cell Therapy; University Paris Diderot, Paris, FRANCE, 9APHP, Hôpital Européen Georges Pompidou, Department of Cardiovascular Surgery, Paris, FRANCE
P-16 The Arterial Switch Operation in Patients With Transposition and Left-Sided Aorta
S. Talwar1, S. K. Gupta1, A. K. Bhoie1, P. Ramakrishnan1, R. H. Anderson2, S. K. Choudhary1, S. S. Kothari1, R. juneja1, A. Saxena1, B. Airan1
1All India Institute of Medical Sciences, New Delhi, INDIA, 2 Institute of Genetic Medicine, Newcastle University, Newcastle-upon-Tyne, UNITED KINGDOM
for infants with transposition. The procedure is technically challenging when the aorta is left-sided, and requires surgical expertise and precision for a good surgical outcome. We review here our experience with such patients.
P-17 Peacock Tail Technique Simultaneously to Glenn in Patients With Ebstein Malformation and Failing Right Ventricle: The Tirana Modification
A. Veshti1, A. Baboci1, E. Kajo1, N. Maliqari2, E. Prifti1
1Department of Cardiovascular Sciences, Cardiac Surgery Division, Mother Theresa Universitary Hospital, Tirana, ALBANIA, 2Department Of Pediatrics, Mother Theresa Universitary Hospital, Tirana, ALBANIA
P-18 The Fate of Extracellular Matrix Valves in Right Ventricular Outflow Tract Reconstruction
F. Scholl1, A. Levy1, S. Bibevski1
1Joe DiMaggio Children’s Hospital, Hollywood, USA
P-19 Incidence, Etiology and Risk Factors of Unplanned Readmissions After Congenital Heart Surgery
E. Lushaj1, K. Nelson1, K. Amond1, E. Kenny1, P. Anagnostopoulos1
1University of Wisconsin-Madison, Department of Surgery, Madison, USA
Median time-to-first readmission was 21 (IQR: 12-58) days. Median HLOS at readmission was 2 (IQR: 1-8) days. The 1-, 3-, 6- and 12-month freedom from first readmission was 98%, 96%, 95% and 88% respectively (Figure-1). There was no significant difference in survival between readmitted and non-readmitted patients (p = 0.68). Time-to-readmission and readmission frequency didn’t impact patient survival (p > 0.05).
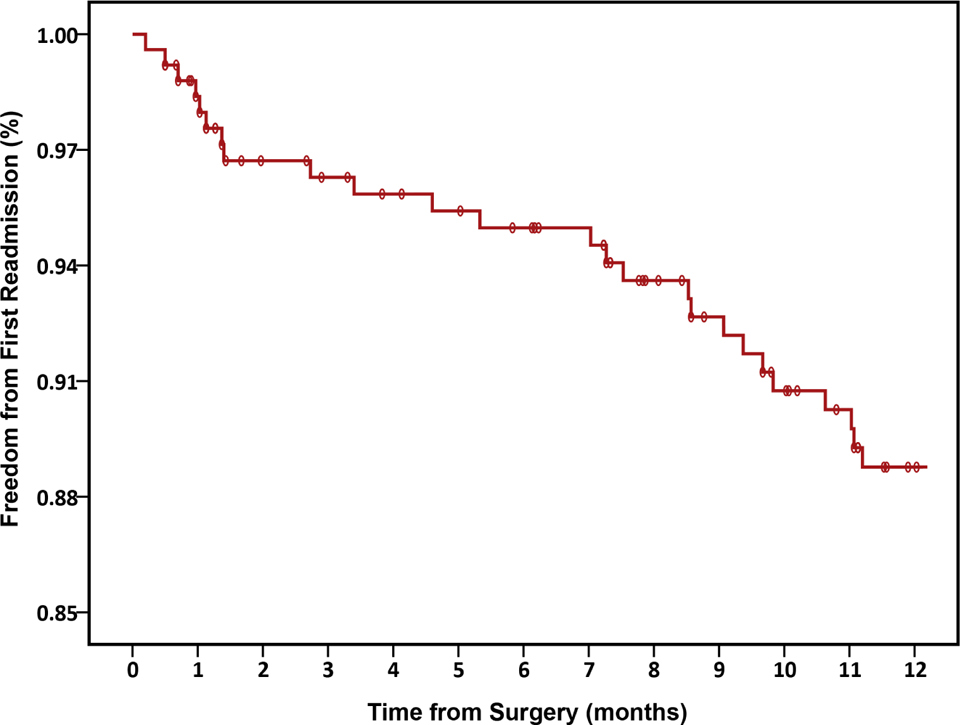
Kaplan-Meier plot demonstrating freedom from first unplanned readmission following CHS.
P-20 National Trend and Variability in Blood Utilization in Pediatric Cardiac Surgery
M. Karimi1, J. Sullivan2, C. Hronek3
1Yale University School of Medicine-Children’s Medical Center New Haven USA, 2Connecticut Children’s Medical Center Hartford, USA, 3Children’s Hospital Association Kansas City, USA
P-21 An Update of the Analysis of Outcomes in Neonatal Congenital Heart Surgery: Data From ECHSA Congenital Database
A. Kansy1, G. Sarris2, T. Ebels3, J. P. Jacobs4, Z. Tobota1, J. Fragata5, B. Maruszewski1
1Childrens Memorial Health Institute, Warsaw, POLAND, 2Athens Heart Surgery Institute, Athens, GREECE, 3University Medical Center Groningen, Groningen, NETHERLANDS, 4Johns Hopkins All Childrens Heart Institute, St. Petersburg, USA, 5Hospital de Santa Marta, Lisbon, PORTUGAL
P-22 Aortic Translocation With Aortic Free Wall Patch Plasty for Optimal Repositioning of Coronary Artery
T. Sakurai1, H. Sakurai1, T. Nonaka1, M. Kosakai1, T. Osawa1
1Chukyo Hospital, Nagoya, JAPAN
P-23 Comprehensive Valve Program in Pediatric Patients Undergoing Re-entry Right Ventricular Outflow Track Intervention in the Transcatheter Era: Implementation of a Customized Approach and Review of Early Outcomes
A. Polimenakos1, A. Gupta1, B. Shafer1, Z. Amin1, K. Vinayak1
1Children’s Hospital of Georgia / Medical College of Georgia, Augusta, USA
P-24 The Destiny of Post Operative Residual Ventricular Septal Defects After Surgical Repair
S. Bibevski1, J. Decker1, A. Sorunmu1, K. C. Chan1, F. G. Scholl1
1Joe DiMaggio Children’s Hospital, Hollywood, USA
P-25 Del Nido and Conventional Multi-Dose Cardioplegia Solutions in Congenital Heart Surgery: A Single-Center Comparison
K. Pourmoghadam1, M. Ruzmetov1, G. Plancher1, T. Benjamin1, H. Hardison1, A. Cherukuri1, K. Piggott1, M. O’Brien1, S. Suguna Narasimhulu1, W. DeCampli1
1Arnold Palmer Hospital for Children, Orlando, USA
P-26 Disaster Recovery and Pediatric Cardiac Program Building in Nepal May 2015: Moral Imperative Vs Personal Safety Assurance
A. Marath1, V. Nina2, E. Farkas1, R. Vilela de Abreu Haickel2, J. Henson1, M. Devbhandari3, R. Karmacharya3, R. Koju3
1CardioStart International, Tampa, USA, 2Federal University of Maranhao, Sao Luis, BRAZIL, 3University of Kathmandu, Dhulikhel, NEPAL
Specialist trauma assistance; Rapid delivery of two 40-foot medical containers from the USA following the first tremblor, to assemble the fully operational surgical suite and ICU; Daily seminars to teach familiarity with the new program; Intense outreach pediatric cardiology clinic activity to make immediate diagnoses, and provide conduits for future management.
Fast-tracking of pediatric program building and ICU management skills evolved, by including adult surgical development simultaneously; Markedly increased levels of late congenital cardiac lesions were identified followed intense evacuation of trauma victims from affected areas; New active rheumatic heart disease diagnoses were diagnosed, permitting early treatment and ongoing tracking; Financial budget load of other departments were eased rather than imperiled by general hospital donations included among specialist equipment.