
Abstract
We report two neonates with distal ductal origin of the left pulmonary artery who also had rare vascular rings comprised of a left aortic arch and right arterial duct with a midline/rightward descending aorta. To the best of our knowledge, this association has not previously been described, although other abnormalities of the left pulmonary artery in the setting of vascular rings have been reported. We review the embryology, utility of imaging, and clinical course.
Introduction
Vascular rings are rare anomalies of the extrapericardial arterial pathways resulting in complete encompassment of the trachea and esophagus by vascular structures. The most common variations are double aortic arch (49.7%) and right aortic arch, aberrant left subclavian artery, and retroesophageal diverticulum of Kommerell (25.9%). 1 Kommerell first described his retroesophageal diverticulum in 1936 in the setting of a left aortic arch and aberrant right subclavian artery. 2 A complete ring is present in this variation when a right ligament or arterial duct arises from the base of the right subclavian artery and joins a right-sided descending aorta. This is a very rare vascular ring, but even rarer is the ring comprised of a left aortic arch with a normal right-sided brachiocephalic artery and a right arterial duct joining the right-sided descending aorta. 1 We present two neonates with this latter arrangement, both associated with distal ductal origin of the left pulmonary artery (LPA) from the aorta. In both situations, bilateral arterial ducts were present, with the left arterial duct providing the connection between the LPA and the aorta. Ductal origin of the LPA is in and of itself a rare cardiac defect and usually occurs in the presence of a right aortic arch. 3 Although its association with bilateral arterial ducts has been described, 3 this does not form a vascular ring in the setting of a right arch. The combination of ductal origin of the LPA with bilateral arterial ducts occurring in the setting of a left aortic arch, to the best of our knowledge, has not been previously reported. We have now encountered two patients with this rare arrangement.
Case 1
A 29 weeks’ gestation, 1.15-kg twin neonate underwent an echocardiogram after birth secondary to respiratory distress. Distal ductal origin of the LPA was noted (Figure 1), and prostaglandin infusion was initiated. After three weeks, she was transferred to our institution where echocardiographic interrogation confirmed the diagnosis of a left-sided arch and aberrant right subclavian artery. Intracardiac anatomy was normal, including patency of the oval foramen. She underwent surgical repair via sternotomy, with implantation of the LPA into the pulmonary trunk on cardiopulmonary bypass. A nasoduodenal tube was in place throughout her postoperative recovery. Chromosome 22q11 deletion was identified. She failed extubation postoperatively; bedside bronchoscopy one month after repair was concerning for tracheomalacia. Prior to a scheduled laryngobronchoscopy, she developed acute, massive hemoptysis that rapidly decompensated into hemodynamic collapse. Emergent laparotomy revealed no source of bleeding within the distal esophagus, stomach, and duodenum. Simultaneous esophagoscopy localized the source to the proximal esophagus, concerning for an aortoesophageal fistula. Despite aggressive surgical efforts, the patient could not be resuscitated.
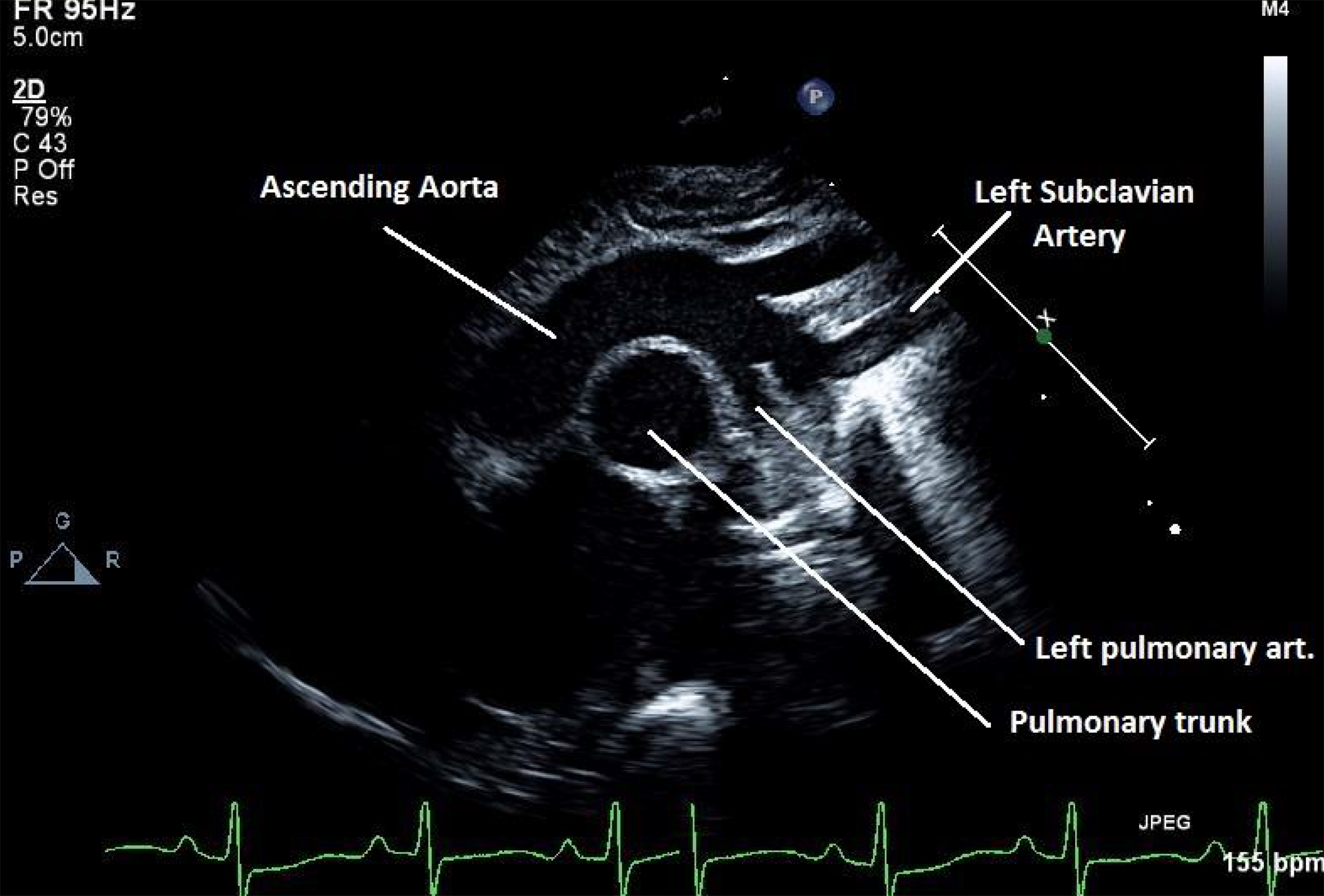
Echocardiographic still image of the suprasternal view demonstrates ductal origin of the left pulmonary artery from the aorta.
At autopsy, surgical repair was intact. The unexpected finding was a complete vascular ring consisting of a left aortic arch, aberrant right subclavian artery, patent right-sided arterial duct, and right-sided descending aorta. A ruptured aortoesophageal fistula was identified.
Case 2
A 35 weeks’ gestation, 2.15-kg twin neonate underwent echocardiographic interrogation after birth, with prenatal examination having aroused concern for aortic coarctation. The postnatal study revealed no coarctation but demonstrated distal ductal origin of the LPA. The intracardiac anatomy was otherwise normal, including patency of the oval foramen. The aortic arch was left-sided, with a right-sided brachiocephalic artery. A right-sided duct was also present joining the descending aorta. A computed tomography (CT) angiogram confirmed the presence of a vascular ring.
At one week of life, the patient underwent sternotomy, with implantation of the LPA into the pulmonary trunk on cardiopulmonary bypass and ligation and division of the right-sided arterial duct. He was extubated uneventfully after delayed sternal closure and was discharged at six weeks.
Discussion and Lessons Learned
Formation of the human aortic arch requires understanding of the fate of the arteries initially extending through the pharyngeal arches. These are initially symmetric structures, which undergo a series of asymmetric changes to account for the final configuration. There are five arteries on either side, not including the alleged fifth arch artery, which, to the best of our knowledge, has been identified only as an incomplete structure in a solitary human embryo. The remaining arches, named 1 through 4 and 6, undergo consequential changes, which result ultimately in the bilateral third arteries forming the common carotid arteries, the right fourth artery remaining as the proximal right subclavian, the left fourth artery becoming the definitive left aortic arch, with regression of the distal right sixth (ductal) arch and the right distal dorsal aorta. The distal left sixth artery remains as the left-sided arterial duct. This is the mechanism of formation of the most commonly encountered left aortic arch with right brachiocephalic artery and left-sided arterial duct. 4
As the pharyngeal arches remodel, pairs of endocardial cushions are formed by endothelial-to-mesenchymal transformation of cardiac jelly, and these are found along the length of the outflow tract, which distally is continuous with the aortic sac. At the base of the aortic sac, the right and left pulmonary arteries develop within the mediastinal mesenchyme, arising from the ventral components of the sixth arch arteries. As the right fourth and dorsal sixth arches start to involute, the endocardial cushions fuse distally with a protrusion growing from the dorsal wall of the aortic sac to separate the intrapericardial components of the aortic and pulmonary trunks. The obliquity of the protrusion as it grows into the pericardial cavity allows for continuity of the pulmonary trunk and the left sixth arch, which eventually develops into the left arterial duct. 5 Failure of fusion of the protrusion, which is the embryonic aortopulmonary septum, with the distal ends of the major outflow cushions provides a plausible explanation for the morphogenesis of aortopulmonary windows. 6
Distal ductal origin of the LPA occurs most commonly in conjunction with a right aortic arch and complex intracardiac defects, especially tetralogy of Fallot with pulmonary stenosis or atresia. 3 Persistence of the distal left sixth arch produces the arterial duct feeding the discontinuous LPA. In a right-sided arch, the left-sided arterial duct usually connects the left brachiocephalic artery to the LPA, whereas in a left arch, the left arterial duct connects the LPA to the descending aorta. 7
Disturbances in the normal pattern of regression of the pharyngeal arch arteries result in arch anomalies, which may become symptomatic if a complete ring is present. Well-recognized vascular rings are relatively easy to identify on echocardiographic evaluation. Other types of vascular rings have been reported, but identification of these subtypes is made difficult by their rarity and the lack of consistent ductal patency. One of these is the left aortic arch with aberrant right subclavian artery, right descending aorta, and right-sided arterial duct or ligament. Regression of the proximal right fourth aortic arch results in an aberrant right subclavian artery, which remains connected in retroesophageal fashion to the descending aorta via persistence of the dorsal portion of the right fourth aortic arch. Persistence of the right sixth ductal arch completes the vascular ring. This was the type of ring identified in our first patient (Figure 2). On retrospective review of the echocardiographic images, antegrade diastolic flow was identified originating in the right pulmonary artery (RPA) by color flow mapping and Doppler interrogation (Figure 3). This was a clue to the insertion site of the right-sided arterial duct. In addition, the duct can be seen inserting into the RPA in the parasternal short-axis view (Figure 4).
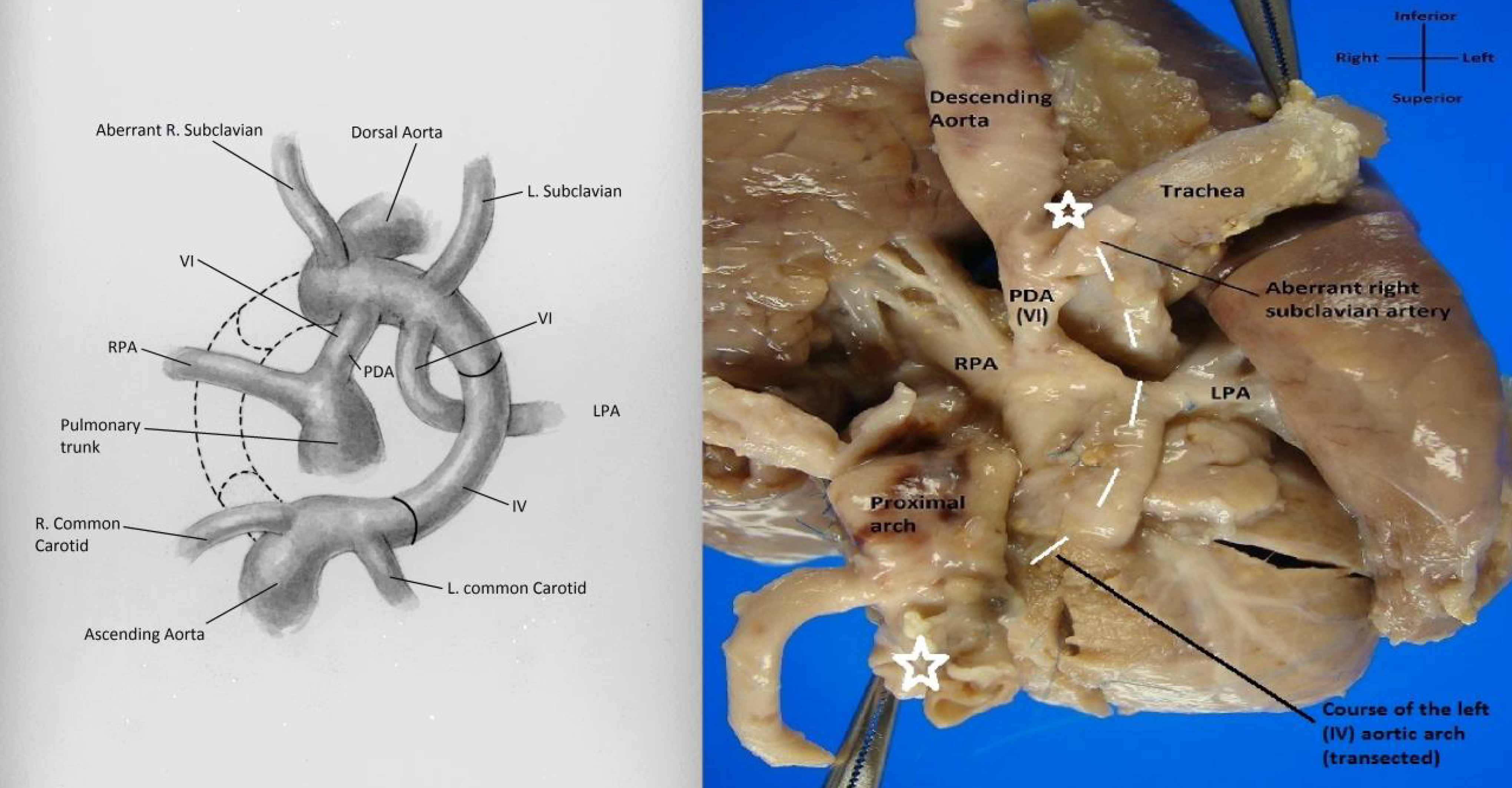
Left: There is complete regression of the right fourth and proximal sixth arches. The left pulmonary artery is connected to the aorta by the left sixth arch (arterial duct). The right sixth arch (arterial duct) completes the ring as it connects the descending aorta to the right pulmonary artery (illustration courtesy of Rebekah Dodson). Right: Autopsy specimen demonstrates a transected left aortic arch (stars denote transected edges, dotted line denotes the course of the left arch). The left pulmonary artery has been unifocalized to the pulmonary trunk, and the left (sixth) arterial duct has been divided. The right-sided arterial duct (PDA) connects the descending aorta to the right pulmonary artery. The trachea has been mobilized; it was completely encompassed by vascular structures (photography courtesy of Sarah Johnson-Welch, MD).
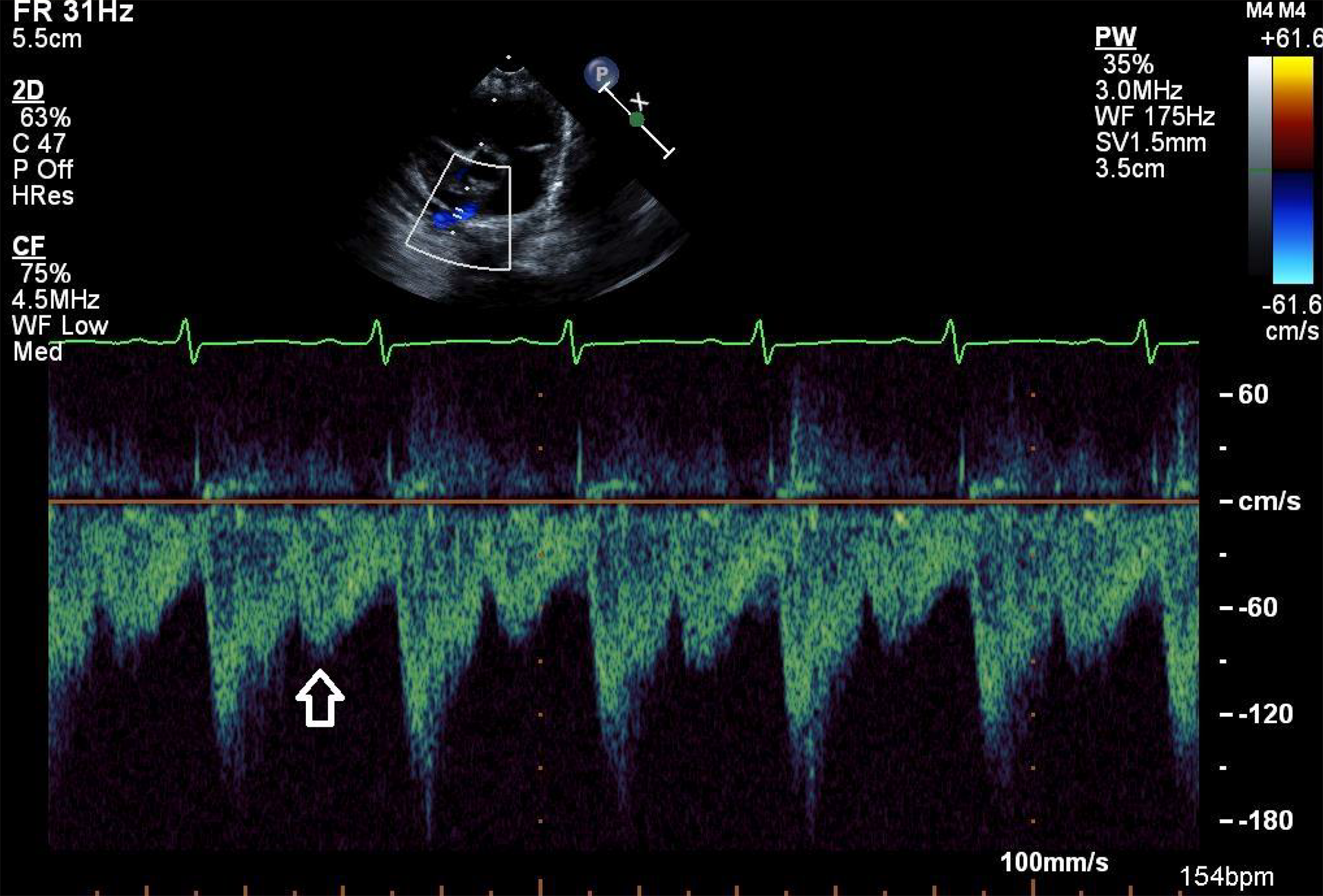
Antegrade diastolic flow (arrow) in the proximal right pulmonary artery.
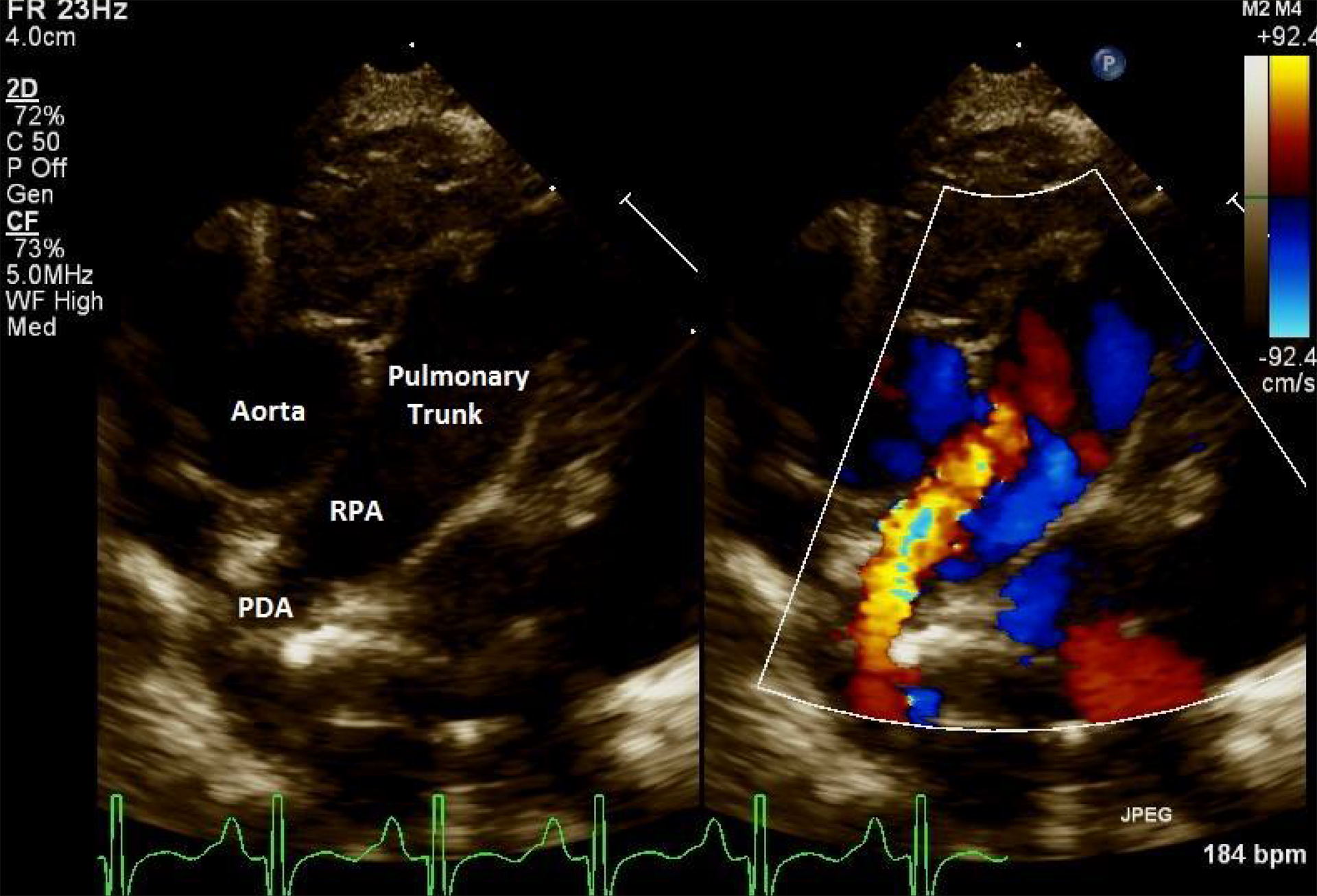
Parasternal short-axis view in two-dimensional imaging (left) and color (right) demonstrates the right arterial duct (PDA, red) into the right pulmonary artery (RPA).
Applying these lessons of echocardiographic assessment allowed prospective diagnosis in our second patient, who presented just two months after our first patient. Doppler interrogation of the proximal RPA demonstrated antegrade diastolic flow, and the descending aorta was midline at the level of the diaphragm. We diagnosed a left aortic arch with normal branching, right descending aorta, and right-sided arterial duct, which is an exquisitely rare type of vascular ring (Figure 5). This occurs due to the persistence of the fourth right arch, allowing for normal branching, whereas there is an interruption of the proximal right dorsal aortic root just distal to the origin of the right subclavian artery. The right-sided arterial duct maintains its connection to the descending aorta via the distal dorsal aortic root and is retroesophageal in course. Symptoms in this lesion depend on the size of the vascular ring and tend to be less severe than those produced by a double aortic arch. The retroesophageal portion of the aortic arch, nonetheless, regardless of the presence of an arterial duct or ligament, may itself cause symptoms depending on the degree of compression of the esophagus. 8 The diagnosis in our patient was confirmed both by CT scan and intraoperatively.
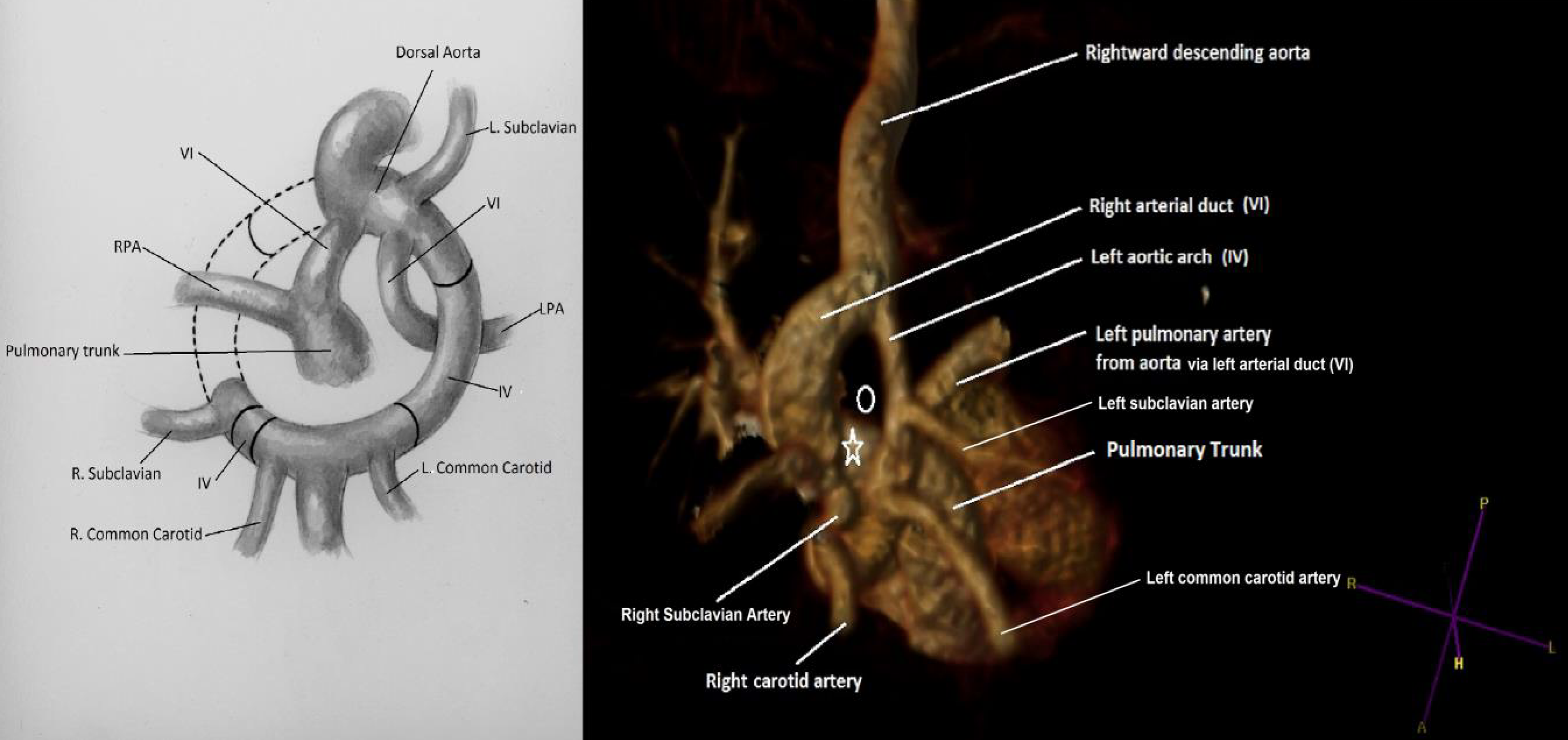
Left: Diagrammatic representation of a left aortic arch, normal branching with right-sided arterial duct (VI), and aortic origin of the left pulmonary artery (LPA) via the left arterial duct (VI; illustration courtesy of Rebekah Dodson). Right: Preoperative three-dimensional CT reconstruction—the right pulmonary artery (star) is connected to the pulmonary trunk and is discontinuous from the LPA (circle—location of the trachea and esophagus within the vascular ring).
Strikingly, both of these neonates with extremely rare vascular rings also had ductal origin of the LPA. Both had a mutual abnormality in development of the sixth arch arteries, with regression of the proximal left component and persistence of the distal right segment. This resulted in bilateral arterial ducts, with the left-sided duct feeding the LPA. The right duct, in the setting of a left aortic arch with a midline to rightward descending aorta, completed the vascular ring. This combination may appear to be coincidental, but its existence in two consecutive patients warrants recognition. Prior reports of absent LPA with rare vascular rings may represent ductal origin of the LPA, with closure of the arterial duct at the time of presentation. 9,10 While bilateral arterial ducts have previously been reported in the setting of ductal origin of a pulmonary artery, the aortic arch is usually on the opposite side to the abnormal pulmonary artery, and thus, a vascular ring is not formed. When ductal origin of a pulmonary artery occurs on the same side as the aortic arch, careful interrogation for bilateral arterial ducts should be undertaken. When both ducts are present, a vascular ring is formed. Failure to make the diagnosis may be catastrophic, as demonstrated in our first patient who died of an aortoesophageal fistula, a rare but known complication of unrecognized rings, thought to be secondary to direct injury resulting from manipulation of nasogastric tubes. 11 A thorough evaluation of the aortic arch anatomy should be undertaken, with particular detail to the presence of diastolic antegrade flow in the proximal RPA and the position of the descending aorta in relation to the midline. Attention to these findings should allow for prospective identification of these rare vascular rings. Three-dimensional reconstruction by CT angiography can assist in preoperative planning.
Footnotes
Authors’ Note
The families consented to publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.