
Abstract
Background:
Infants with shunt-dependent pulmonary blood flow are at risk for developing proximal pulmonary artery (PA) stenosis, which may result in morbidity and mortality. Transthoracic echocardiography (TTE) is the primary means of surveillance for PA narrowing but has significant limitations and has not been compared to computed tomographic angiography (CTA)–derived measurements of the proximal PA anatomy in this population.
Methods:
A retrospective chart review identified infants with shunt-dependent pulmonary blood flow who had both TTE and CTA performed <14 days apart during a five-year period. Proximal right pulmonary artery (RPA) and left pulmonary artery (LPA) diameters were measured by TTE and CTA. Pulmonary artery z-score, linear and intraclass correlation (ICC) coefficients, and Bland-Altman plots were computed.
Results:
Seventeen pairs of studies were analyzed. The TTE and CTA proximal PA diameters had moderate linear correlation and agreement (R = 0.67, P ≤ .0001, ICC = 0.65); the RPA showed stronger correlation and agreement (R = 0.76, P = .0004, ICC = 0.72) than the LPA (R = 0.59, P = .01, ICC = 0.59). Computed tomographic angiography detected missed PA stenosis (Z score < −2) in five (14.7%) cases, four of which were on the LPA.
Conclusion:
In this study of infants with shunt-dependent pulmonary blood flow, TTE and CTA proximal PA diameters had only moderate correlation and agreement overall, which was worse when comparing LPA measurements. This resulted in missed PA stenosis by TTE. Computed tomographic angiography may be warranted in patients with poorly visualized PAs by TTE or suspicion for deficient pulmonary blood flow.
Keywords
Introduction
The current management paradigm for infants with single-ventricle (SV) heart disease, such as hypoplastic left heart syndrome, includes an operation in the first days of life to establish unobstructed blood flow from the ventricle to the systemic arterial bed and a controlled source of pulmonary blood flow. 1 The source of pulmonary flow is a modified Blalock-Taussig (BT) shunt, central shunt, or right ventricle to pulmonary artery (PA) conduit. Infants with shunt-dependent pulmonary blood flow are at risk for developing proximal branch PA stenosis, 2 -5 resulting in reintervention, perioperative complications, and failure of passive cavopulmonary circulation en route to the Fontan operation. 1,6 -8 Transthoracic echocardiography (TTE) is the primary means of surveillance for PA narrowing after initial SV palliation but is limited by acoustic windows, operator experience, and requires patient cooperation. 9,10 Newer high-pitch computed tomographic angiography (CTA) scanning modes offer high spatial resolution, relatively low ionizing radiation, and rapid acquisition which has been useful in children with congenital heart disease and minimizes the need for sedation. 11 However, its role in interstage PA surveillance remains unknown. The purpose of this study was to compare TTE and CTA-derived measurements of the proximal PA diameters after initial palliation in infants with SV physiology and shunt-dependent pulmonary blood flow. We hypothesized that CTA-derived measurements of proximal PA diameters in this population would more accurately detect PA stenosis.
Materials and Methods
Design and Participant Selection
A retrospective chart review identified infants with shunt-dependent pulmonary blood flow (BT shunt, central shunt, or Sano conduit) who had both TTE and CTA performed less than 14 days apart between January 2010 and September 2015. Studies were included if they both occurred after stage 1 palliation and before any additional surgical or catheter-based intervention. Focused echocardiographic studies that did not evaluate the proximal pulmonary vasculature were excluded. The institutional review board of University of Colorado approved the present study.
Imaging Protocols and Analysis
Transthoracic echocardiography
Echocardiography was performed using a Vivid 7 (GE Healthcare, Milwaukee, Wisconsin) or iE33 (Philips Medical Systems, Andover, Massachusetts) platform, with probe frequencies appropriate for body habitus. Echocardiograms were reviewed offline, using commercially available software (AGFA Healthcare Cardiovascular Review Station version 2.14.03, Mortsel, Belgium). Measurements of proximal PA diameter were made in a fashion identical to the clinical practice of echocardiographers at our center; more specifically, the proximal branch pulmonary arteries were imaged primarily in the parasternal short-axis view, unless poor echocardiographic windows prevented adequate visualization. In this case, the pulmonary arteries were measured from the suprasternal or subcostal windows preferentially, then any available off-axis window to obtain an accurate measurement. Pulmonary artery diameter was measured at its smallest diameter prior to the origin of the first right and left segmental branches. All measurements were performed by a single investigator (M.D.).
Computed tomographic angiography
Nonsedated, free-breathing CTA examinations were performed after the administration of 2 mL/kg of iodinated contrast (Optiray 320, Mallinckrodt, Inc., St. Louis, MO, USA). All CTA examinations were performed on a second-generation dual-source Somatom Definition FLASH CT scanner (Siemens AG, Forchheim, Germany). Gantry rotation time was 280 milliseconds, collimation was 0.6 mm, and temporal resolution was 75 milliseconds. Scans were performed with high-pitch (3.4) helical techniques with prospective electrocardiogram triggering and a tube potential of 70 kV. Online tube current modulation was used. Iterative reconstruction was used for image processing. Information regarding radiation dose was obtained using Radimetrics (Bayer HealthCare, Whippany, New Jersey). Radimetrics extracts dose metrics through direct connections with the patient archiving and communication systems and calculates organ doses which are used to compute effective doses using published International Commission on Radiological Protection tissue-weighting factors. 12 All CTA measurements were performed using the same landmarks by a single investigator (D.E.). Measurements were obtained in orthogonal planes using multiplanar reconstruction on an OsiriX viewer (http://www.osirix-viewer.com/; Figure 1). The average of both measurements was calculated and used for all analyses.
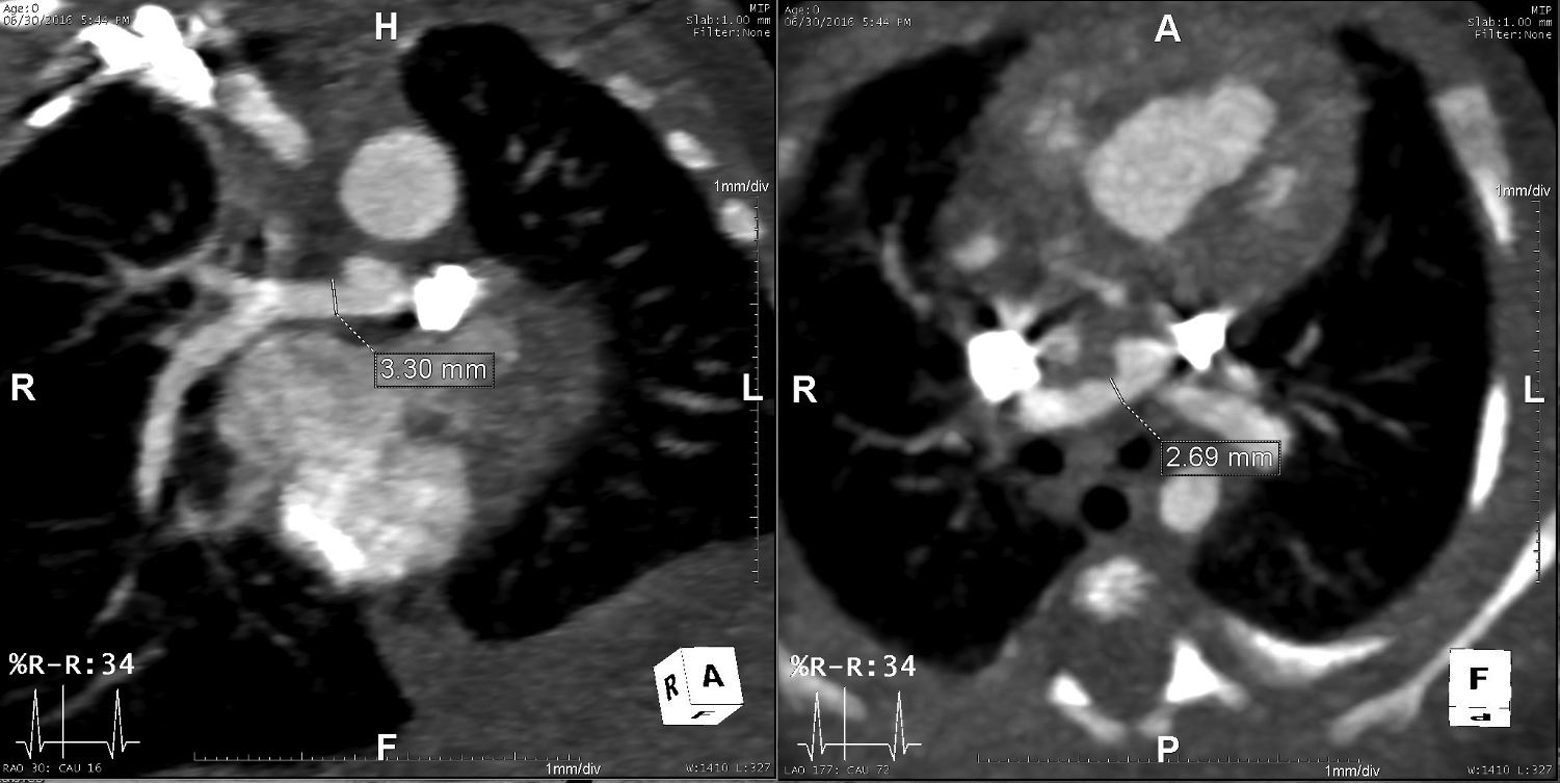
Measurement of the proximal pulmonary arteries by computed tomographic angiography (CTA) using orthogonal planes.
Statistical Analyses
All data are presented as median with interquartile range, mean with standard deviation, or percentage, when appropriate. Since no age and gender-specific, body surface area (BSA)–indexed CTA norms for proximal pulmonary arteries exist, Boston z-scores for echocardiographic data were applied to both CTA- and TTE-derived measurements to allow for meaningful comparison. 13,14 Similar methodology has been used in prior studies. 15 The PA stenosis was defined a priori as a z-score ≤ −2. The PA measurements were compared using Pearson and intraclass correlation (ICC) coefficients and were analyzed over the range of PA values using Bland-Altman plots.
Results
Participant Characteristics
Seventeen pairs of studies met the inclusion criteria (Table 1). The median age at TTE was 38 days (24-76 days), and the majority of patients were male (64.7%). Sixty-five percent had hypoplastic left heart syndrome and 58.8% underwent a BT shunt. The median BSA was 0.23 m2 (0.20-0.26 m2). The median interval between imaging studies was 1 day (1-2 days). The most common indication for obtaining the CTA was refractory hypoxemia (52.9%), defined as oxygen saturations persistently less than expected for physiology.
Characteristics of the Study Population.
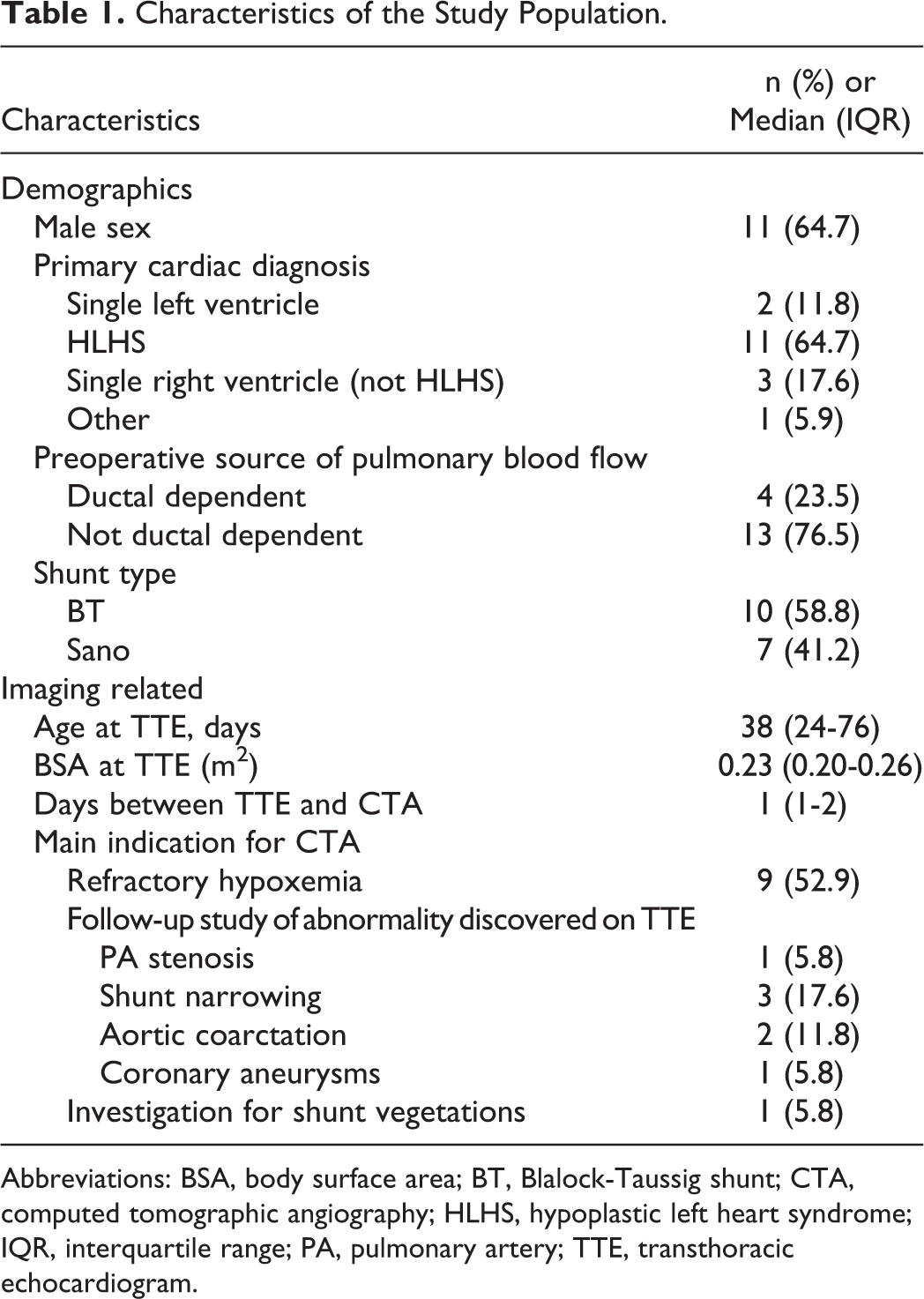
Abbreviations: BSA, body surface area; BT, Blalock-Taussig shunt; CTA, computed tomographic angiography; HLHS, hypoplastic left heart syndrome; IQR, interquartile range; PA, pulmonary artery; TTE, transthoracic echocardiogram.
Proximal PA Measurements
Proximal PA measurements ranged from 2.0 to 5.8 mm (Table 2). An analysis of all proximal PA diameters combined yielded a moderate linear correlation and agreement between TTE and CTA (R = 0.67, P ≤ .0001, ICC = 0.65; Figure 2A). There was significant variation but no systematic bias over the range of all PA diameters determined by Bland-Altman analysis (Figure 2B). On subgroup analysis, right pulmonary artery (RPA) measurements showed a stronger linear correlation and agreement (R = 0.76, P = .0004, ICC = 0.72; Figure 3A) than left pulmonary artery (LPA) measurements (R = 0.59, P = .01, ICC = 0.59; Figure 3B). Bland-Altman plots did not indicate systematic bias of either the RPA or LPA measurements (Figure 4). Computed tomographic angiography detected five cases of PA stenosis that was missed by TTE (14.7% of cases, mean difference 0.25 ± 0.69 mm), and four of these instances were measurements of the LPA compared to one case on the RPA, though this was not statistically significant (Fisher exact P = .34). Sensitivity and specificity for PA stenosis by TTE was 58% and 32%, respectively, using CTA as a reference for comparison. Two (11.8%) patients underwent surgical or catheter-based intervention as a result of the CTA, but none of these were on the proximal pulmonary arteries (stenting of occluded BT shunt resulting in resolution of hypoxemia, repair of aortic coarctation). The median radiation dose (CT dose index volume), dose-length product, and effective age- and size-adjusted radiation dose were 0.4 mGy (0.1-0.6 mGy), 8 mGy·cm (3-11 mGy·cm), and 0.31 mSv (0.1-0.8 mSv), respectively.
Pulmonary Artery Measurements (mm) of the Study Population.
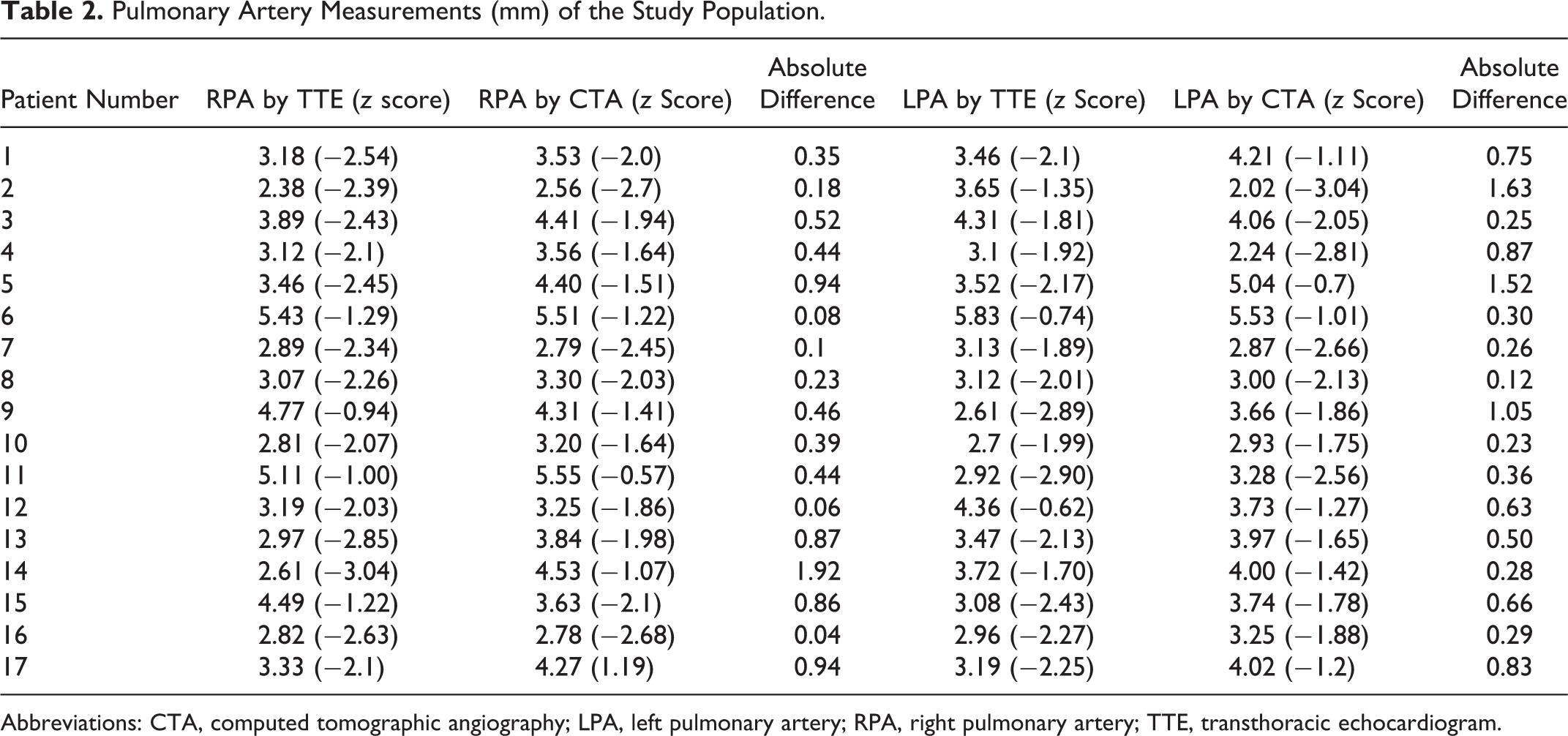
Abbreviations: CTA, computed tomographic angiography; LPA, left pulmonary artery; RPA, right pulmonary artery; TTE, transthoracic echocardiogram.
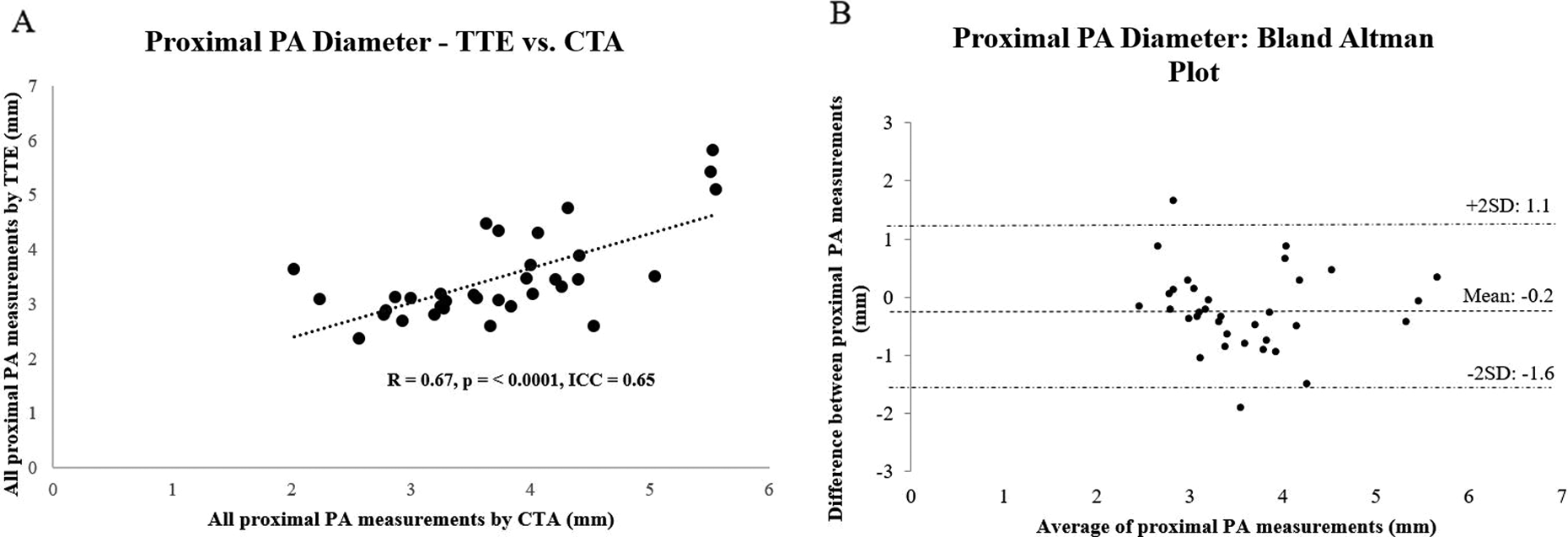
A, Linear correlation plot between transthoracic echocardiography (TTE) and computed tomographic angiography (CTA) on all proximal pulmonary artery (PA) measurements. B, Bland-Altman plot of TTE and CTA on all proximal PA measurements.
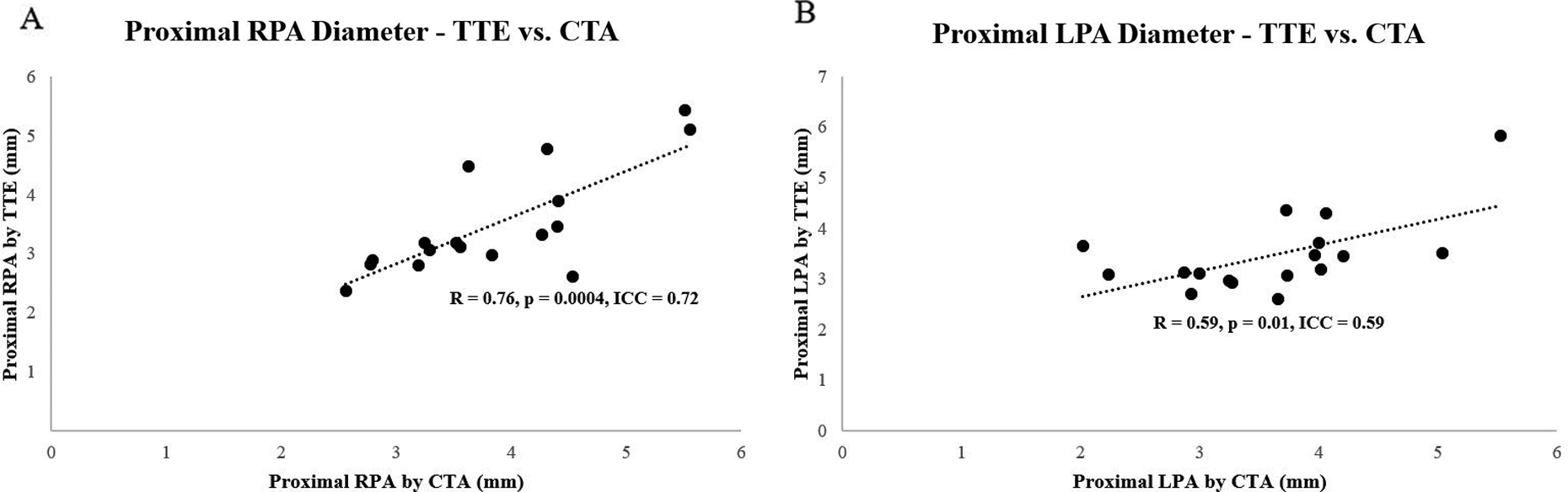
A, Linear correlation plot between transthoracic echocardiography (TTE) and computed tomographic angiography (CTA) on right pulmonary artery (RPA) measurements. B, Linear correlation plot between TTE and CTA on left pulmonary artery (LPA) measurements
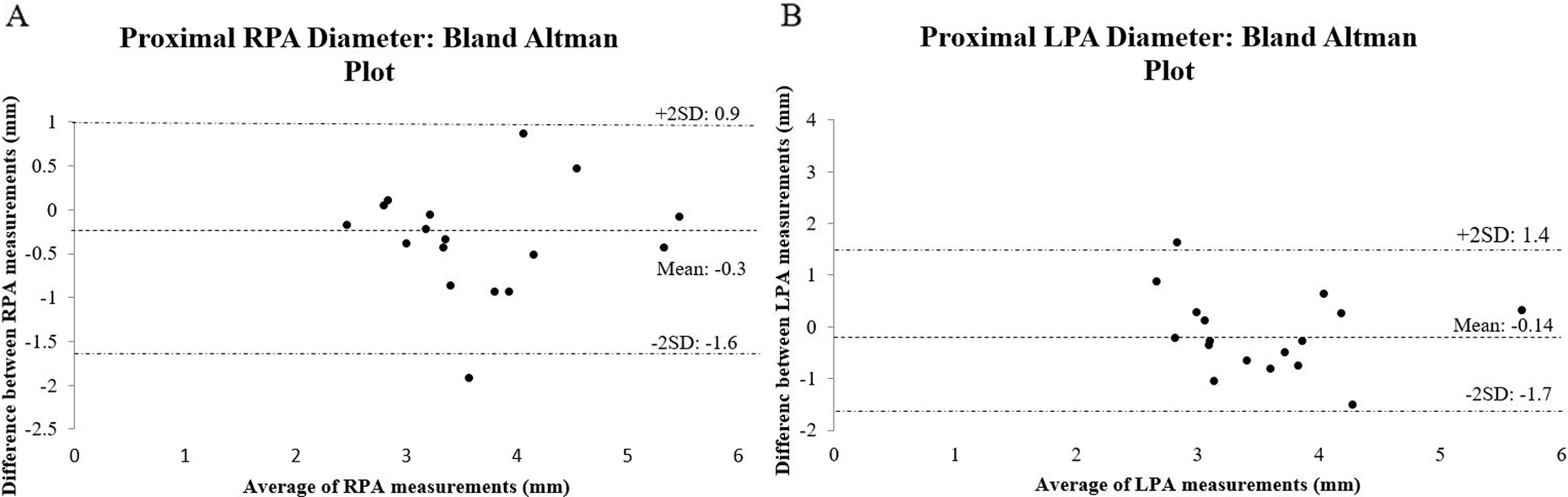
A, Bland-Altman plot of proximal right pulmonary artery (RPA) measurements. B, Bland-Altman plot of left pulmonary artery (LPA) measurements.
Comment
In this retrospective analysis of proximal PA measurements in infants with shunt-dependent pulmonary blood flow, TTE measurements were only moderately correlated with CTA measurements, with weaker correlation and agreement of the LPA. This resulted in five cases of missed PA stenosis by TTE that were detected by CTA, which suggests that CTA may be more accurate in detecting PA stenosis in this high-risk population.
Pulmonary artery growth is crucial during initial palliation for SV congenital heart disease in order to create the substrate for successful cavopulmonary anastomoses. Branch PA stenosis in this cohort has significant consequences, leading to prolonged hospitalization and increased short-term mortality. 16 -22 The scope and importance of this problem should not be understated, as 33% to 43% will develop angiographically or surgically confirmed proximal PA stenosis prior to their stage 2 operation, 7,23 many of which require intervention. The current practice at most centers is to periodically screen for proximal PA stenosis using TTE. However, few studies have been performed to date illustrating the accuracy of TTE-based measurements in this population, relative to CTA as a reference for comparison. Computed tomographic angiography generally performs excellently relative to angiography and surgery in delineating complex cardiac anatomy and is therefore commonly used as a reference for comparison in imaging comparison studies. 24,25
Only two studies have been performed to date that specifically compared TTE to CTA in measuring thoracic vessels in patients with congenital heart disease. Shi and colleagues compared both TTE and CTA measurements of the pulmonary arteries with surgical measurements among patients (median age 28 months) with cyanotic congenital heart disease. 26 They did not compare TTE and CTA directly but did find an excellent correlation between CTA and surgical measurements (r = 0.95, 0.96, and 0.97 for the main pulmonary artery (MPA), RPA, and LPA; P < .001) compared to only moderate correlation between TTE and surgical measurements (r = 0.61-0.84; all P < .001). They concluded that CTA is a more reliable and accurate modality for measuring the pulmonary arteries in pediatric cardiac surgical patients than TTE. Chandrashekhar et al compared angiography, CTA, and TTE-derived measurements of the pulmonary arteries in a cohort of patients aged 2 months to 20 years with cyanotic congenital heart disease. 25 They demonstrated that CTA identified 17 total cases of subjective PA stenosis, of which 14 were missed by TTE.
Madan et al compared PA and proximal aortic measurements obtained by contrast-enhanced magnetic resonance angiography (CE-MRA) and TTE among infants and children with congenital heart disease. 15 The median age in their cohort was four months, and approximately 25% had SV anatomy. They found excellent correlation between CE-MRA and TTE (r = 0.94, P < .0001). However, in a subanalysis of 50 of the 129 measurements with the greatest discordance (>1 mm), they found that 13 (26%) of 50 were “incorrectly classified,” in which one measurement suggested stenosis (Z score ≤ −2) and the other did not. They did not perform an isolated analysis of the proximal pulmonary arteries.
Our results differed from those by Madan et al citing strong correlations between TTE-based measurements and a cross-sectional imaging reference for comparison. We found that there was only moderate linear correlation and agreement between TTE- and CTA-based proximal PA measurements among infants with shunt-dependent pulmonary blood flow. This may be explained by many factors. First, our cohort’s median age at TTE was just over one month old with small branch PA sizes ranging from 2.0 to 5.8 mm compared to the older patients in the study by Madan et al. Furthermore, our study population had a higher risk for having tortuous pulmonary arteries with an atypical course that did not fall into a single imaging plane, which may have resulted in inaccurate measurement. Finally, measurements between TTE and CTA were not always made in analogous dimensions, which may have implications on the correlation when the measured PA shape is not perfectly tubular. However, in the study by Madan et al, there was no significant differences between proximal thoracic measurements made in analogous versus orthogonal planes. 15
The majority of our missed PA stenosis occurred on the left side, a phenomenon also noted in the data of Madan et al. 15 This may be a result of the fact that the LPA is more difficult to image by TTE as it dives posteriorly and inferiorly adjacent to the aorta. The tendency to miss LPA stenoses is especially concerning since the LPA may be more vulnerable to impaired growth in patients with modified BT shunts. 5 In one large series that followed infants after the Norwood procedure, approximately 20% of patients required proximal PA catheter-based intervention during the interstage period, with all but two cases occurring on the LPA. 7
Two patients underwent surgical or catheter-based interventions resulting in resolution of the clinical concern based on the CTA findings, though none of these were on the proximal pulmonary arteries. Among our study cohort, the magnitude of PA stenosis detected by CTA tended to be relatively mild. This may explain why no additional interventions were performed on the pulmonary arteries immediately after the CTA. The detection of predominantly mild stenosis may be related to the fact that the median age at CTA was approximately 40 days and PA stenosis in the interstage population may worsen over time. Indeed, three patients underwent PA plasty at the time of their Glenn operation. Hypoxemia in this population can be multifactorial, and the PA narrowing identified by CTA early during the interstage period may have played a contributory role in some patients.
Study Limitations
Our findings should be interpreted in the context of important limitations. First, this was a relatively small, retrospective study at a single center. Inferences to the interstage population at large would benefit from a larger sample size, which is likely to require a multicenter collaboration. The retrospective nature of this analysis limited our ability to manipulate TTE windows in order to more accurately visualize the pulmonary arteries.
Finally, it is difficult to make definitive conclusions between two imaging modalities when measurements are made in nonanalogous planes. Prior studies have been methodologically rigorous in comparing analogous planes and have found much higher correlations. 15 However, our study was intended to simulate realistic conditions in which measurements of the pulmonary arteries during the interstage period can only be obtained from TTE imaging planes not analogous to those employed in CTA. Indeed, clinical decisions are often made with this implicit understanding.
Conclusion
In this study of infants with shunt-dependent pulmonary blood flow, assessment of proximal PA size by TTE versus CTA had only moderate correlation and agreement overall, with poorer correlation of the LPA measurements compared to the RPA. Transthoracic echocardiography did not detect proximal LPA stenosis relatively frequently. In this population at high risk for circulatory failure due to PA obstruction, CTA may be warranted in patients with poorly visualized PA morphology by TTE or clinical suspicion for deficient pulmonary blood flow.
Footnotes
Authors’ Note
The authors had full control of the design of the study, methods used, outcome parameters, analysis of data, and production of the written report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.