
Abstract
Background:
Postoperative care delivered in the pediatric cardiac intensive care unit (CICU) relies on providers’ understanding of patients’ congenital heart defects (CHDs) and procedure performed. Novel, bedside use of virtual, three-dimensional (3D) heart models creates access to patients’ CHD to improve understanding. This study evaluates the impact of patient-specific virtual 3D heart models on CICU provider attitudes and care delivery.
Methods:
Virtual 3D heart models were created from standard preoperative cardiac imaging of ten patients with CHD undergoing repair and displayed on a bedside tablet in the CICU. Providers completed a Likert questionnaire evaluating the models’ value in understanding anatomy and improving care delivery. Responses were compared using two-tailed t test and Mann-Whitney U test and were also compared to previously collected CICU provider responses regarding use of printed 3D heart models.
Results:
Fifty-three clinicians (19 physicians, 34 nurses/trainees) participated; 49 (92%) of 53 and 44 (83%) of 53 reported at least moderate to high satisfaction with the virtual 3D heart’s ability to enhance understanding of anatomy and surgical repair, respectively. Seventy-one percent of participants felt strongly that virtual 3D models improved their ability to manage postoperative problems. The majority of both groups (63% physicians, 53% nurses) felt that virtual 3D heart models improved CICU handoffs. Virtual 3D heart models were as effective as printed models in improving understanding and care delivery, with a noted provider preference for printed 3D heart models.
Conclusions:
Virtual 3D heart models depicting patient-specific CHDs are perceived to improve understanding and postoperative care delivery in the CICU.
Introduction
Congenital heart disease (CHD) remains the most common type of birth defect, with an incidence of 75 affected newborns per 1,000 live births, 1 and about 25% of children with CHD will require treatment, including operative repair. During their procedure and recovery, they will be cared for by different types of providers in the cardiac intensive care unit (CICU), each with a specific and important role. Care delivered to these children and adults with CHD is typically informed by standard cardiovascular imaging, which requires expertise to interpret and can be limited in its ability to demonstrate the full complexity of CHD. Recent studies have demonstrated a positive impact of patient-specific, three-dimensional (3D) printed models of CHD prior to initiation of patient care, both in preparation for a procedure 2 –6 and in postprocedural care delivery. Specifically, they were noted to increase confidence in a planned procedure, knowledge retention about the defect, quality of the care team handoff, and provider confidence when prepared with 3D models of patient-specific CHD. 7
The 3D models of CHD are derived from high-quality, 3D cardiovascular imaging, including cardiac computed tomography (CT), magnetic resonance (MR), and echocardiography, 8,9 and can be displayed three dimensionally either in printed form or virtual form. The expanding availability of 3D printing technology and significant advances in printing capabilities in recent years have proved to be assets in medical care and applications. 10,11 However, display of cardiac defects by a 3D printed model can be expensive and is constrained by the chosen “cut plane” to view the cardiac defect through. In addition, 3D printed models are not easily manipulated, magnified, labeled, measured, or shared, making collaboration difficult. Hence, a dynamic and user-friendly 3D digital platform that provides more fluidity when interacting with the model may be superior and add better value to current two-dimensional displays and printed 3D model display.
Multiple software tools are available for producing virtual 3D models reconstructed from patient imaging. 12,13 However, these products are generally of low resolution, can only display images of a particular vendor, are difficult to manipulate, and are not designed to meet the specific needs of collaborative imaging review. An immersive 3D digital display software, called Cardiac Review 3D (Indicated LLC, Pennsauken, New Jersey), was developed that has the ability to interactively display patient-specific 3D digital heart models on a tablet device, which can be easily used at the clinical bedside. The display software was developed according to specifications from our team of engineers, cardiologists, cardiovascular surgeons, and intensive care unit (ICU) providers to include tools to label and measure the heart model, with a simple, streamlined display that allows for care team engagement. This is in contrast to many other 3D object tools which have a complex interface and contain tools to engineer different shapes which are not useful and not appropriate for the caregiver setting.
Thus, the objective of this study was to evaluate the utility of virtual 3D heart models displayed using custom, digital software in providing patient-specific, “just-in-time” training for CICU providers caring for postoperative patients.
Material and Methods
Clinical Study Design and Workflow
This prospective study was approved by Children’s National’s Institutional Review Board and consent was obtained where appropriate. Bedside CICU providers of ten consecutive patients admitted to the CICU following a surgery for CHD, who also had 3D cardiovascular imaging data sets obtained as part of their clinical care, were selected for this study using Cardiac Review 3D. All patients included in this study had virtual 3D heart models created from their 3D imaging data sets. Cardiovascular images were anonymized, exported into segmentation software (Mimics Innovation Suite software; Materialise, Leuven, Belgium), and a 3D digital model was created through a combination of thresholding and semiautomatic, edge detection segmentation methods to capture anatomic contours, as shown in Figure 1. Models were generated by experienced members of the 3D Cardiac Lab, a collaboration between cardiologists and biomedical engineers. Models were occasionally decreased in size as much as 33% to save money on printer material costs, provided display was not compromised. Each case was rated for complexity using the Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery (STS-EACTS) Congenital Heart Surgery Mortality Score. 14
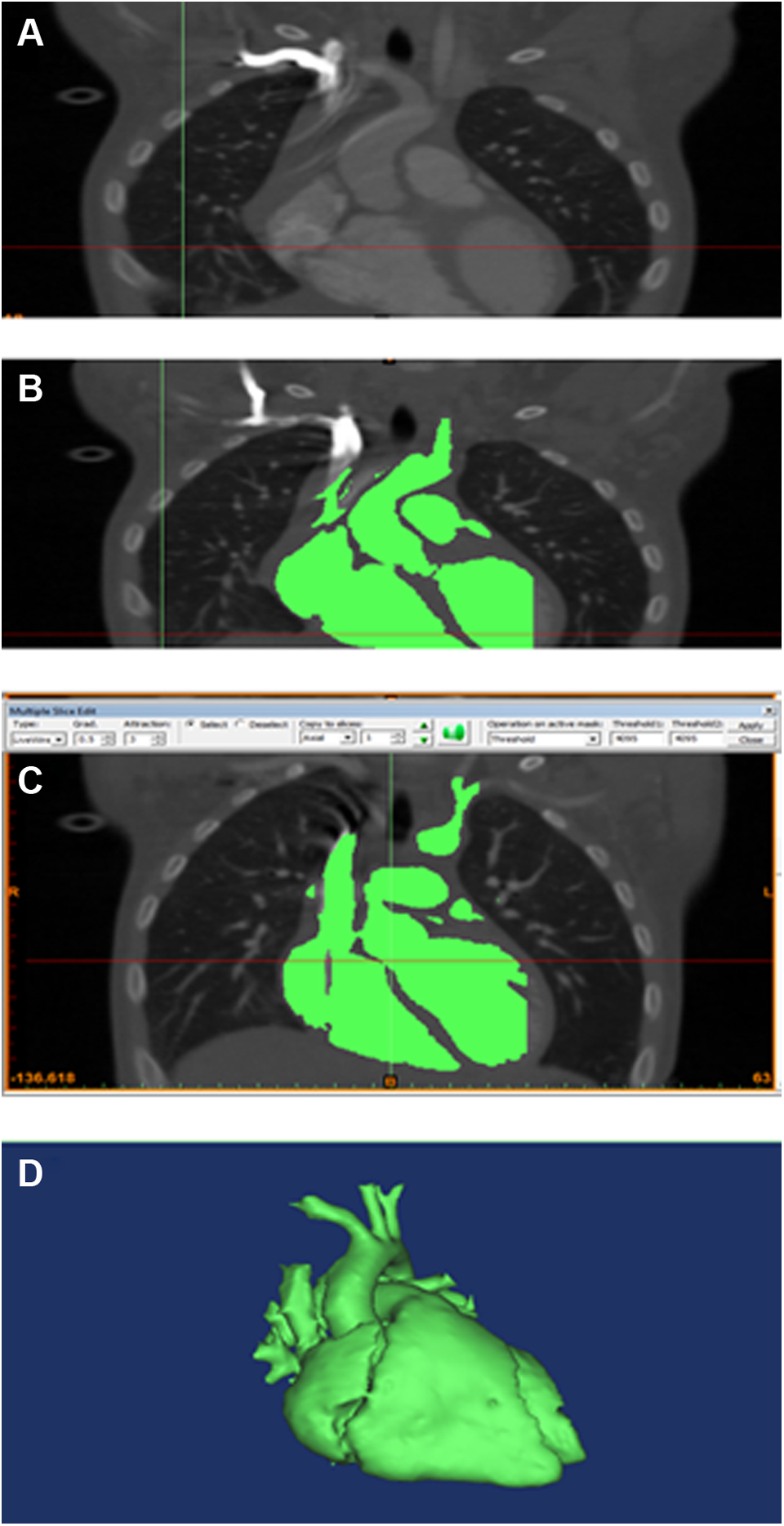
Screenshots of segmentation of CT image data set displaying segmentation process of the second case (left pulmonary artery sling): (A) plain CT images, (B) applying basic thresholding, (C) manually editing the mask, (D) final 3D model. 3D indicates three-dimensional; CT, computed tomography.
Next, 3D digital models were exported to a tablet computer preinstalled with the Cardiac Review 3D software and a labeled workspace was created which contained the patient-specific 3D digital model and a brief document with pertinent information regarding the preoperative anatomy, type of surgical repair, and potential postoperative complications for that patient. Clinical material was directed at surveillance for and treatment of known postoperative complications in the first 72 hours following surgery. This tablet was made available to providers on a voluntary basis, “just-in-time,” on the morning of the surgery, prior to admission to the CICU, and resided at the bedside to be available for use during the CICU admission as care teams handed off to one another, as shown in Figure 2. All participants were briefly introduced to the 3D Cardiac Review application and, on their own time, completed a patient-specific session using the application and reading through a brief, 2-page clinical summary file of their patient created using the application. Team members interacted with the same workspace and PDF of the patient’s clinical file, but individually so that the whole team participated in asynchronous “just-in-time” simulation.
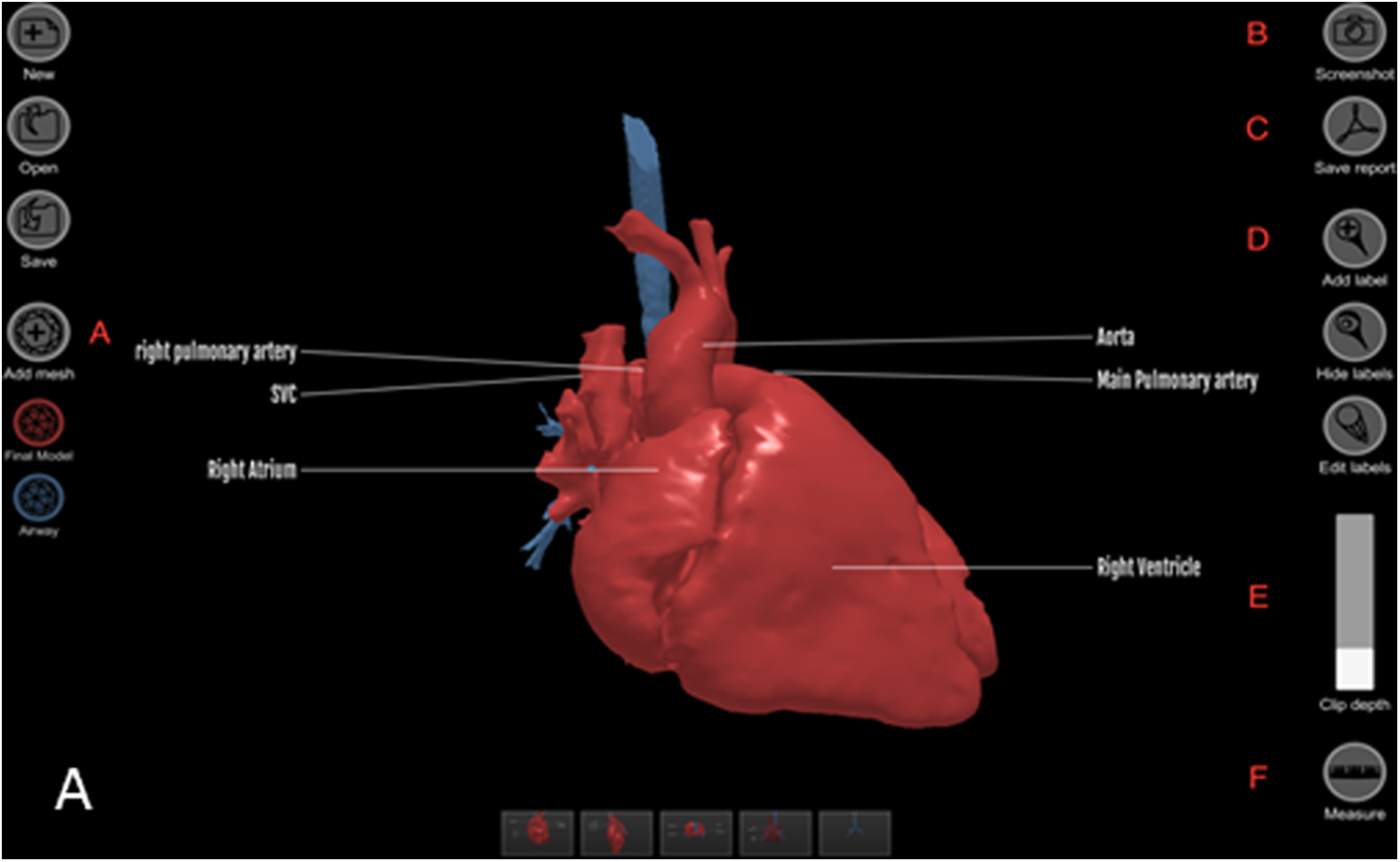
A screenshot of the Cardiac Review 3D software displaying a left pulmonary artery sling with annotated functions. A, Add a new 3D object file. The software can display up to 4 coregistered surface models simultaneously, (B) capture a screenshot, (C) export a PDF report, (D) add a new label to the 3D model, (E) clip function to visualize the interior anatomy, and (F) linear measurement tool. 3D indicates three-dimensional.
Users then gave feedback via surveys designed to gauge the utility of the digital display software as it compares to standard patient handoff, which includes clinical details and a hand-drawn cartoon of the patient’s surgery, but no collaborative review of imaging or models. Feedback was given through a constructed questionnaire with a 10-point Likert-type scale, consisting of eight questions discussing in what capacity an interactive 3D digital model at the patient bedside could improve the understanding of the care provider in three main areas: type of the heart defect, type of the surgical repair, and anticipating clinical complications that may follow the surgery.
Statistical Analysis
Univariate analysis comparing participant responses was carried out using the nonparametric Mann-Whitney U-test, stratified by provider type. Percentages were compared using Fisher exact text. Multivariable logistic regression was applied to compare odds of moderate to high Likert scores (7 or higher on 10-point scale), suggesting perceived high value among providers evaluating printed 3D versus virtual 3D heart models controlling for provider type (nurse, physician) and previous familiarity. Median scores and interquartile range from the ten cases using the virtual 3D models were compared to previously reported scores using printed 3D models in a group learning session with the Mann-Whitney U test. Statistical analysis was performed with IBM SPSS Statistical software (version 23.0, IBM Corporation, Armonk, New York). Two-tailed P < .05 was considered statistically significant.
Results
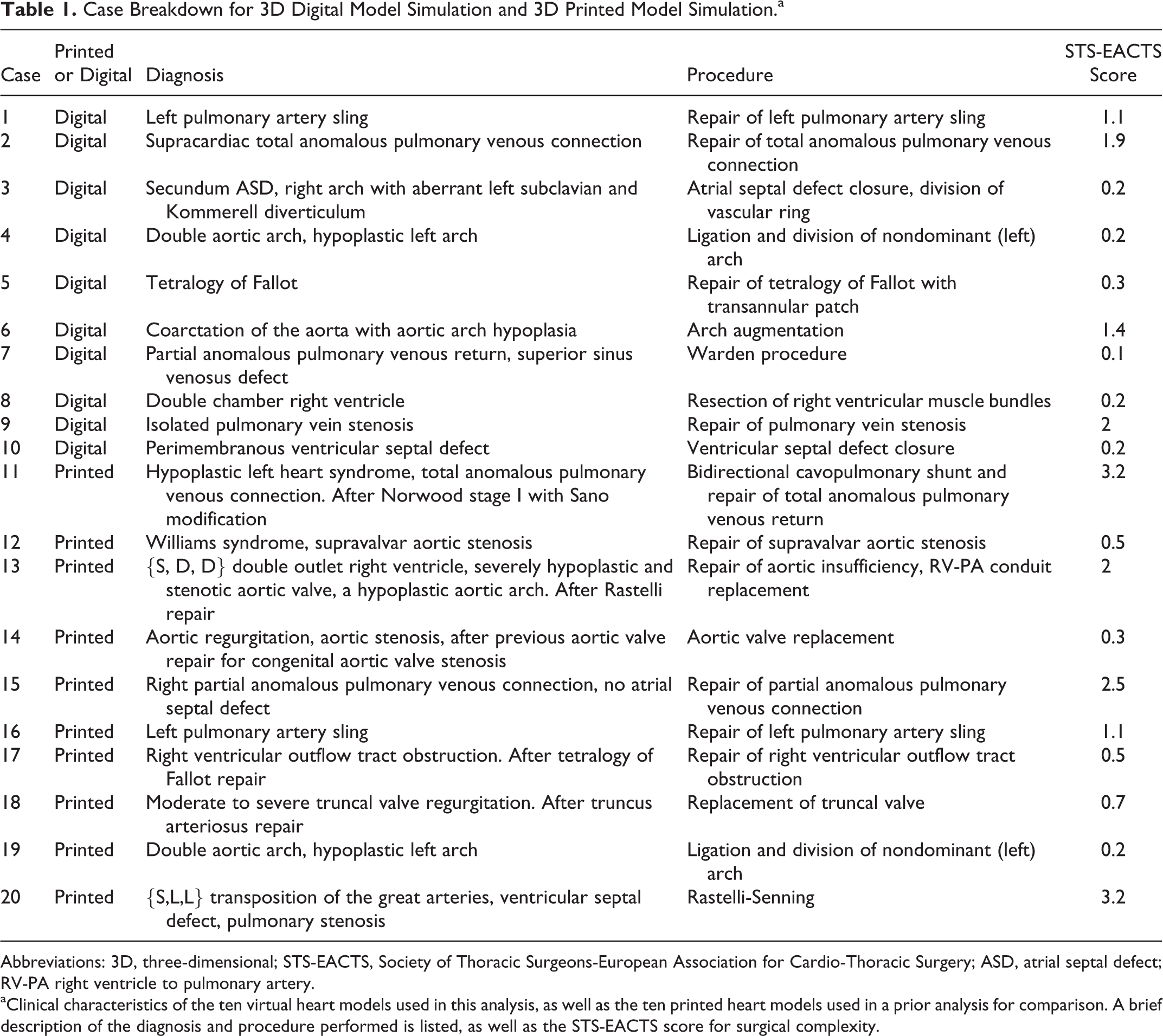
Fifty-three pediatric cardiac intensive care clinicians enrolled in the study, including 19 intensive care physicians (4 attendings and 15 fellows) and 34 critical care nurses (29 nurses and 5 trainees). Provider types were evenly distributed across each simulation, with 3 to 5 participants per case who made up the bedside care team in the immediate postoperative period. The ten cases had an average STS-EACTS score of 0.76 (range: 0.1-1.9). Responses from this virtual 3D heart experiment were compared to a previously published, identical experiment using printed models in the same CICU provider population with 70 provider participants caring for ten CICU cases with an average STS-EACTS score of 1.4 (range: 0.2-3.2). 7 An identical study questionnaire was administered after use of the printed model. Table 1 lists the clinical characteristics of the ten cases used in the virtual 3D heart model simulation experiment, as well as the ten previously published cases used in the printed 3D heart model experiment.
Case Breakdown for 3D Digital Model Simulation and 3D Printed Model Simulation.a
Abbreviations: 3D, three-dimensional; STS-EACTS, Society of Thoracic Surgeons-European Association for Cardio-Thoracic Surgery; ASD, atrial septal defect; RV-PA right ventricle to pulmonary artery.
aClinical characteristics of the ten virtual heart models used in this analysis, as well as the ten printed heart models used in a prior analysis for comparison. A brief description of the diagnosis and procedure performed is listed, as well as the STS-EACTS score for surgical complexity.
Impact of Virtual 3D Heart Model on Care
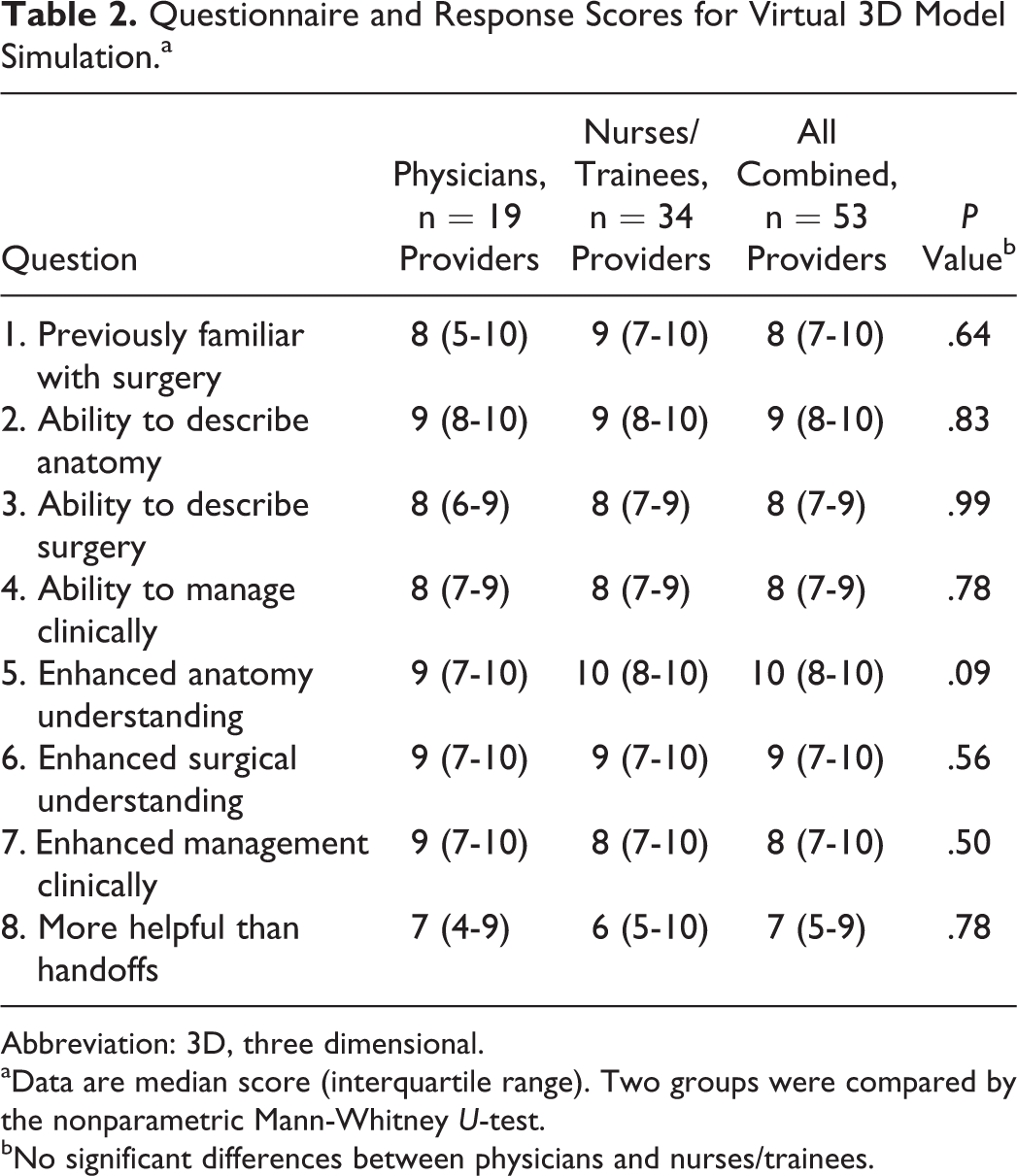
Table 2 lists the questionnaire responses by provider type using the virtual models on the novel bedside tablet application. Other than self-reported previous familiarity with cardiac surgery specific to the providers’ just-in-time case, there was no difference between the provider type (nurse vs physician) in terms of the perceived benefits realized with the use of the virtual 3D model and how it impacted their understanding of the anatomy, surgical repair, and navigating potential postoperative issues. When controlling for previous familiarity, 49 (92%) of 53 and 44 (83%) of 53 participants reported moderate to high levels of agreement (score at least 7) that the virtual 3D model enhanced anatomic understanding and surgical repair comprehension, respectively.
Questionnaire and Response Scores for Virtual 3D Model Simulation.a
Abbreviation: 3D, three dimensional.
aData are median score (interquartile range). Two groups were compared by the nonparametric Mann-Whitney U-test.
bNo significant differences between physicians and nurses/trainees.
There were no statistically significant differences in perceived value of the model (questions 5-8) for simple versus complex heart defects (defined by STS-EACTS score >1 and <1) and between trainees and professionals (both nurse and MD) other than the model’s enhancement of anatomic understanding (professionals 10 [9-10] vs trainees 9 [7-10], P = .04). Table 3 summarizes percentage of moderate to high levels of agreement (score greater than 7) by provider type. Of 53, 38 (71%) of the participants had a moderate to high level of agreement with the statement that the virtual 3D model improved their ability to manage potential postoperative problems. The majority of both groups (63% of physicians and 53% of nurses) agreed that use of the tablet with virtual 3D model was an improvement over the standard handoff process in the CICU. The bedside virtual tablets were often utilized during handoff to demonstrate surgical details to oncoming teams unfamiliar with the patient.
Percentages Indicating Moderate to High Level of Agreement (At Least 7 on 1-10 Likert Scale).a
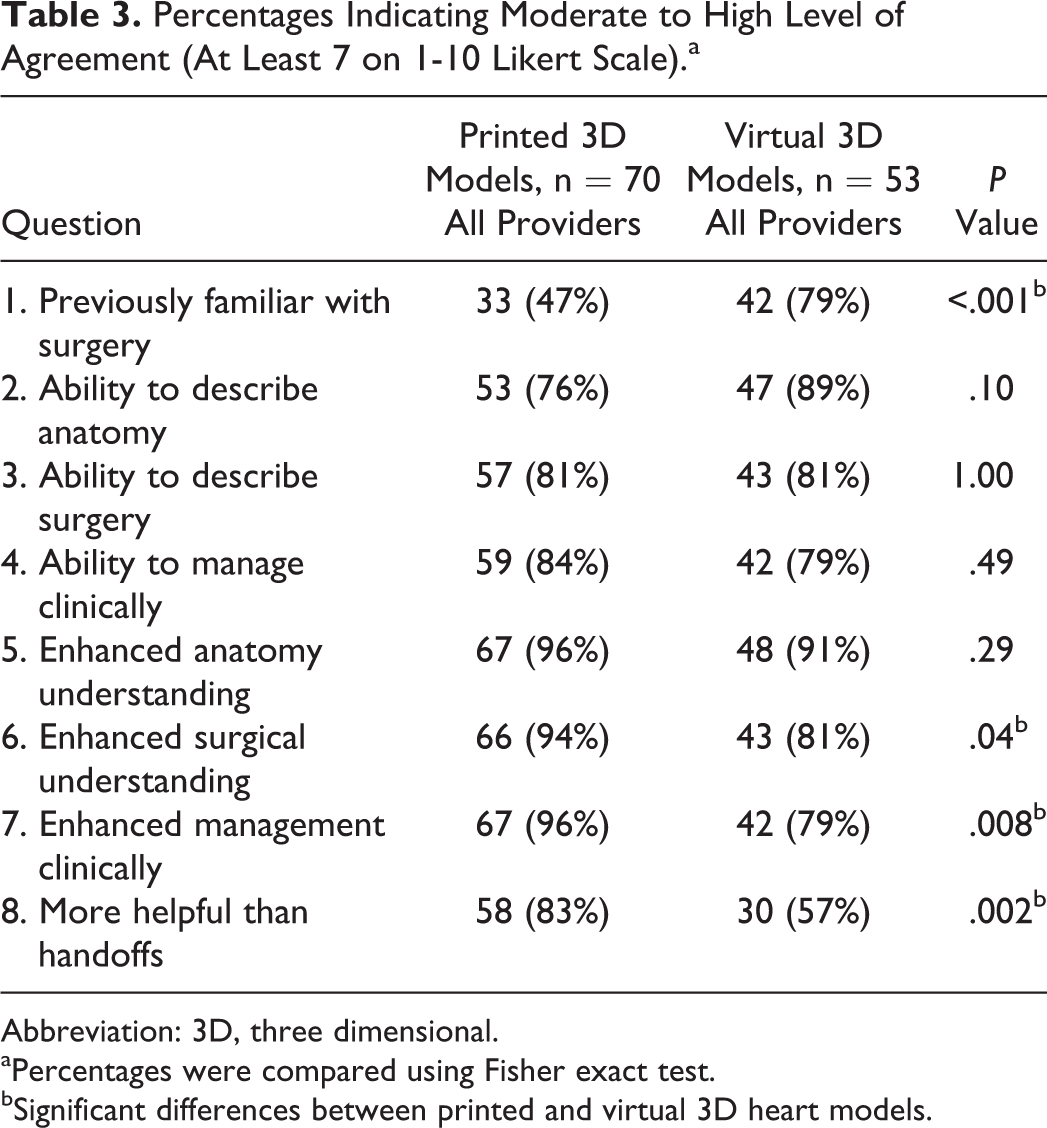
Abbreviation: 3D, three dimensional.
aPercentages were compared using Fisher exact test.
bSignificant differences between printed and virtual 3D heart models.
Impact of Printed Versus Virtual Models
Table 3 shows responses using the virtual 3D heart model compared to response using the printed 3D heart model when controlling for previous familiarity. All responses regarding the impact of the models on care delivery, handoff, and understanding were favorable (greater than 4) among all participants, regardless of virtual or printed model use. Printed models scored higher among CICU providers in their perceived ability to help care providers manage patients (96% vs 79% gave a score greater than 7, P = .008 for printed vs virtual, respectively) and handoff care of their patient (83% vs 57% gave a score greater than 7, P = .002 for printed vs virtual, respectively). Table 4 shows the same responses but grouped by provider type. Regarding the introduction of either type of model into the clinical care setting, there were no significant differences noted in any responses for both nurses and physicians and there were high rates of satisfaction among all clinicians.
Virtual 3D Heart Models—Percentages of Physicians Versus Nurses/Trainees Who Indicated Moderate to High Agreement (At Least 7 on 1-10 Likert Scale).a
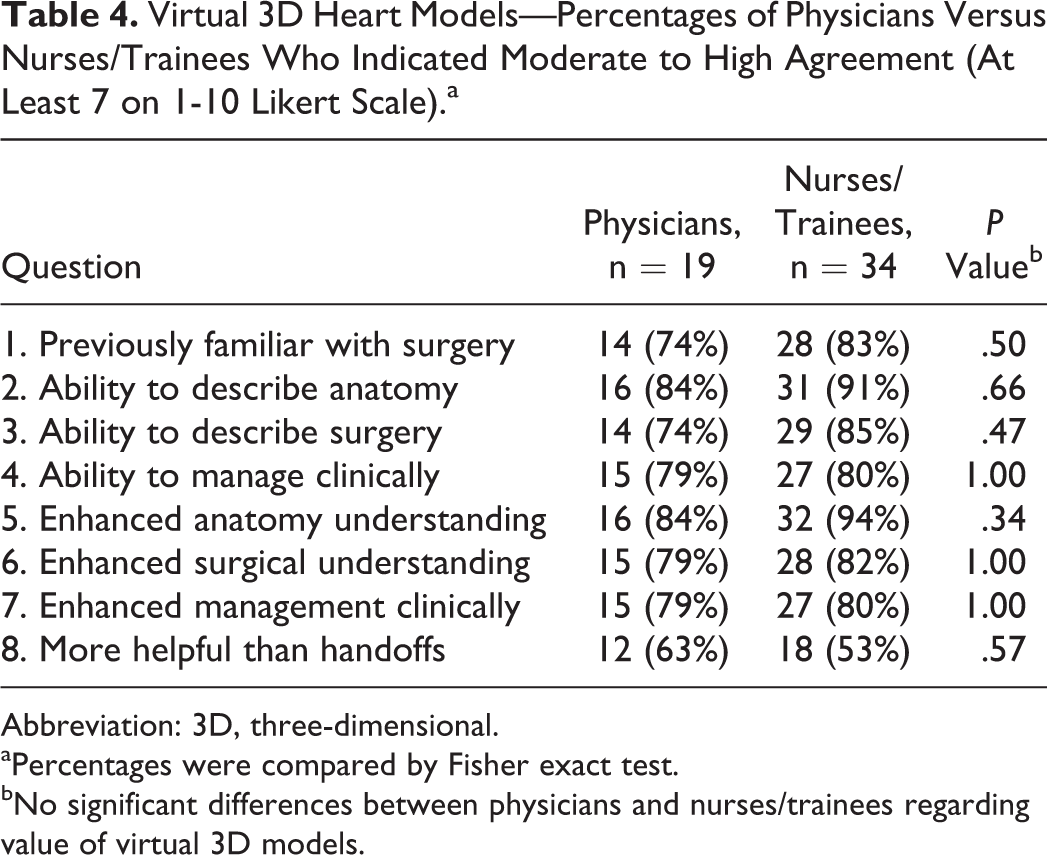
Abbreviation: 3D, three-dimensional.
aPercentages were compared by Fisher exact test.
bNo significant differences between physicians and nurses/trainees regarding value of virtual 3D models.
A higher percentage of the providers in the printed group were confronted with highly complex cases compared to the digital group (34% vs 15%, P = .02), with the average STS-EACTS score of 1.4 versus 0.76 for printed versus virtual 3D models, respectively. However, in controlling for this imbalance, the results remained essentially unchanged regarding questions 6, 7, and 8. Applying multivariable logistic regression controlling for both provider familiarity with the surgery and case complexity, the providers in the printed 3D heart model group indicated significantly higher Likert scores (7 points or above) with respect to questions 6 to 8: question 6: odds ratio = 9.6, 95% confidence interval (CI): 2.2 to 42.3, P = .003, question 7: odds ratio = 13.1, 95% CI: 2.7 to 62.3, P < .001, question 8: odds ratio = 5.5, 95% CI: 2.2 to 14.3, P < .001.
Cost/Resource Analysis
An important consideration in the current analysis of the impact of printed and virtual heart models is cost. Both types of models are derived from 3D cardiac imaging, which requires operator time and specialized software to create a 3D digital heart representation. From the point of creation of the 3D digital heart representation, it can then be uploaded into digital display software as a virtual 3D model, or it can be printed out and displayed as a printed 3D model, demonstrated in Figure 3. The costs up to the decision point of display choice (ie, virtual vs printed model) are identical and therefore not included. The average cost of the virtual 3D model display includes a dedicated tablet ($1,300) and display software, which ranges from shareware ($0) to in-house display software developed specifically for this study (US$3,500). This is a onetime cost for the tablet and software license, which is divided over the life of the tablet. The total cost of production of the ten printed heart models ranged from $3,200 (for in-house printing) to quotes ranging $1,515 to $11,192, depending on outsourcing vendor and type of material. For purposes of this study of 20 cases, the virtual 3D heart model cost ranges from $1,300 to $4,800 (an initial, up-front cost that is not recurring), and the printed 3D heart model cost ranges from $3,200 to $11,192 with an average recurring cost of $260 to $560 per case. Extrapolated to 100 cases, virtual 3D cost would range from $1,300 to $3,500 and printed 3D cost would range from $16,000 to $55,960. There are additional costs to the “just-in-time” simulation with the printed 3D model, as there is no reasonable option for asynchronous, independent “just-in-time” learning with the printed model. Instead, use of a printed 3D model in a “just-in-time” simulation session requires a synchronous group dynamic guided by a CICU attending. This potentially adds hundreds of dollars into the cost model, but varies widely by institution so was not included here.

Process for creation of both 3D virtual and 3D printed models; both models begin with a standardized process using 3D cardiac imaging as a roadmap for creation of a 3D heart reconstruction as a digital file. From there, a decision is made to further render the file to display as a 3D virtual model (bottom left) or as a 3D printed model (bottom right). Cost differential between the two methods was approximately $5,000 to $10,000 for the 20 cases described in this publication. 3D indicates three-dimensional.
Comment
This article presents a first experience with incorporating bedside virtual 3D heart models into a patient-specific, “just-in-time” training program for CICU providers that are accepting patients following congenital heart surgery. Initial results are promising and show that, regardless of provider type, provider familiarity, and case complexity, 3D digital heart models can enhance provider care of patients in the CICU by improving confidence and quality of handoffs when compared to standard verbal review of clinical data. Exploring high-fidelity 3D digital surface models created from MR, CT, and 3D echocardiography images interactively on a tablet device can be an effective tool for providers/patients to intuitively manipulate both a 3D digital model to explore a detailed digital representation of the heart.
Postprocedural, “just-in-time” simulation sessions are an effective way to familiarize bedside CICU providers with uncommon clinical scenarios that can complicate postoperative care of patients with CHD. Doing so with a high-fidelity visual aid could help align the mental models of the team caring for the patient by creating a shared understanding of a patient’s exact cardiac disease with positive results previously published through work done at our institution with printed 3D models. 7 When virtual 3D models are used in the place of printed 3D models, participants are positive about the impact of both types of models, although they were more enthusiastic regarding the printed model and its ability to enhance care and handoffs. However, when a cost analysis is performed, there are significant cost savings when a virtual 3D heart program is established, without significant decreases in satisfaction or overall perception of quality and impact. The result is that virtual 3D heart models offer better value.
In addition, the 3D heart model educational intervention was accompanied by a CICU faculty-led simulation session using a high-fidelity simulation scenario by our institution’s simulation program which was not calculated into cost. In order to access the educational opportunity of the prior 3D printed model, CICU providers had to be available during a specific time for a guided, group “just-in-time” simulation. The digital 3D models allowed for asynchronous “just in time” learning at a time most convenient for the CICU team and allows for continued use of the digital model throughout the patient’s hospital stay including handoffs during changes in shift and care teams (CICU and cardiology inpatient floor). The apparent preference of the care team for the printed heart model intervention in enhancing handoff and postoperative care may have been impacted by experiencing tactile learning by holding the heart in one’s hands in the printed model group, as well as the asynchronous “just-in-time” session that did not involve the presence of a faculty member. Further studies are warranted to investigate this.
Although this article discusses the implementation of a virtual 3D heart model simulation in the immediate postoperative period, these models have the potential to improve surgical planning of CHDs similar to printed 3D heart models. The 3D printed heart models have established clinical value in CHD management, 15,16 and these models can easily be extended to any clinical process that could benefit from a portable visual communication framework for patient imaging data. Initial work looking at use of models with families is promising. 17 Extending use of the model to the clinical care team in the ICU and beyond is a next logical step.
Limitations of this work include the disparity in self-reported familiarity with congenital heart surgery postoperative care between the printed and virtual groups, as well as disparity between the complexity of cases between these two groups, although this was controlled for statistically. Ideally, a printed versus virtual study should occur simultaneously to fully understand impact and provider preference; however, these studies occurred in series as bedside virtual 3D display technology became available, possibly contributing to the discrepancy in previous familiarity between the two groups. Studying heart models of any variety in the larger workflow, from decision-making to procedural planning, family consultation, and postoperative care provision, would be the ideal way to quantify their impact. Additional limitations include the low number of trainees enrolled in this clinical care study, which limited our ability to draw conclusions about how heart models perform in this group. Future work will be dedicated to this study.
In conclusion, virtual 3D heart models displayed at the patient bedside using a novel digital display increase CICU provider confidence in their care delivery and their ability to handoff care, regardless of provider type (nurse or physician). While 3D printed heart models received more enthusiastic scores, a cost analysis of printed versus virtual heart models demonstrates excellent value in virtual 3D heart models in the CICU care setting.
Footnotes
Acknowledgements
The authors wish to thank the Children’s National Medical Center Board of Visitors, who supported this work.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Matt Irwin is a full-time employee of Indicated, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in full by the Children’s National Medical Center Board of Visitors.