
Abstract
Background:
Arterial switch operation (ASO) is a relatively safe operation nowadays. We hypothesize that intraoperative revision for coronary malperfusion still plays an important role during ASO in the current era.
Methods:
From January 2005 to May 2016, 244 patients underwent ASO. Medical records were reviewed and the details of intraoperative revision were described. Morbidity and mortality were compared in patients with/without intraoperative revision. Factors related to the need for intraoperative revision were analyzed.
Results:
Seventeen (7%) patients needed intraoperative revision. As a technique for intraoperative revision, revision of a coronary button was performed in eight patients and revision of the main pulmonary artery anastomosis to relieve compression on the coronary artery was performed in five patients. Factors related to intraoperative revision were body weight at surgery (P = .051), eccentric position of the coronary ostium (P = .01), single coronary artery system (P = .03), and intramural coronary artery (P = .003). The commonest coronary artery origin and branching pattern was not protective against the need for intraoperative revision (P = .43). Discharge mortality was 2% overall: 2 of 17 with intraoperative revision versus 3 of 238 without it (P = .04). Patients who underwent intraoperative revision had longer postoperative hospitalization (P = .003).
Conclusion:
The need for intraoperative revision was related to eccentric coronary ostium, single coronary artery, and intramural coronary artery. Although the need for intraoperative revision correlated with higher mortality and morbidity, prompt intraoperative revision also likely contributed to our good results after ASO.
Introduction
Early outcomes for the arterial switch operation (ASO) have dramatically improved since it was first introduced by Jatene et al in 1975. 1 The current expectation according to the Society of Thoracic Surgeons Congenital Heart Surgery Database 2 is that operative mortality is 2.7% for ASO and 5.3% for ASO plus ventricular septal defect (VSD). These numbers should be lower in high-volume centers, including our own. 3
One major factor that should contribute to the excellent outcome in the current era is the establishment of standard techniques for ASO by pioneers and mentorship utilizing the standard techniques. 4,5 However, diversity exists with respect to the standard technique of ASO among surgeons and ASO is still technically demanding and challenging for young surgeons. Surgeons have also added modifications to their standard technique to cope with variations in morphology, and many modifications have been proposed. Some modifications such as the trapdoor technique 6 have gained popularity and are considered part of the standard technique by some surgeons. 4,5
After the ASO, early mortality is almost always due to coronary malperfusion related to coronary artery transfer, 7 and we occasionally have had to perform intraoperative revision for coronary transfer during ASO if there were signs of myocardial ischemia. There have been a few case reports on intraoperative revision during ASO. 8 –10 Mussa et al 4 described that out of 449 patients who underwent ASO (excluding patients with a complex anatomy), 10 patients required intraoperative revision to refashion coronary buttons, although the revision details were not documented. Thus, limited published data exist on intraoperative revision during ASO. We hypothesize that intraoperative revision for coronary malperfusion still plays an important role during ASO in the current era. The objectives of this study were three-fold: (1) to describe the details of intraoperative revision performed in our patients, (2) to analyze the risk factors related to the need for intraoperative revision, and (3) to compare morbidity and mortality in patients with/without intraoperative revision.
Patients and Methods
This study was approved by the institutional review board of Columbia University (Protocol Number: AAAR0277) and the need for informed consent for the study was waived. The medical records were reviewed retrospectively.
Patients
Between January 2005 and May 2016, 244 patients underwent ASO, including all patients with a complex anatomy and 4 who underwent palliative ASO. Patients who underwent the double-switch procedure were excluded. Patient characteristics are shown in Table 1. Preoperative comorbidity was defined as having sepsis; gastrointestinal diseases; pulmonary diseases such as neonatal respiratory distress syndrome, pneumonia, pneumothorax, or congenital diaphragmatic hernia; or neurologic deficit such as infarct or hemorrhage. It was our routine to check brain magnetic resonance imaging after balloon atrial septostomy. A previous palliative surgery had been performed in seven patients: two patients underwent pulmonary artery banding due to a late referral, three patients underwent palliation due to extreme prematurity or septic shock, and the other two patients underwent a scheduled palliation for morphological reasons (modified Blalock-Taussig shunt in a patient with transposition of the great arteries [TGA]/VSD/left ventricular outflow tract obstruction and aortic arch repair/pulmonary artery banding in a patient with double outlet right ventricle/noncommitted VSD/crisscross heart). Five attending surgeons operated during this period who were classified as follows: level A: >20 years of experience as an attending surgeon (n = 1), level B: 10 to 20 years of experience (n = 3), and level C: <10 years of experience (n = 1).
Patient Characteristics.
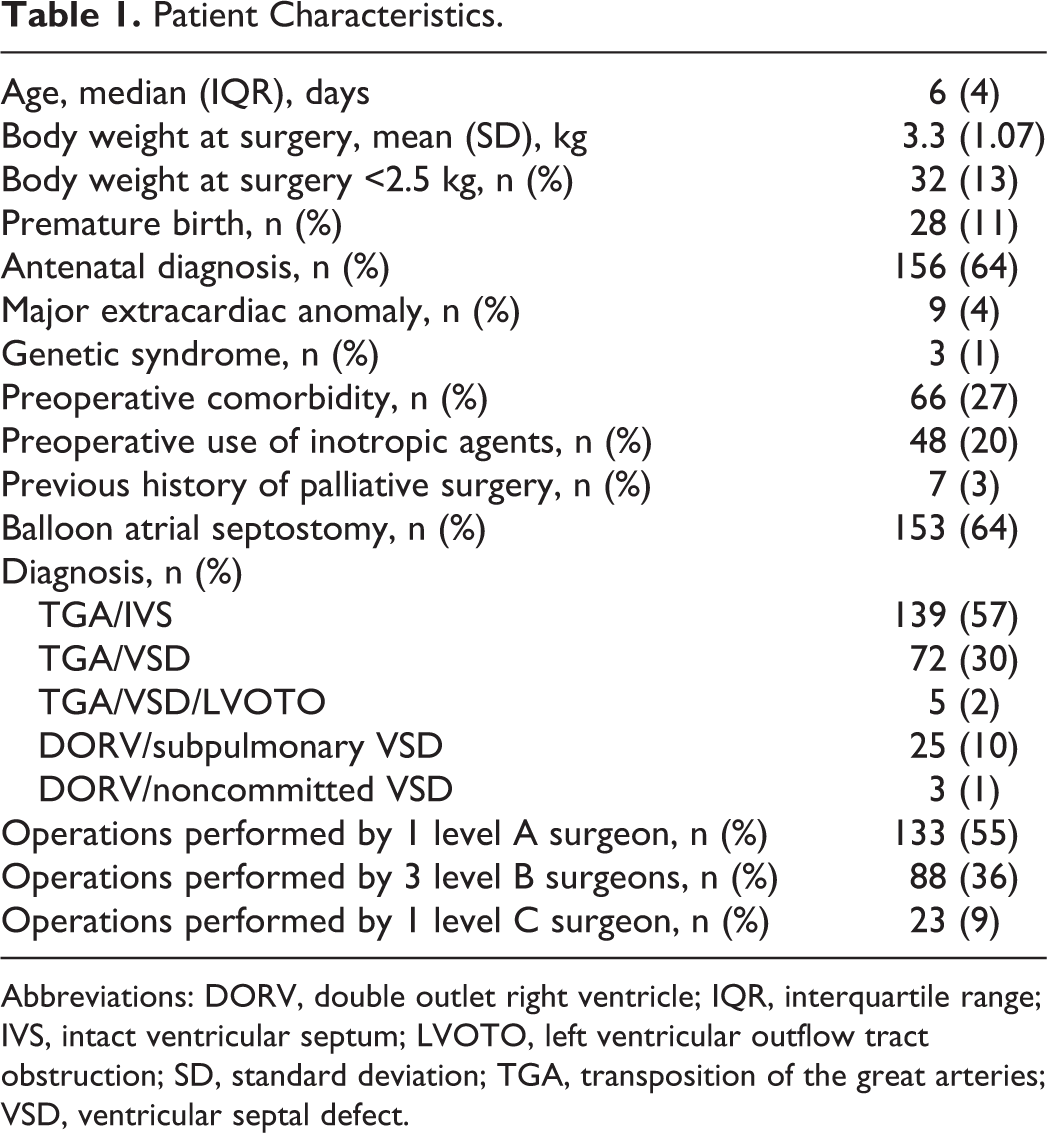
Abbreviations: DORV, double outlet right ventricle; IQR, interquartile range; IVS, intact ventricular septum; LVOTO, left ventricular outflow tract obstruction; SD, standard deviation; TGA, transposition of the great arteries; VSD, ventricular septal defect.
Details of coronary artery anatomy were based on surgeons’ observations during ASO (Table 2). The coronary artery origin and branching pattern was described using the Leiden convention. 11 One patient with {1 Cx 2 LR} and a crisscross heart had an intramural course for both coronary arteries. Single right coronary artery (RCA) {2 LCxR} is the one with the left coronary artery (LCA) behind the pulmonary artery; single RCA {2 RLCx} is the one with the LCA anterior to the aorta. Major malalignment of the commissures was defined as the commissure between the two facing sinuses of the aorta pointing toward the middle of the facing pulmonary sinus. Of the 12 patients with a bicuspid pulmonary valve, 5 had major commissure malalignment. The orifice of the coronary artery located in the middle of the aortic sinus just below the sinotubular junction was considered normal, and other positions such as the one very close to the commissure or above the commissure were considered eccentric. If the main pulmonary artery was approximately twice the size of the aorta, this was regarded as a significant aortopulmonary diameter mismatch (larger pulmonary artery).
Details of the Anatomy.
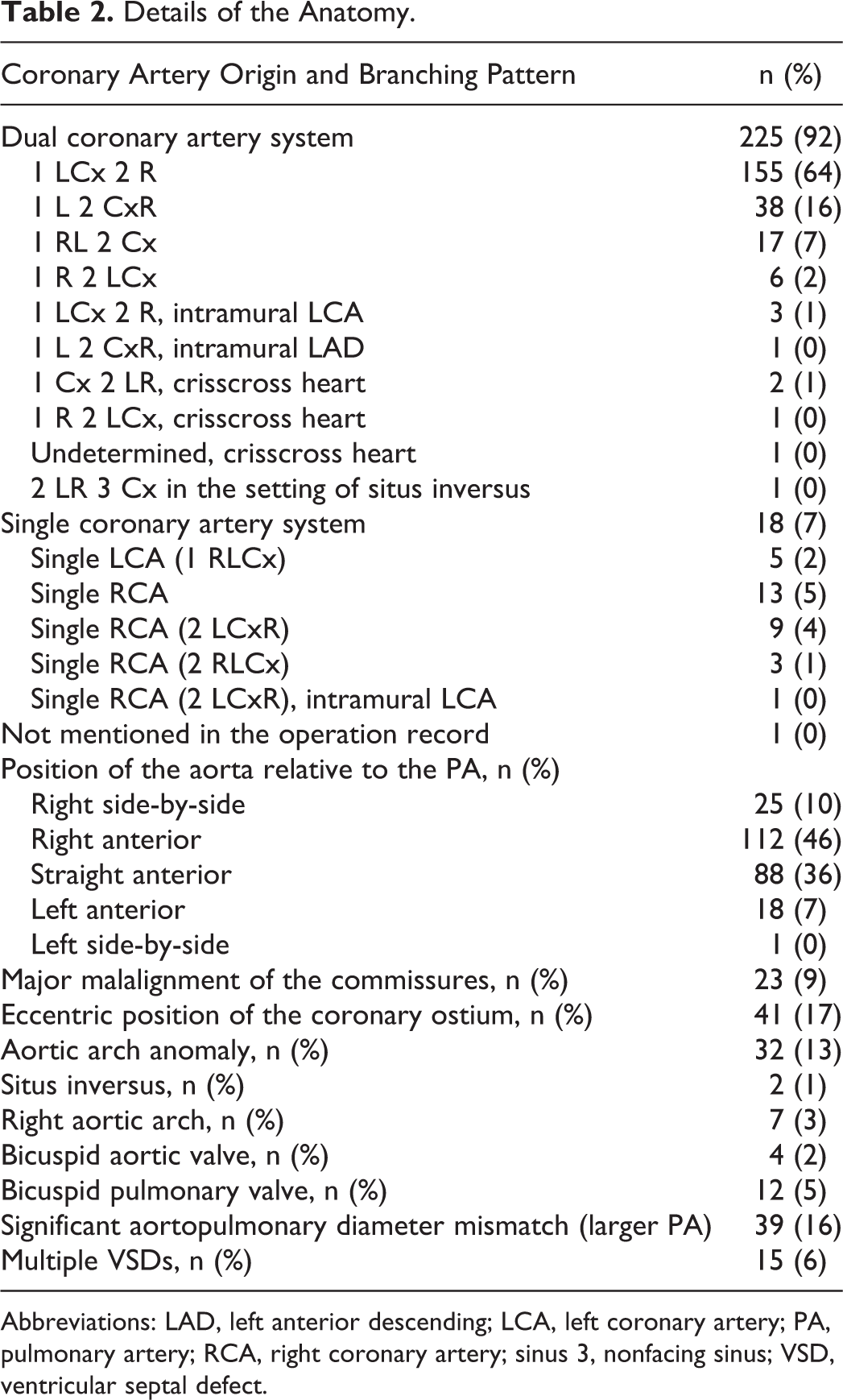
Abbreviations: LAD, left anterior descending; LCA, left coronary artery; PA, pulmonary artery; RCA, right coronary artery; sinus 3, nonfacing sinus; VSD, ventricular septal defect.
Arterial Switch Operation Technique
The standard technique for the commonest coronary artery pattern {1 LCx 2 R} is described herein. Cardiopulmonary bypass was instituted and the patients were cooled down to varying degrees depending on the complexity of the case. The coronary arteries were excised with an incision starting from the aortic transection site except that the level A surgeon excised the coronary artery from sinus 2 as a button. After a minimum dissection and mobilization of the coronary arteries, four surgeons except one level B surgeon implanted the coronary arteries to a simple linear incision made at the “appropriate site” in each corresponding sinus below the neoaortic suture line, whereas the level B surgeon used the trapdoor technique. 6 Two out of five surgeons implanted the coronary artery after neoaortic anastomosis. 12 The Lecompte maneuver was performed, and the distal aorta was anastomosed to the neoaorta. The neopulmonary root was repaired with either two patches (two out of five surgeons) or a single pantaloon-shaped patch using autologous pericardium. The distal pulmonary bifurcation was anastomosed to the neopulmonary root during the rewarming phase after unclamping the aorta. Other or additional techniques were applied for coronary transfer in cases with more complex coronary anatomy, such as single coronary artery system and intramural coronary artery. Excluding four patients who underwent palliative ASO, all the VSDs were closed except when the surgeons decided to leave tiny muscular VSDs after significant VSDs were closed in patients with multiple VSDs.
Follow-Up
The last date of documented encounter by our pediatric cardiology service was defined as the last follow-up date. We had quite a number of out-of-state and international patients, which rendered our median follow-up period relatively short (median: 131, interquartile range [IQR]: 1,347.75 days).
Statistical Analysis
Continuous data are expressed as mean with standard deviation or median with IQR, as appropriate. Categorical variables are represented as numbers and percentages. Categorical data were analyzed by Fisher exact test. Between-group comparisons were obtained using the Mann-Whitney U test. The study period was dichotomized into two groups (before 2010 vs after 2010) because our extracorporeal membrane oxygenation (ECMO) program became more active since 2010 when our new section chief was appointed. Statistical analyses were performed with IBM SPSS 16.0 (SPSS Inc, Chicago, Illinois).
Results
Discharge Mortality
Discharge mortality was 2% (n = 5) of the entire series and the details are described in Table 3. Discharge mortality was not different among all five surgeons (P = .23). All of the patients died within 24 hours after the operation. Patients A and B died in the operating room despite intraoperative revision. Autopsy findings in patient B showed ischemic change in the left ventricle (LV). Patient C showed some LV global dysfunction intraoperatively, but intraoperative revision was not performed and the chest was left open. The patient deteriorated thereafter and died on postoperative day 1. Patient D showed a smooth intra- and postoperative course but had a sudden pulmonary hemorrhage that led to cardiac arrest and died on postoperative day 1. Autopsy findings showed diffuse pulmonary congestion with extensive intra-alveolar hemorrhage and early LV myocardial ischemia. Patient E had a smooth intraoperative course, but the patient became bradycardic and hypotensive within 10 minutes of arriving in the intensive care unit and subsequently died. No specific pathology was detected by autopsy to explain this event other than changes consistent with persistent fetal circulation in the lungs.
Discharge Mortality.
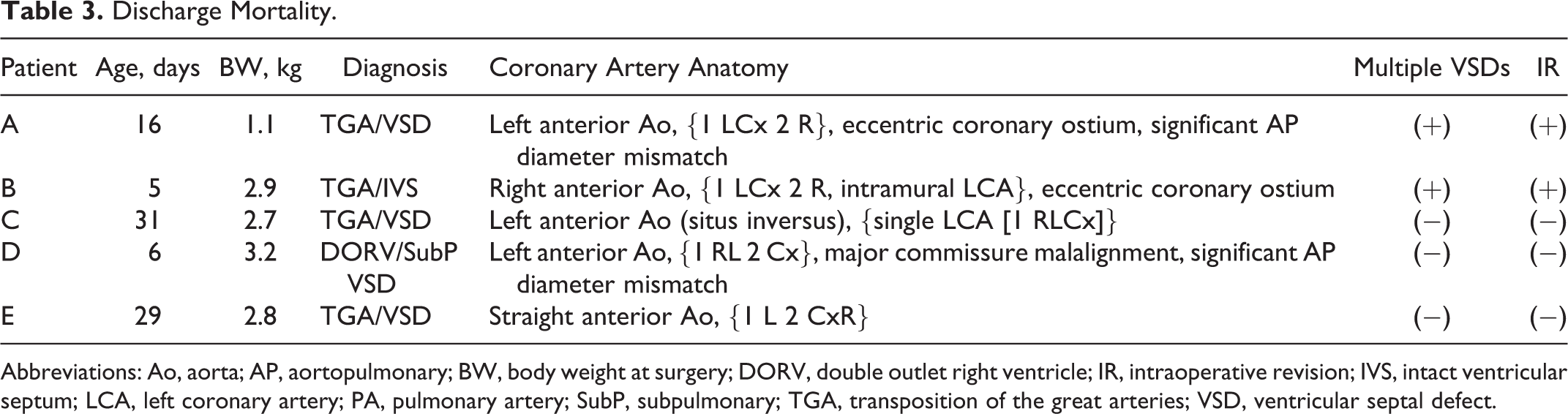
Abbreviations: Ao, aorta; AP, aortopulmonary; BW, body weight at surgery; DORV, double outlet right ventricle; IR, intraoperative revision; IVS, intact ventricular septum; LCA, left coronary artery; PA, pulmonary artery; SubP, subpulmonary; TGA, transposition of the great arteries; VSD, ventricular septal defect.
Complications and Morbidity Outcomes
Three patients required postoperative ECMO and all of them were discharged alive: one patient had a congenital diaphragmatic hernia and was already on ECMO preoperatively, another patient needed support due to a deconditioned LV from delayed surgery for noncardiac comorbidities, and the other patient required support for hemodynamic instability encountered while trying to achieve hemostasis. Besides the patients who died, there were three other patients who needed cardiopulmonary resuscitation: one patient had a cardiac tamponade, another patient had an issue with coronary artery transfer and needed a reoperation after resuscitation, and the other patient had a complicated postoperative course due to atrial tachyarrhythmia and significant chylous effusion after ASO with intraoperative revision. Among the 242 patients (excluding 2 patients who died in the operating room), delayed sternal closure was adopted in 31 (13%) patients and the application of delayed sternal closure had no relationship with the need for aortic arch repair during ASO (P = .58). A total of 15 unplanned operations during the same hospital stay were performed: chest re-exploration for bleeding (n = 5) or hemodynamics instability (n = 1), pulmonary artery plasty (n = 1), coronary artery revision (n = 1), permanent pacemaker insertion (n = 5), and wound revision (n = 2). The postoperative mechanical ventilation time was 2.9 ± 2.2 days, and the postoperative length of hospital stay was 12.0 ± 11.3 days.
Intraoperative Revision
Intraoperative revision for a suspected coronary malperfusion was required in 17 (7%) patients. Details of the intraoperative revision are described in Table 4. Table 5 shows the results of the univariate analysis of risk factors for intraoperative revision. Discharge mortality was 2 (12%) out of the 17 patients versus 3 (1%) out of 227 patients without intraoperative revision (P = .04). Postoperative mechanical ventilation time was longer in patients who underwent intraoperative revision (median: 2, IQR: 1 day vs median: 5, IQR: 3 days, P = .0002). The postoperative length of hospital stay was also longer in patients with intraoperative revision (median: 8.5, IQR: 8 days vs median: 15, IQR: 10 days, P = .003). In 135 patients with TGA/intact ventricular septum without any other concomitant procedures, cardiopulmonary bypass time (median: 130, IQR: 30.25 vs median: 239, IQR: 121, P = .0002) and cross-clamping time (median: 75, IQR: 19 vs median: 99.5, IQR: 77.25, P = .008) were longer in patients who underwent intraoperative revision.
Details of the Intraoperative Revision.
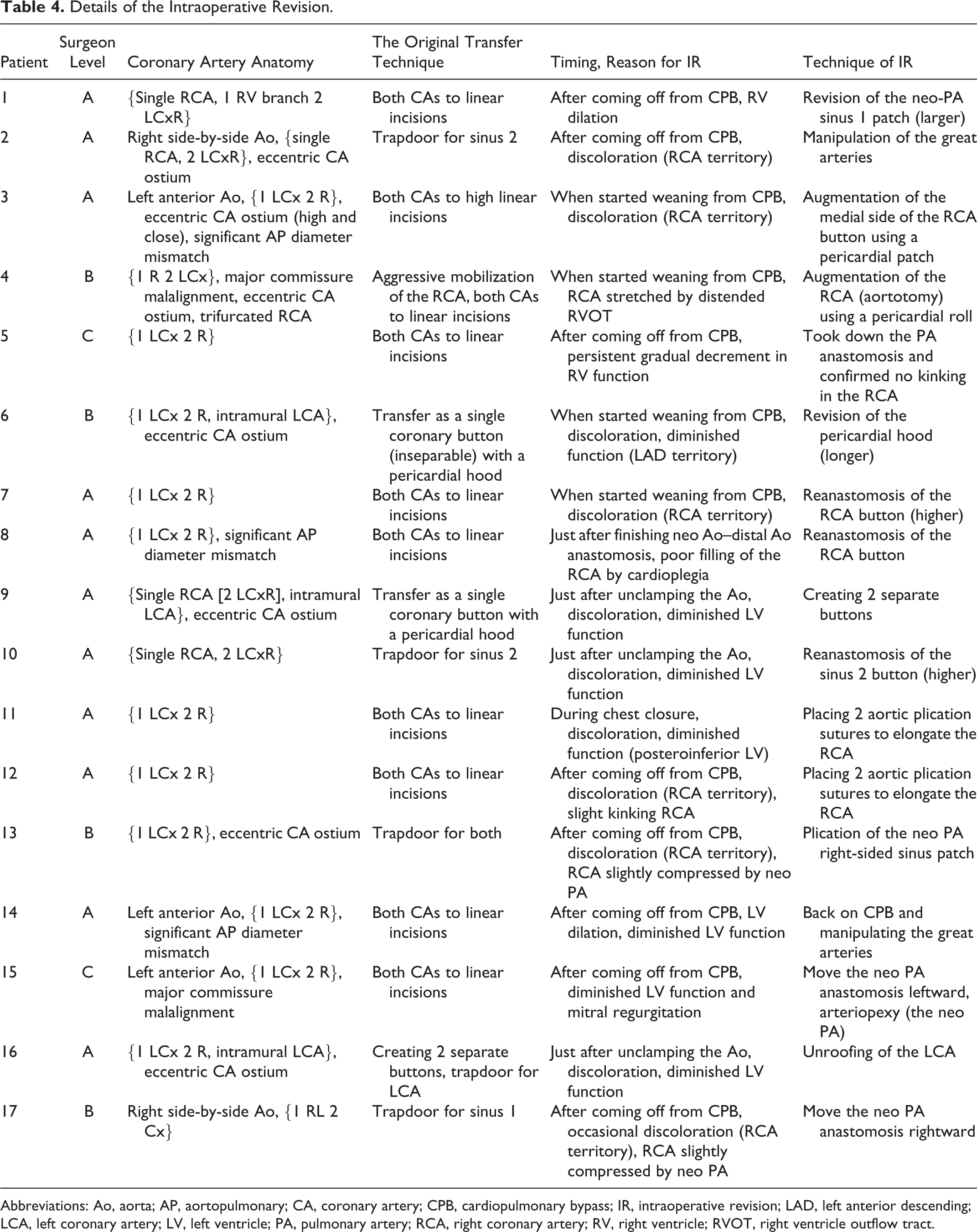
Abbreviations: Ao, aorta; AP, aortopulmonary; CA, coronary artery; CPB, cardiopulmonary bypass; IR, intraoperative revision; LAD, left anterior descending; LCA, left coronary artery; LV, left ventricle; PA, pulmonary artery; RCA, right coronary artery; RV, right ventricle; RVOT, right ventricle outflow tract.
Univariate Analysis of Risk Factors for Intraoperative Revision.
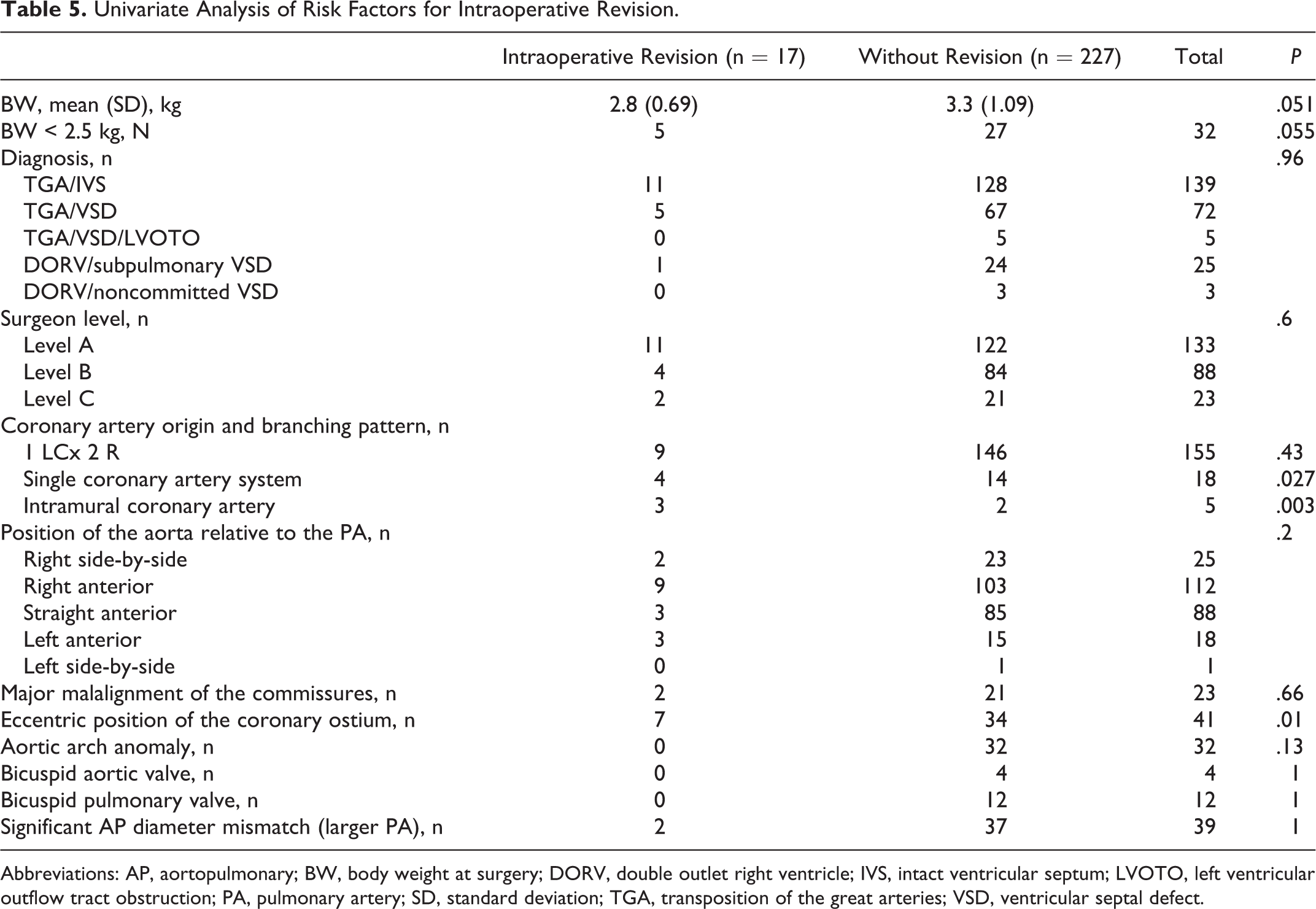
Abbreviations: AP, aortopulmonary; BW, body weight at surgery; DORV, double outlet right ventricle; IVS, intact ventricular septum; LVOTO, left ventricular outflow tract obstruction; PA, pulmonary artery; SD, standard deviation; TGA, transposition of the great arteries; VSD, ventricular septal defect.
Comparison Between Before 2010 and After 2010
All the three cases that required postoperative ECMO were operated on after 2010 and none of them had signs of coronary malperfusion and did not require intraoperative revision. The need for intraoperative revision was equivalent between patients operated on before 2010 and after 2010 (9 out of 128 patients vs 8 out of 116 patients, P = .97), whereas discharge mortality was higher in patients operated before 2010 compared with patients operated on after 2010 (5 out of 128 patients vs 0 out of 116 patients, P = .06).
Short-Term Follow-Up
Neither postdischarge death nor biventricular dysfunction was observed at short-term follow-up, and no patients required a heart transplant. One patient who did not need intraoperative revision during ASO had a coronary event and underwent LCA plasty eight years after ASO. All the patients who needed intraoperative revision and who survived ASO (n = 15) were doing well with reinterventions only to address pulmonary artery stenosis (four reoperations and two catheter interventions) during follow-up (median: 590, IQR: 1,980 days).
Comment
The first learning curve for young surgeons is mastering a standard technique for the common anatomic pattern, namely, {1 LCx 2 R}, anterior rightward aorta, well-aligned commissures, and normal position of the coronary ostium. 13,14 The second learning curve 13,14 is how to modify the repair depending on the anatomical features. Experiences of pioneers have enabled us to describe these modification patterns to some extent. For example, patients with intramural coronary arteries can be managed successfully using Mee’s method. 15,16 When we address patients with {1 RL 2 Cx} or {1 R 2 LCx} (double-looping coronaries by Planché classification 17 ), we know that stretching of the sinus 1 coronary artery and kinking of the sinus 2 coronary artery is a problem that can be managed by an extensive dissection of the sinus 1 coronary artery and transferring the sinus 2 coronary artery at a higher position than usual. Further, if a Lecompte maneuver is performed in the setting of a more rightward aorta, mobilization of the main pulmonary artery anastomosis rightward might be necessary. 13 Understanding these already established modifications is important and helpful even when performing intraoperative revision, such as in our patient 17 (Table 4).
The third learning curve should be for the decision of intraoperative revision and techniques used for such a revision. Out of our five patients with discharge mortality, three patients did not undergo intraoperative revision and died within 24 hours after the operation. There might be some signs of coronary malperfusion during the three cases that seemed to have a “smooth” intraoperative course and intraoperative revision should likely have been done in these cases. There has been no discharge mortality since 2010, whereas the need for intraoperative revision was equivalent between patients operated on before 2010 and after 2010. Postoperative ECMO for cardiac failure due to coronary malperfusion has never been applied even after 2010 when our ECMO program got more active. These observations suggest that our surgeons have been improving in terms of the decision-making and techniques used for intraoperative revision over the course of the study period, which likely contributed to no discharge mortality since 2010.
The risk factors related to intraoperative revision were body weight, eccentric position of the coronary ostium, single coronary artery system, and intramural coronary artery (Table 5). Interestingly, the commonest coronary artery origin and branching pattern {1 LCx 2 R} was not protective against the need for intraoperative revision, and six out of the nine patients with {1 LCx 2 R} who needed intraoperative revision were operated on by the most experienced surgeon (level A). The need for intraoperative revision was equivalent among the surgeons. These findings indicate that identification of the “appropriate site” for coronary transfer is sometimes difficult regardless of the coronary artery anatomy, surgeon’s experience, and techniques applied for ASO, which resulted in 7% of our patients undergoing intraoperative revision. Now that operative mortality for ASO is much lower than 7%, the need for intraoperative revision might be the best “near miss” event 18 to analyze ASO in the current era.
As described in Table 4, failure of separation from cardiopulmonary bypass was rather uncommon reason for intraoperative revision in our patients and surgeons have to search for any signs of coronary malperfusion step by step at each decision point during ASO: (1) when the aorta is unclamped by checking filling of the coronary arteries and checking the color of the myocardium, (2) when weaning from cardiopulmonary bypass is started and volume shift occurs, (3) just after separation from cardiopulmonary bypass, and (4) observe for a while even after successful separation from cardiopulmonary bypass to confirm that there is no fluctuation in ventricular function and coloration or electrocardiogram findings. Although intraoperative echocardiography definitely plays an important role in decision-making, it is surgeon’s intraoperative observation and judgment that trigger intraoperative revision.
The decision of intraoperative revision and techniques used for such a revision were very variable and not stereotypical. We believe that intraoperative revision and decision-making need advanced surgical skills and experience that contributes to an excellent result after ASO in the current era. Although the need for intraoperative revision was related to higher discharge mortality and longer postoperative mechanical ventilation time and hospital stay, at least during short-term follow-up, all of the patients who needed intraoperative revision and who survived ASO were doing well.
Study Limitations
The limitations of this study were its retrospective nature. All data were derived from a single institution. Our cohort consisted of patients with heterogeneous morphological backgrounds. There were five surgeons during the study period, and the ASO technique was different among them. The definition of eccentric position of the coronary ostium was based on surgeons’ subjective observations during ASO. Our follow-up after discharge was short and incomplete.
Conclusion
Intraoperative revision was necessary in 7% of our patients during ASO in the current era, and highly advanced surgical skills and experience were necessary for decision-making and a successful revision. Although the need for intraoperative revision was related to higher mortality and morbidity, it likely also contributed to our excellent results after ASO.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.