
Abstract
Adequate caloric intake plays a vital role in the course of illness and the recovery of critically ill patients. Nutritional status and nutrient delivery during critical illness have been linked to clinical outcomes such as mortality, incidence of infection, and length of stay. However, feeding practices with critically ill pediatric patients after cardiac surgery are variable. The Pediatric Cardiac Intensive Care Society sought to provide an expert review on provision of nutrition to pediatric cardiac intensive care patients, including caloric requirements, practical considerations for providing nutrition, safety of enteral nutrition in controversial populations, feeding considerations with chylothorax, and the benefits of feeding beyond nutrition. This article addresses these areas of concern and controversy.
Introduction
Adequate caloric intake plays a vital role in the course of illness and the recovery of critically ill patients. Nutritional status and nutrient delivery during critical illness have been linked to mortality and other clinical outcomes such as poor growth, increased incidence of infection, poor wound healing, prolonged ventilation, increased length of stay, and worse neurodevelopmental outcomes. 1 –10 Early enteral nutrition (EN) has been demonstrated to decrease morbidity and length of stay in critically ill populations. 11,12 However, feeding practices with critically ill pediatric patients after cardiac surgery are variable. The Pediatric Cardiac Intensive Care Society sought to provide an expert review on provision of nutrition to pediatric cardiac intensive care patients, and this article addresses these areas of concern and controversy.
Caloric Needs of Cardiac Intensive Care Unit (CICU) Patients
Malnutrition is reported in as many as 50% of hospitalized patients and 20% of those who are critically ill. 4,13 –16 Specifically, infants undergoing congenital heart surgery have a high rate of growth failure in the perioperative period, especially those undergoing staged single ventricle palliation. 17 The metabolic response to critical illness is unpredictable and energy needs are heterogeneous as patients recover from surgery. Failure to accurately determine energy requirements may result in underfeeding or overfeeding; thus, precise assessments of the patient’s energy expenditure are integral to optimal provision of nutrition.
During critical illness, malnutrition can be associated with increased or decreased metabolism and catabolism partnered with reduced nutrient delivery. Generally, there is a net increase in muscle breakdown leading to large amounts of free amino acids in the blood. 18 These are rapidly consumed by generation of acute inflammatory proteins and used for tissue repair. It is extremely important to provide optimal protein while in this catabolic response to slow the rate of net protein loss. 18 In addition, increased fatty acid oxidation leads to ketone production and increased carbohydrate turnover via gluconeogenesis leading to hyperglycemia.
Postoperative caloric needs are often higher than expected due to elevated resting energy expenditure (REE) but are variable and not easily predictable in children. The catabolic stress response varies significantly from one patient to another. Factors that affect this response are the duration and severity of injury or illness, complications experienced during critical illness, and the medical therapy and respiratory support requirements.
13,18
In the immediate postoperative period, the aim is to provide basal energy expenditure using the World Health Organization tables for the first three to five days, and then escalate, giving consideration to stress and injury factors.
13
Caloric intake as high as 150 to 170 kcal/kg/d may be necessary for some children to gain weight,
13,17,19
–21
and protein provision 1.5 to 2 times the recommended dietary allowance may be warranted. Factors such as fever, recent surgery, neurologic storming, and trauma all potentially increase metabolism, whereas paralysis, sedation, hypotonia, and some genetic dispositions may decrease metabolism.
13,17,20
When determining energy needs of the intensive care unit (ICU) patient, indirect calorimetry is the preferred method.
13,14,17,18
Indirect calorimetry calculates heat production by measuring the patient’s pulmonary gas exchange. It determines oxygen consumption, carbon dioxide production, and a respiratory quotient (RQ) along with REE. The following equations are utilized.
4,22


It is recommended to use the RQ to validate the test results. The RQ helps gauge whether the test is within the normal biological range (0.67-1.3). There are specific patient eligibility criteria to use indirect calorimetry in the ICU, such as those who are underweight (BMI <5th percentile for age) or overweight (>85th percentile for age), children with >10% weight gain or loss during ICU stay, failure to consistently meet prescribed calorie goals, or failure to wean from respiratory support. 14,15,23 However, there may be potential barriers to implementing the test such as cost, time to reach steady state, and limited manpower or resources available. If indirect calorimetry is not feasible, using standard REE equations (World Health Organization, Harris-benedict, and Schofield equations) is recommended, with additions for stress and activity factors. These predictive equations are less reliable because they do not account for changes in body mass, sedation, paralysis, or stress factors, but they are used frequently due to the limitations of implementing calorimetry studies. There is a higher risk of overfeeding and underfeeding with predictive equations so energy expenditure should be assessed often throughout the course of illness. 18
A standard prescription of feeding volume and caloric density cannot be made to ensure optimum nutrition in all patient subsets. Table 1 provides general recommendations for providing nutrition to a neonate. However, a dedicated nutrition team is helpful for recognizing heterogeneous nutrition needs, identifying patients at risk for altered metabolism, developing tailored nutrition plans, facilitating protocol advances, managing troublesome emesis, reflux, and/or formula intolerance, and ensuring patients are meeting nutrition goals. 24,25
Recommended Provision of Nutrients for a Neonate.
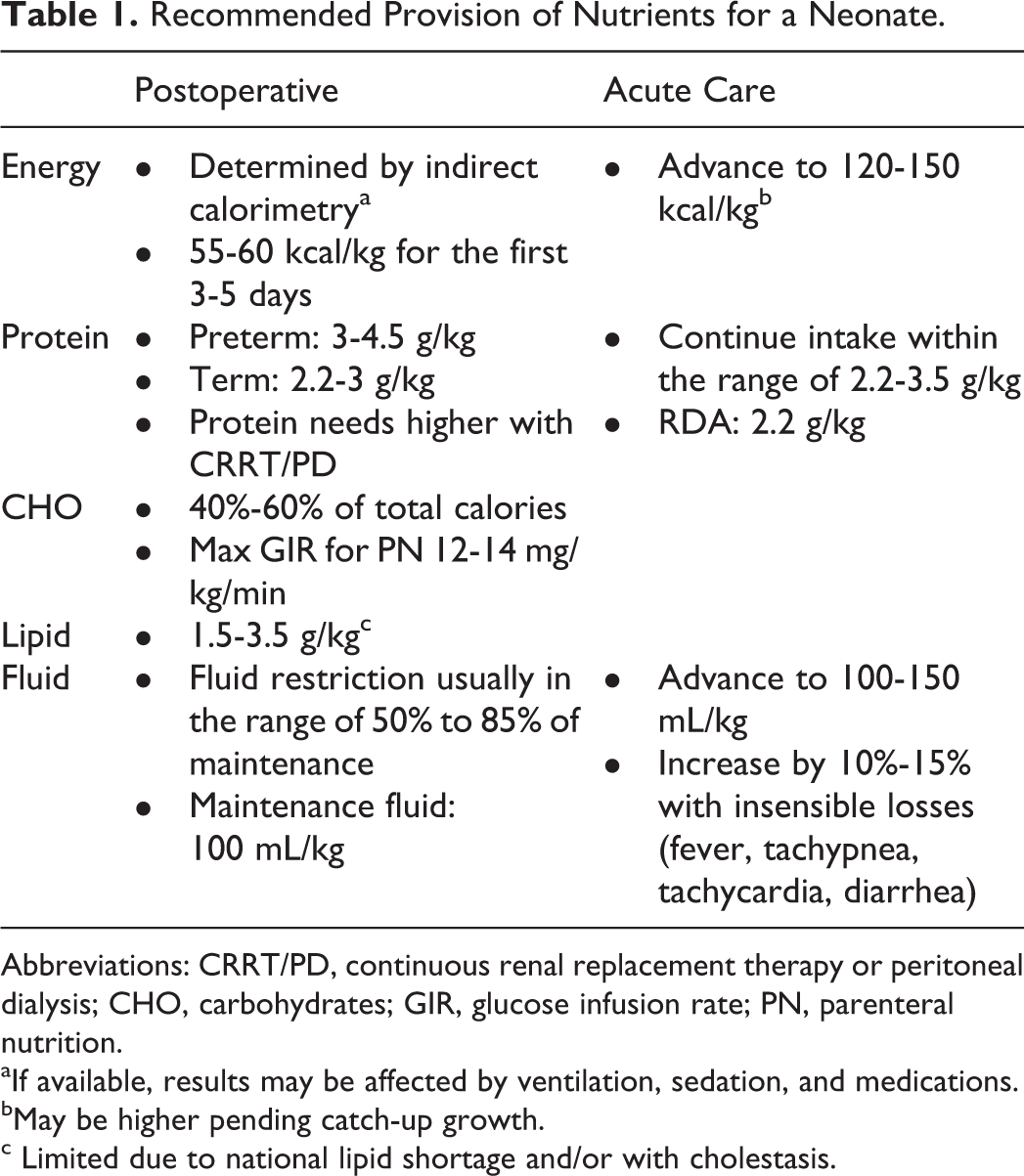
Abbreviations: CRRT/PD, continuous renal replacement therapy or peritoneal dialysis; CHO, carbohydrates; GIR, glucose infusion rate; PN, parenteral nutrition.
aIf available, results may be affected by ventilation, sedation, and medications.
bMay be higher pending catch-up growth.
c Limited due to national lipid shortage and/or with cholestasis.
Practical Concerns Feeding the CICU Patient
The etiology of perioperative growth failure in children undergoing congenital heart surgery is multifactorial and includes genetic syndromes, increased REE, gastrointestinal (GI) abnormalities, fluid restriction, and/or inadequate caloric intake. 17,20,21,26,27 Insufficient caloric intake may be related to perioperative feeding difficulties associated with congestive heart failure, gastroesophageal reflux disease, vocal cord dysfunction, aspiration, uncoordinated suck and swallow, feeding aversion, and/or neurologic injury. 17,20,21,27,28
Optimizing perioperative nutrition is gaining increasing attention as a route to improve overall outcomes after cardiac surgery, especially in neonates and infants. However, no consensus exists regarding optimal feeding strategies or feeding-related management in neonates with CHD. Examination of current evidence suggests that most feeding practices remain center-specific, and given the lack of evidence, there is tremendous variability among patient cohorts, centers, and even individual clinicians regarding almost every aspect of perioperative feeding management. Opportunities exist for multicenter collaborative quality improvement and clinical research for standardization and development of best-practice feeding guidelines.
Despite acceptance that optimizing nutrition is important for good postoperative outcomes, two recent studies highlight that standard practice does not achieve this goal. Toole and colleagues showed only two-thirds of 121 children younger than two years reached their protein and caloric needs by one week after surgery, 26 and Schwalbe-Terilli et al demonstrated that less than half of neonates achieved set caloric goals, resulting in an overall net weight loss at discharge. 10 Feeding and nutrition should not be marginalized as a perioperative outcome that is less important than well-studied clinical outcomes such as duration of ventilation or inotropic score. Protein and caloric goals should be understood by the entire care team and reviewed daily, including weight tracked on a visible growth chart. Many centers have integrated dieticians into CICU care teams to facilitate standard feeding practices that achieve these goals. 24 Perioperative feeding protocols are the best studied aspect of nutritional management and have been shown to facilitate more efficient attainment of nutritional goals, improve growth, decrease GI morbidity, and possibly decrease hospital length of stay and incidence of necrotizing enterocolitis (NEC) in single-center studies. 24,25,28 –30 The optimal, safest protocol is not known and should be the focus of multicenter initiatives.
Preoperative Feeding in Neonates
There is tremendous variability in the proportion of children that are fed preoperatively among centers and clinicians. A study from the Pediatric Cardiac Critical Care Consortium (PC 4 ) reported only about half of 251 neonates were fed preoperatively, with a range of 29% to 79% among centers. 27 A survey from the National Pediatric Cardiology Quality Improvement Collaborative (NPC-QIC) reported 30 of 46 centers feed single ventricle neonates preoperatively. 31 Still to date, there is minimal prospective, controlled evidence to support the safety and/or benefit of preoperative EN in neonatal cardiac surgical patients. Concerns for intestinal ischemia lead many clinicians to avoid preoperative feeds in ductal-dependent systemic circulation. 19 However, recent publications suggest that preoperative feeds may be safe and may improve postoperative feeding tolerance and other clinical outcomes in this high-risk population. 32 –35 One study found that neonates with hypoplastic left heart syndrome (HLHS) that received preoperative trophic feeds had a shorter duration of postoperative mechanical ventilation, less fluid overload, and earlier postoperative feeding tolerance. 36 The analysis contains all of the expected limitations of a single-center, retrospective cohort study but remains important for showing that preoperative feeds might be safe and positively impact clinical outcomes. Further research is necessary to determine the comparative risks and benefits of preoperative feeding in specific patient subgroups, including volume, type, and route of feeds.
Postoperative Feeds
Best practices regarding the timing and type of postoperative EN are not known and again demonstrate significant practice variation. In a multicenter cohort of neonates, median time to initiation of feeds ranged from one to four days postoperatively. 27 Early initiation of feeding and postoperative feeding protocols have been associated with improved outcomes. 24,25,28 –30 However, feeds are often delayed in patients on mechanical ventilation and vasoactive medications, despite growing evidence that early EN in patients requiring these therapies is safe and may improve outcomes. In the pediatric ICU population, patients who receive EN while on vasoactive support do not have increased GI morbidity compared to those not fed, 37 and early EN while mechanically ventilated is associated with decreased mortality in a prospective multicenter cohort. 6 Frequent interruption of feeds prevents attainment of optimal nutrition. Clinical dogma commonly dictates that feeds be stopped often, due to tracheal extubation, procedures, minor GI disturbances, respiratory distress, and other minor clinical deteriorations. Early initiation of feeds via the transpyloric route has been shown to be safe in this population and may help significantly decrease interruption of feeds. 6,38 Transpyloric feeds may even be continued during weaning from the ventilator, during tracheal extubation, and for those on noninvasive ventilation. 39
Total Parenteral Nutrition
The role of total parenteral nutrition (TPN) in the perioperative period is not clear. It is unknown whether the potential nutritional benefit outweighs the morbidity associated with TPN. A recent randomized control trial in critically ill pediatric patients demonstrated that withholding TPN was clinically superior to providing early TPN, including fewer new infections and other improved outcomes, with most benefit seen in neonates. 40 We surmise a protocol that provides a framework for appropriate risk assessment for provision of preoperative feeds, as well as early initiation of protocol-driven postoperative feeds, and avoidance of TPN in children undergoing normal postoperative convalescence warrants further study.
Feeding Tubes
Sixty percent to 80% of neonates are unable to take enough oral feeds to support caloric needs after cardiac surgery and are discharged home with a feeding tube. 27,41 Swallowing dysfunction, vocal cord paresis, aspiration, neurologic injury, and genetic syndromes are common in this population and significantly increase the risk for tube feeding at discharge. Frequency of feeding tube at discharge varies dramatically by center 27 and is likely related to different institutional guidelines for placement, thresholds for discharge with feeding tubes versus continued hospitalization to work on oral feeds, and/or protocols for assessment of vocal cord dysfunction and aspiration. There is no consensus about which type of tube (surgical or temporary) is superior in terms of overall safety and efficacy. Studies show no consistent difference between the two modalities 41 –43 Early identification of children at risk for tube feedings and subsequent early feeding tube placement will likely decrease hospital length of stay. 44 Risk-adjusted comparison of temporary versus surgical tubes is necessary to help determine which type of feeding tube, if any, is superior with regard to safety and/or improved outcomes after neonatal cardiac surgery.
Safety of Enteral Nutrition in the CICU: Controversial Populations
There are several populations in the pediatric CICU in whom controversy and practice variation persist with regard to the safety of providing EN. These populations and their respective perceived feeding risks are summarized in Table 2.
Enteral Nutrition in the CICU: Controversial Populations.
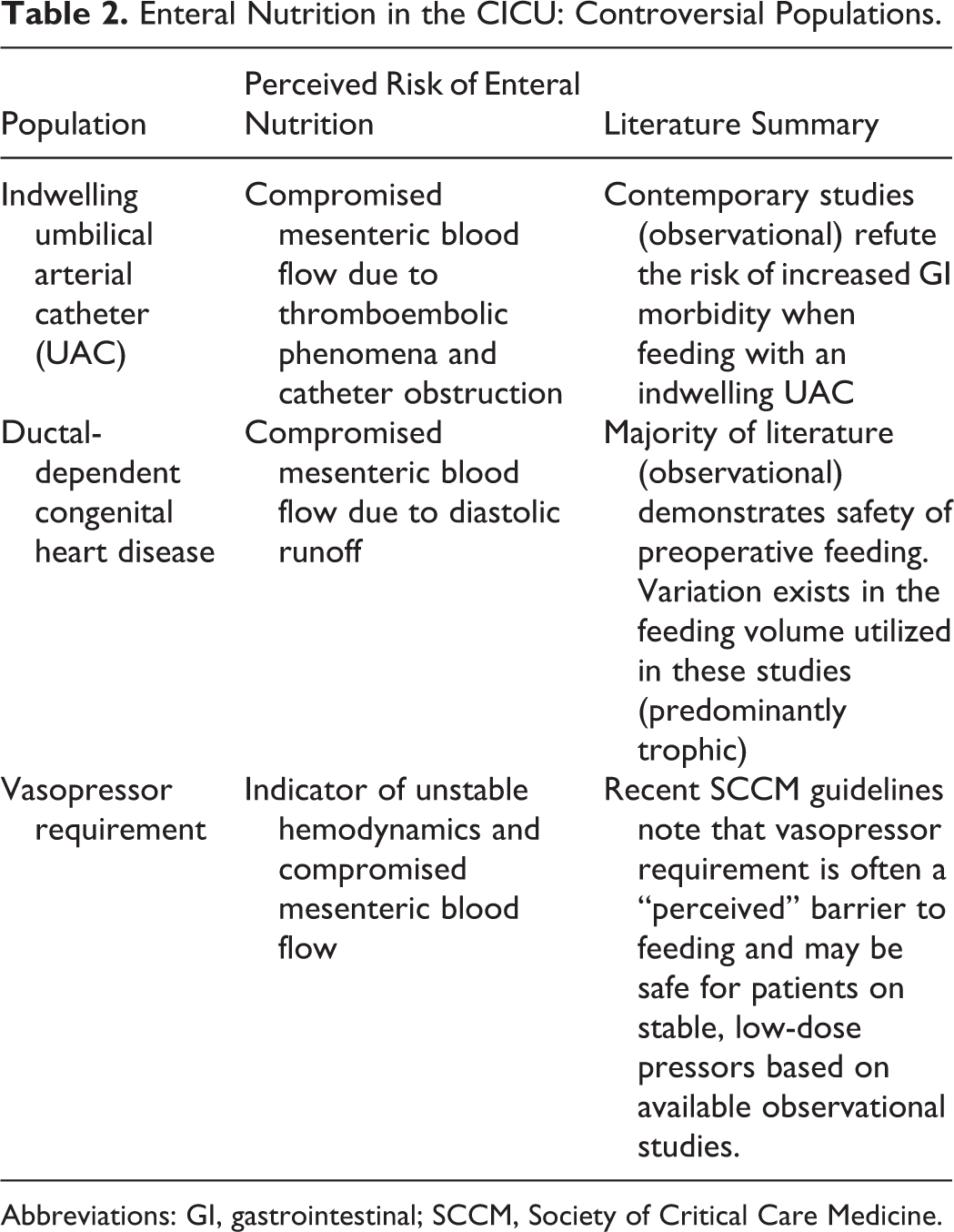
Abbreviations: GI, gastrointestinal; SCCM, Society of Critical Care Medicine.
Indwelling Umbilical Arterial Catheters
Controversy continues to exist regarding the safety of administering EN when an infant has an indwelling umbilical arterial catheter (UAC). Necropsy studies performed in the 1970s found an alarming rate of arterial thromboembolic phenomena in infants with UACs, causing concern that mesenteric blood flow may be compromised in these patients, thereby increasing the risk of necrotizing enterocolitis. 45,46
Recent studies suggest that most providers believe feeding with an UAC present is a safe practice but lack of high-quality data has allowed significant practice variation to persist. 27,47 Davey and colleagues performed a prospective, randomized study evaluating the safety of feeding preterm infants with a “low-lying” UAC and found no difference in the incidence of feeding intolerance or NEC. 48 This study was limited by a small sample size (29 infants) and did not include patients with cyanotic congenital heart disease (CHD). Larger, retrospective studies aimed at evaluating the epidemiology of NEC in CHD have not observed an increased risk due to the presence or duration of an indwelling UAC. 49,50 The impact of these findings is limited by the observational nature of these studies and lack of data regarding enteral feeding practices.
Several attempts have been made to demonstrate the effect an indwelling UAC may have on mesenteric blood flow using Doppler ultrasound techniques. The results of early studies were equivocal and concluded that UACs have the potential to decrease mesenteric blood flow. 51,52 More recent studies found no differences in blood flow velocity or vascular resistance when an UAC was present. 53,54 One study evaluated Doppler flow patterns in infants while feeding and found that an UAC did not alter pre-or postprandial flow in the superior mesenteric artery. 54 Despite the above limitations, the evidence argues against the notion that an indwelling UAC should be a contraindication to enteral feeding when viewed in isolation of other potential risk factors for GI morbidity.
Vasopressor Requirement
Several retrospective studies have reported low rates of GI morbidity when feeding critically ill children on vasopressors. 37,38,55 The recently published Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition guidelines support the use of EN in critically ill children. 14 The guidelines note that vasopressor requirement is often a “perceived” barrier to feeding that may be avoidable based on available observational studies. Of note, the quality of evidence is described as “low” and this recommendation is graded as “weak.” Similar guidelines exist for adult critically ill patients and recommend EN for patients on stable, low doses of vasopressors and who have an adequate perfusion pressure without progressive metabolic acidosis or signs of feeding intolerance. 23 Prospective studies and analyses specific to children with cardiac disease are lacking. Despite limited evidence, it seems reasonable to consider enteral feeds in children requiring vasopressor support while heeding caution during the situations noted above in the adult guidelines when the clinical picture suggests unstable hemodynamics.
Ductal-Dependent CHD
Preoperative feeding of infants requiring prostaglandin infusion for ductal-dependent CHD continues to be a debated topic. The rate of preoperative feeding during the Single Ventricle Reconstruction trial (2005-2008) was 12%. 56 More recent studies have suggested that this rate may be increasing. An analysis utilizing the PC 4 registry found that 42% of neonates with hypoplastic left heart syndrome were fed preoperatively among six participating centers, but there was significant center variation with rates ranging from 29% to 79%. 27 In 2016, survey data from centers participating in the NPC-QIC reported that 65% of the 46 centers allow single ventricle neonates to feed preoperatively. 19
This trend toward higher rates of preoperative feeding is likely the result of studies demonstrating it can be a safe practice. 32,33,35,36 Although these analyses did not find that feeding ductal-dependent neonates poses additional risk of GI morbidity or NEC, there were important limitations. The studies are predominately retrospective or observational in design, subject to selection bias, and often excluded important comorbidities such as prematurity. Zyblewski and colleagues performed a randomized trial comparing neonates that were fed trophic breast milk with a group that remained NPO. Although the study found no difference in rates of feeding intolerance or NEC between the groups, the small sample size was underpowered to detect differences in adverse events. 33
As the field continues to establish the safety and potential advantages of preoperative feeding in ductal-dependent neonates, the more difficult question becomes “when is it not safe to feed?” these tenuous patients. It will be challenging for any study to model the complex risk assessment made by the astute clinician at the bedside that incorporates patient-specific risk factors, careful physical examination, and data from physiologic monitoring.
Chylothorax
Chylothorax is a common complication after pediatric cardiac surgery, associated with rates as high as 9% reported among benchmark operations. 57 The Fontan, Norwood, atrioventricular canal repair, Glenn, and arterial switch procedures are all associated with an incidence higher than 5% in surveillance of national databases. The presence of chylothorax has also been associated with significantly increased cost, hospital resource utilization, and increased ICU and hospital length of stay. 58 –61 The incidence of this complication over the last decade reveals a consistently increasing trend with no singular treatment pathway emerging. An analysis by the PC 4 showed that risk-adjusted postoperative chylothorax rates vary among centers, suggesting that the incidence may be modifiable with a better understanding and mitigation of perioperative risk factors. 62
Definition
Some of the discrepancy in treatment lies in how chylothorax is defined, or more specifically, the definition that triggers a change in management has not been uniformly accepted as evidenced by multiple published algorithms. 63 –68 Chylous effusions are characterized as milky in appearance with a pleural fluid white blood cell count of greater than 1,000 cells/μL, pleural lymphocytes greater than 80%, and if normally fed, a triglyceride level in the pleural fluid of greater than 1.1 mmol/L. Additionally, a pleural fluid triglyceride level to serum triglyceride level ratio of greater than 1 is also characteristic of a chylothorax. 69 It remains unclear how many of the above criteria must be met before a change in management is sought and what quantity of drainage merits initiation of a treatment algorithm.
Management
Treatment algorithms have been largely limited to single-institution experience with significant variation. Figure 1 represents a summary of the various protocols in the published literature and from an informal survey of practice patterns in over 50 international CICUs. There are several common elements shared among these algorithms, with variation mostly in the duration spent in each step.
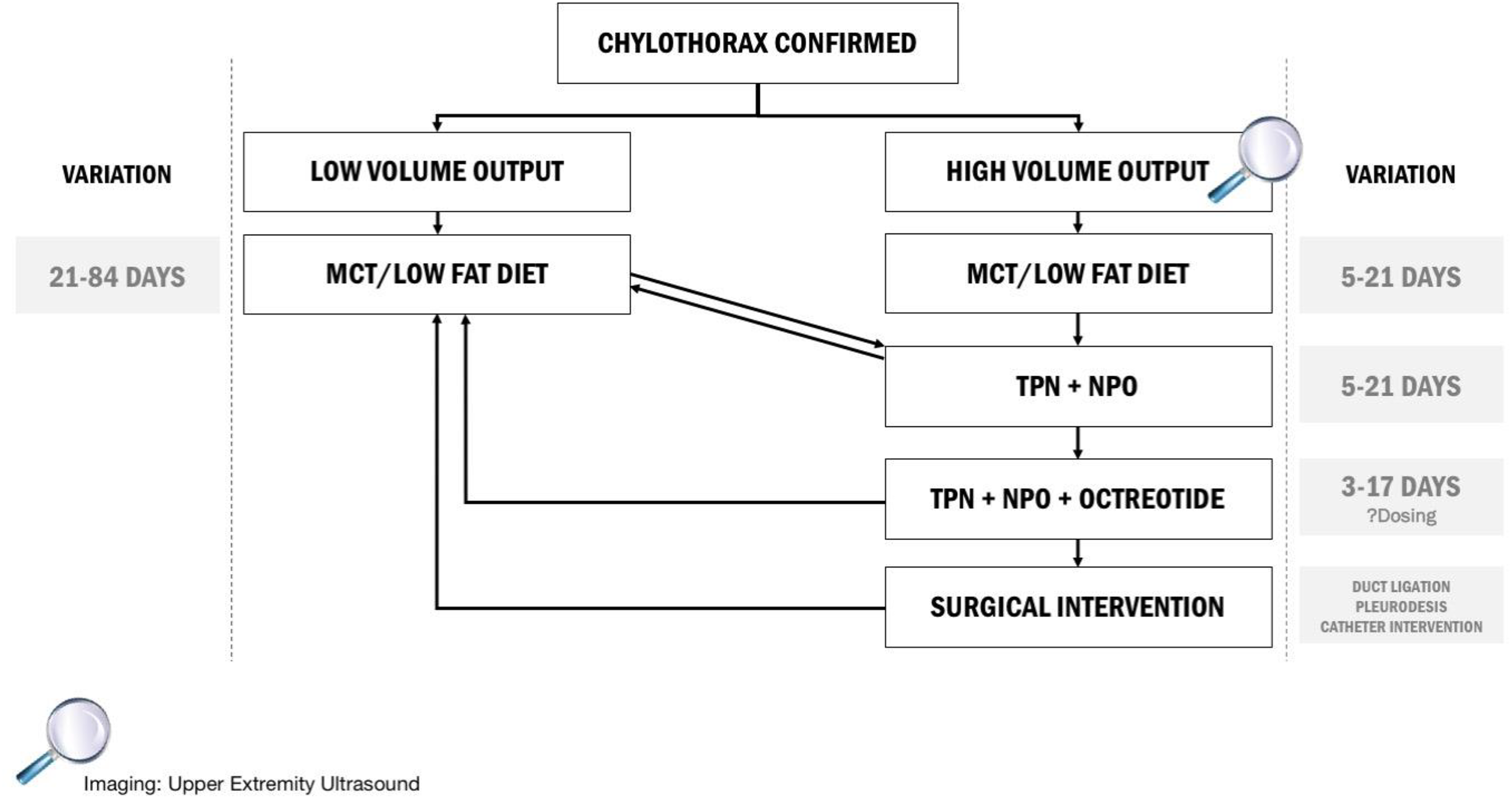
Summary of published chylothorax protocols and practice patterns from over 50 international ICUs managing postoperative congenital heart disease patients.
There exists virtual uniformity that two arms of an algorithm must be present: high-volume output and low-volume output. However, little consensus exists in what volume of drainage constitutes entry into each. Generally, drainage above 10 mL/kg/d warrants clinicians to categorize patients into the high output arm. Regardless of the volume of drainage, the first stage of the algorithms is a change to a medium-chain triglyceride or low-fat diet. 17,70,71 These types of fats, which are absorbed directly by the portal venous system, bypass the lymphatic system allowing for healing of a potentially traumatized lymphatic channel. Recent research has centered around the use of defatted mother’s milk as a potential alternative nutritional strategy with encouraging results. 72,73 The time spent using solely a change in nutritional composition varies significantly in both the low output arm (21-84 days) and high output arm (1-21 days).
Failure to diminish chylous drainage with an alternative nutritional strategy uniformly progresses patients to cessation of feeds (nil per os [NPO]) and starting TPN. This stage is also the entry point for patients who had entered the low chylous drainage arm with minimal change in drainage. Depending on the algorithm, patients could spend anywhere from 5 to 21 days in this stage.
After both alternative nutritional approaches and a period of NPO have been trialed without adequate cessation of drainage, the most common approach is the addition of octreotide to the NPO and TPN strategy. Continued use of octreotide is largely based on evidence from patients with congenital chylothorax, which represents a different pathophysiology than postoperative chyle leak. Even though the exact mechanism for the use of octreotide in congenital heart surgery is still relatively unknown, many algorithms still support its use prior to more invasive treatment regimens. The dose, uptitration, weaning, and duration of this strategy are all highly variable with little agreement across published and spoken algorithms. 74 –77
For patients refractory to these treatment modalities, the next stage in management is institution-specific. Most centers elect to perform pleurodesis or ligation of the thoracic duct with varying success. However, due to anatomic variability of the lymphatic system in children with CHD, 78 as well as potential incorrect identification of channel injury, results have been mixed. 79 –81
Recently, considerable progress has been reported in catheter intervention with embolization of affected lymphatic channels, a technique garnered from patients with plastic bronchitis and in adults with traumatic thoracic duct leak. 82,83 This strategy allows for direct visualization of the lymphatic system to identify the potential pathology of chyle leak and the ability to target the affected area directly. 84,85 Although success with this treatment course is promising, published results have been limited to single-institution experience.
Imaging
Once children have met criteria for entering a treatment algorithm, early monitoring for the development of venous clots as a cause of the chylous leak has been advocated for by multiple institutions. Since the left subclavian vein is the most common site of drainage of the thoracic duct near its junction with the left internal jugular vein, most centers advocate for upper limb ultrasound to identify the structure. Given the anatomic variability of the lymphatic system, bilateral imaging is prudent.
Replacements
Throughout the informal survey, no trends emerged regarding the replacement of either the constituents of chyle or the volume lost. Although the replacement of elements such as electrolytes are commonplace in both intensive care and inpatient ward settings, other components such as albumin, immunoglobulins, fibrinogen, and other proteins and clotting factors are harder to resolve. A study of patients with chylothorax who were randomized to either receive immunoglobulin supplementation or not did not show a difference in infectious outcomes. 86 This finding is in the face of significant infectious morbidity in both the treated and nontreated groups, displaying that the loss of these factors has clinical significance. To answer the question of supplementation of more complex losses, further large-scale studies are required. Until further data are obtained, routine investigations cannot be recommended but must be tailored on a case-by-case basis.
Can Feeding Improve Outcomes Beyond Providing Nutrients?
Understandably, the primary target for enteral feeding algorithms in critically ill infants and children with CHD has been meeting the patient’s caloric requirements in an effort to avoid the catabolic state often associated with critical illness. In addition, there is reason to suspect that provision of EN provides numerous additional benefits beyond caloric delivery, and research has shown that clinical outcomes may be optimized through modifications of substrate delivery.
Feeding, Mucosal Injury, and the Inflammatory Cascade
Although children are admitted to the ICU for various etiologies, many experience an intense systemic inflammatory response that becomes a key element of their illness. The biochemical cascades that result from and further perpetuate this systemic inflammation are associated with end-organ dysfunction, prolonged length of stay, and death. 87,88 It is generally believed that enteral feeding exerts many of its beneficial effects through attenuation of this inflammatory response. Lowering the inflammatory burden is thought to result in improved wound healing, a decrease in acquired infections, and shorter ICU and hospital admissions. 89
Injury to the GI tract is common in critical illness secondary to altered perfusion, hypoxia, and systemic acidosis. These areas of vulnerability result in disruption to the epithelial brush border and tight junctions and allow for translocation of bacteria from the internal lumen into the surrounding tissues. Migration of granulocytes then ensues as part of a complex immune-mediated response in which further injury is mediated by release of cytotoxic chemicals and cytokines and a positive feedback loop is created that culminates in a system-wide inflammatory response. Enteral nutrition may attenuate these events by preserving gut integrity.
Animal and adult studies suggest that gut integrity is compromised during periods of fasting and protected with initiation of feeds. Hernandez and colleagues demonstrated that prolonged fasting in critically ill patients was associated with decreased absorption and increased GI permeability. 90,91 Biopsies confirmed villous atrophy, shorter villi height, and shallower crypts in affected GI mucosa. Unlike patients given TPN, EN was associated with recovery of usual function. 91
Despite the strongly held belief, the data supporting a direct link between EN, inflammation, and clinical outcome are limited. Some evidence has emerged from studies of children undergoing cardiac surgery, a population known to have a predictable inflammatory response following cardiopulmonary bypass. In a representative cohort, the odds of organ injury and morbidity was strongly associated with height of inflammation and degree of insulin resistance. 92 This positive association held true for patients who were fasting or receiving minimal feeds but not for those on liberal EN. 93
Dose–Response
Early EN, started within 24 to 48 hours of ICU admission, has been shown to improve EN delivery and is strongly associated with a reduction in ICU-related infections and duration of hospitalization. 89,94 Rapidly increasing EN and earlier attainment of goal volumes have also been associated with lower infectious complications and shorter intervals of care. 89 Although these results are limited to observational studies, mainly of adult patients, similar findings have been found in children, including high-risk patients with CHD. 29,95
The optimum goal for the provision of EN remains unclear. Enteral nutrition delivery was historically targeted to meet each patient’s metabolic demands with the idea that clinical outcomes are optimized when avoiding underfeeding or overfeeding. More recently, limiting EN with permissive underfeeding has been shown to improve clinical outcomes in some, but not all, studies. In the largest trial, the PermiT study, adults receiving 40%-60% of goal feeds had similar mortality and ICU morbidity (acquired infection, electrolyte imbalance, and feeding intolerance) compared to those receiving standard of care (70%-100% of energy expenditure). 96 This supports growing concern that higher EN delivery may reduce autophagy, a critical housekeeping pathway used by cells to limit cell and tissue injury. Autophagy, the process by which organelles are internally digested without release of cytotoxic chemicals that can promote inflammation, is strongly inhibited by both increased nutrition and insulin. 97
Macronutrients
A growing body within nutrition sciences has focused on improving clinical outcomes through modifications to the provision of macronutrients. Particular attention has been paid to protein delivery, with data demonstrating an association between higher protein intake and survival. 6 Although pediatric studies are challenged with higher protein delivery intimately associated with higher caloric delivery, Rugeles and colleagues showed that increased protein delivery was associated with a decrease in organ injury even after controlling for caloric intake. 98 The use of protein supplementation has also been used as a potential explanation for the positive results associated with permissive underfeeding. 96 In contrast, clinical outcomes in a large cluster randomized trial were not affected by increased protein delivery, 99 and a similar negative result was found using intravenous protein supplementation, although both aforementioned studies were not powered for this secondary outcome. 100
Benefits of EN supplementation with specific amino acids, namely glutamine and
Conclusion
In summary, perioperative feeding management is an important modifiable target to improve outcomes after cardiac surgery, yet optimum practices are not well defined. Provision of EN has been largely determined by institutional practice with predictably wide variability. There is significant variation in which patient populations are considered safe to feed, the timing and type of EN provided, and the feeding protocols, if any, that are utilized. When feeding complications, such as chylothorax, occur postoperatively, considerable variation exists in the treatment approach. Collaboration among centers is necessary to better understand the factors that drive practice variation and help identify specific nutritional strategies that may improve outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.