
Abstract
Background:
Single ventricle (SV) patients with total anomalous pulmonary venous connection (TAPVC) are at high risk. Given the limited published data available, we examined outcomes and the implications of a prenatal diagnosis of SV/TAPVC.
Methods:
A single-center, retrospective review was performed in neonates with SV/TAPVC from 1998 to 2014, identified through institutional databases. Patient demographic, perioperative, and follow-up data were collected.
Results:
Thirty-four eligible infants with SV/TAPVC were identified (mean birth weight: 3.0 kg). The TAPVC types were supracardiac (59%), infracardiac (21%), mixed (12%), and cardiac (9%). Heterotaxy syndrome was present in 25 (74%) infants. A prenatal diagnosis of SV was made in 26 (76%) infants, with TAPVC identified in 12 (35%). Seventeen (50%) had obstructed TAPVC within the first 48 hours of life; 7 of these patients had obstructed TAPVC identified prenatally. There were two preoperative deaths. Overall survival for the cohort was 65% at 1 year and 50% at 3 years. Survival in the obstructed group was significantly worse compared to the unobstructed group (47% vs 81% at 1 year; 27% vs 73% at 3 years, P = .01). Obstructed TAPVC and a prenatal prediction of obstructed TAPVC were significantly associated with postoperative mortality (P = .01 and .03, respectively).
Conclusions:
Patients with SV/TAPVC remain a high-risk group, with obstructed TAPVC a significant risk factor for mortality. Prenatal diagnosis of TAPVC in SV patients is challenging, but given those with obstructed TAPVC are especially at high risk, improved prenatal diagnostic techniques in this group may enhance counseling/delivery planning.
Keywords
Introduction
Despite improvement in early survival in recent years, patients with single ventricle (SV) heart disease and total anomalous pulmonary venous connection (TAPVC) remain a high-risk group of SV patients. 1,2 According to one report, survival at one month was 65% for SV patients versus 90% for two-ventricle patients. 3 Risk factors for mortality in this group include obstructed TAPVC, younger age at the time of initial surgery, and TAPVC repair at the initial surgery. 2 In fact, outcomes are rather poor for SV patients requiring repair of obstructed TAPVC in the neonatal period, with almost 60% mortality, 4 and the SV population is at increased risk of pulmonary vein stenosis requiring reoperation compared to those patients with biventricular physiology. 5 A recent multicenter study from the Society of Thoracic Surgeons Congenital Heart Surgery Database investigating outcomes in two-ventricle and SV patients with TAPVC and heterotaxy syndrome reported an overall hospital discharge mortality of 38%, with significantly worse early outcomes in the SV group of patients. 6
The majority of SV patients (75% by recent data from the Pediatric Heart Network Single Ventricle Reconstruction Trial) are diagnosed prenatally. 7 Although variable data exist regarding the impact of prenatal diagnosis on postoperative survival of SV infants, 8,9 prenatal diagnosis allows for counseling and delivery planning for fetuses presenting with high-risk lesions. The implications of prenatal diagnosis of a high-risk SV population with obstructed TAPVC are not well known. Therefore, the aims of this study were to describe a single-center experience with this extremely high-risk SV population, examine outcomes, and the implications of a prenatal diagnosis of SV/TAPVC in the current era, in order to enhance counseling for families presenting to a center’s prenatal heart program.
Patients and Methods
Patients with SV heart lesions and TAPVC born at or presenting to the University of Michigan Congenital Heart Center from January 1, 1998, to December 31, 2014, were identified through institutional databases. Retrospective chart review was performed, with data collected including demographics, preoperative, operative, postoperative, and follow-up data. Pre-operative data collected included fetal and postnatal echocardiogram results, place of birth, SV lesion type, presence of heterotaxy, TAPVC type, mechanism of obstruction, mean gradient at the site of obstruction, preoperative death, and whether or not the patient was listed for heart transplantation. The diagnosis of pulmonary venous connection obstruction was determined by clinical assessment as documented in the patient medical record including echocardiographic data. Operative data included age at initial operative intervention and type of initial and subsequent surgical procedures performed. Postoperative data included postoperative transesophageal/transthoracic echocardiogram results (N = 28 available), need for reintervention, need for extracorporeal membrane oxygenation, hospital survival, days spent in the intensive care unit, and total hospital days for the initial hospitalization. If postoperative death occurred, timing of death was collected. Operative mortality was defined as death occurring within 30 days after the initial surgery in or out of the hospital or after 30 days during the same operative hospitalization. Follow-up data included the SV palliative operations. If death occurred later in follow-up, age at the time of death was collected. If a patient was identified as “lost to follow-up,” the National Death Index (NDI) was searched to identify if death had occurred. This study was approved by the institutional review board of University of Michigan Medical School.
Data are reported as frequency and percentage for categorical variables, and mean and standard deviation or median and interquartile range, depending on the distributional assumption, for continuous variables. Preoperative, operative, postoperative, and follow-up data were compared between SV patients with and without obstructed TAPVC using χ2 test or Fisher exact test for categorical variables and Wilcoxon rank sum test or t test for continuous variables. The overall survival after initial surgery was generated by Kaplan-Meier curve and was compared between patients with and without obstructed TAPVC using log-rank test. Univariate Cox regression was used to identify patient and clinical characteristics associated with postoperative mortality. Hazard ratio and 95% confidence interval from the regression were reported. All analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, North Carolina). A P value of <.05 was considered statistically significant.
Results
Thirty-five infants with SV heart disease and TAPVC were identified. After excluding 1 patient (due to the first operation occurring at an outside institution), a total of 34 patients were included in the analysis. Demographics and preoperative characteristics are shown in Table 1. The TAPVC types were supracardiac (59%), infracardiac (21%), mixed (12%), and cardiac (9%). Heterotaxy syndrome was present in 25 (74%) patients. Seventeen (50%) patients had obstructed TAPVC within the first 48 hours of life. A prenatal diagnosis of SV disease was made in 26 (76%) patients. Total anomalous pulmonary venous connection was identified in 12 (35%) of 34 total patients, more often diagnosed prenatally in the obstructed group (53% vs 18%, P = .03). Obstructed TAPVC was predicted prenatally in 7 of 12 patients, and all 7 had obstructed TAPVC diagnosed postnatally. Two patients with prenatally diagnosed TAPVC were obstructed postnatally without a prenatal prediction of obstructed TAPVC. In order to describe prenatal diagnosis with respect to era, the cohort was split into patients from the years of 1998 to 2006 (group A: 15/34, 44%) and 2007 to 2014 (group B: 19/34, 56%). All 12 patients with TAPVC identified prenatally and therefore the 7 patients with obstructed TAPVC predicted prenatally were in group B, the more current era. The mean birth weight was 3.04 kg (range: 2.0-3.8 kg), and two patients were born prematurely at less than 37 weeks of gestation. There were two preoperative deaths (both of these deaths were due to withdrawal of care in patients with obstructed TAPVC due to multiple anomalies in one patient and complexity of anatomy in the other patient).
Demographics and Preoperative Characteristics of Single Ventricle Patients With Total Anomalous Pulmonary Venous Connection.a
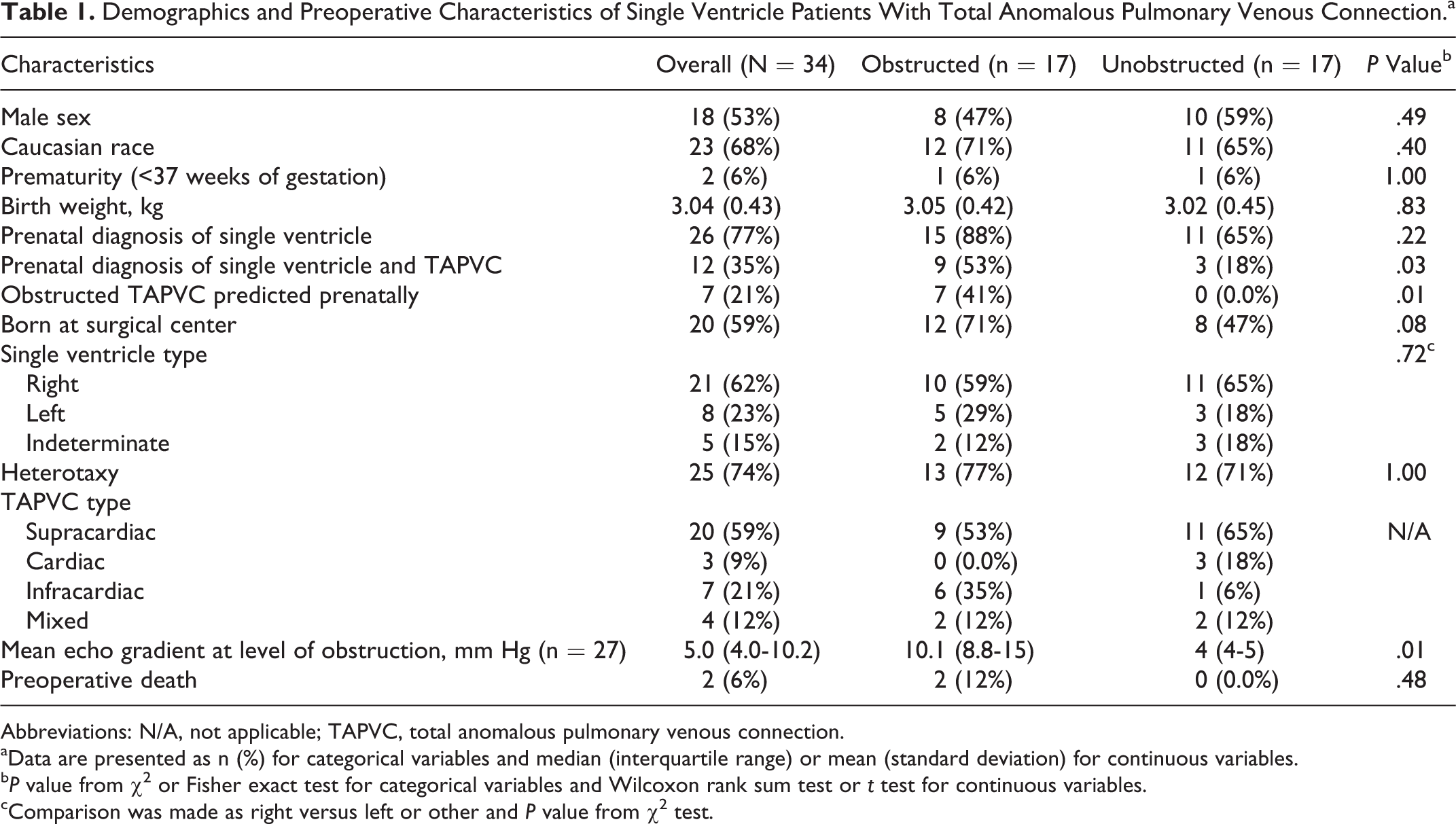
Abbreviations: N/A, not applicable; TAPVC, total anomalous pulmonary venous connection.
aData are presented as n (%) for categorical variables and median (interquartile range) or mean (standard deviation) for continuous variables.
b P value from χ2 or Fisher exact test for categorical variables and Wilcoxon rank sum test or t test for continuous variables.
cComparison was made as right versus left or other and P value from χ2 test.
Operative mortality for the cohort was 31% overall and was significantly worse for the obstructed TAPVC group (53% in the obstructed group vs 12% in the unobstructed group; P = .02). Ten patients underwent the initial surgery within the first 24 hours of life, with nine of these ten patients having obstructed TAPVC. The majority of patients (72%) had TAPVC repair as part of their initial surgery (Table 2).
Operative and Postoperative Characteristics of Single Ventricle Patients With Total Anomalous Pulmonary Venous Connection.a
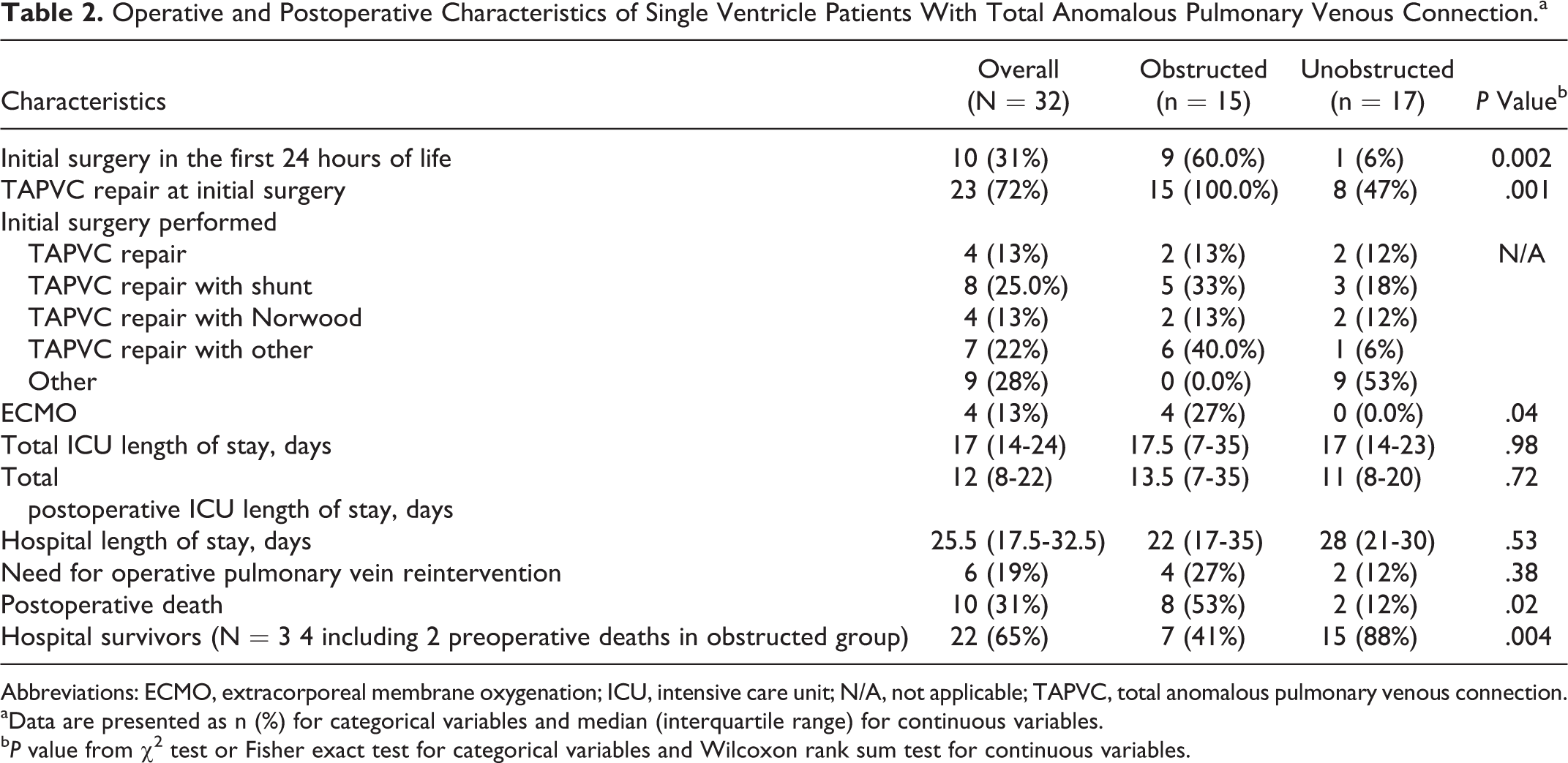
Abbreviations: ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; N/A, not applicable; TAPVC, total anomalous pulmonary venous connection.
aData are presented as n (%) for categorical variables and median (interquartile range) for continuous variables.
b P value from χ2 test or Fisher exact test for categorical variables and Wilcoxon rank sum test for continuous variables.
Of the 22 hospital survivors, 20 (91%) patients underwent a cavopulmonary shunt and 9 (41%) patients went on to have a Fontan operation. One patient was lost to follow-up, and it is unknown whether that patient underwent a cavopulmonary shunt, and one patient died prior to stage 2 palliation after pulmonary vein stenosis was treated with pulmonary vein stenting and experimental chemoprophylaxis to prevent pulmonary vein reocclusion. Only three patients from the obstructed TAPVC group have undergone a Fontan operation, and one of these three patients died after the Fontan. At the time of data collection and analysis, five patients were awaiting a Fontan (four from the unobstructed group) and two patients were not Fontan candidates (one obstructed TAPVC and one unobstructed TAPVC). During median duration of follow-up of 3.6 years since initial surgery (range: 0.4-15.9 years), there were five late deaths. Two patients were lost to follow-up, although death was not identified for these patients following inquiry of the NDI. Notably, from the obstructed cohort, only 3 of 15 patients are alive after the initial surgery and are either eligible for a Fontan or have undergone a Fontan, whereas 10 of 17 patients in the unobstructed cohort are eligible or have had a Fontan. Figure 1 displays midterm outcomes of patients by obstructed and unobstructed TAPVC. Survival after initial surgery in the obstructed group was significantly worse compared to the unobstructed group (P = .01; Figure 2). Obstructed TAPVC and a prenatal prediction of obstructed TAPVC were significantly associated with postoperative mortality (P = .01 and .03, respectively; Table 3). There was no significant difference in early operative or late mortality in patients with obstructed TAPVC between those diagnosed prenatally with obstructed TAPVC and those without a prenatal diagnosis of obstruction (data not shown).
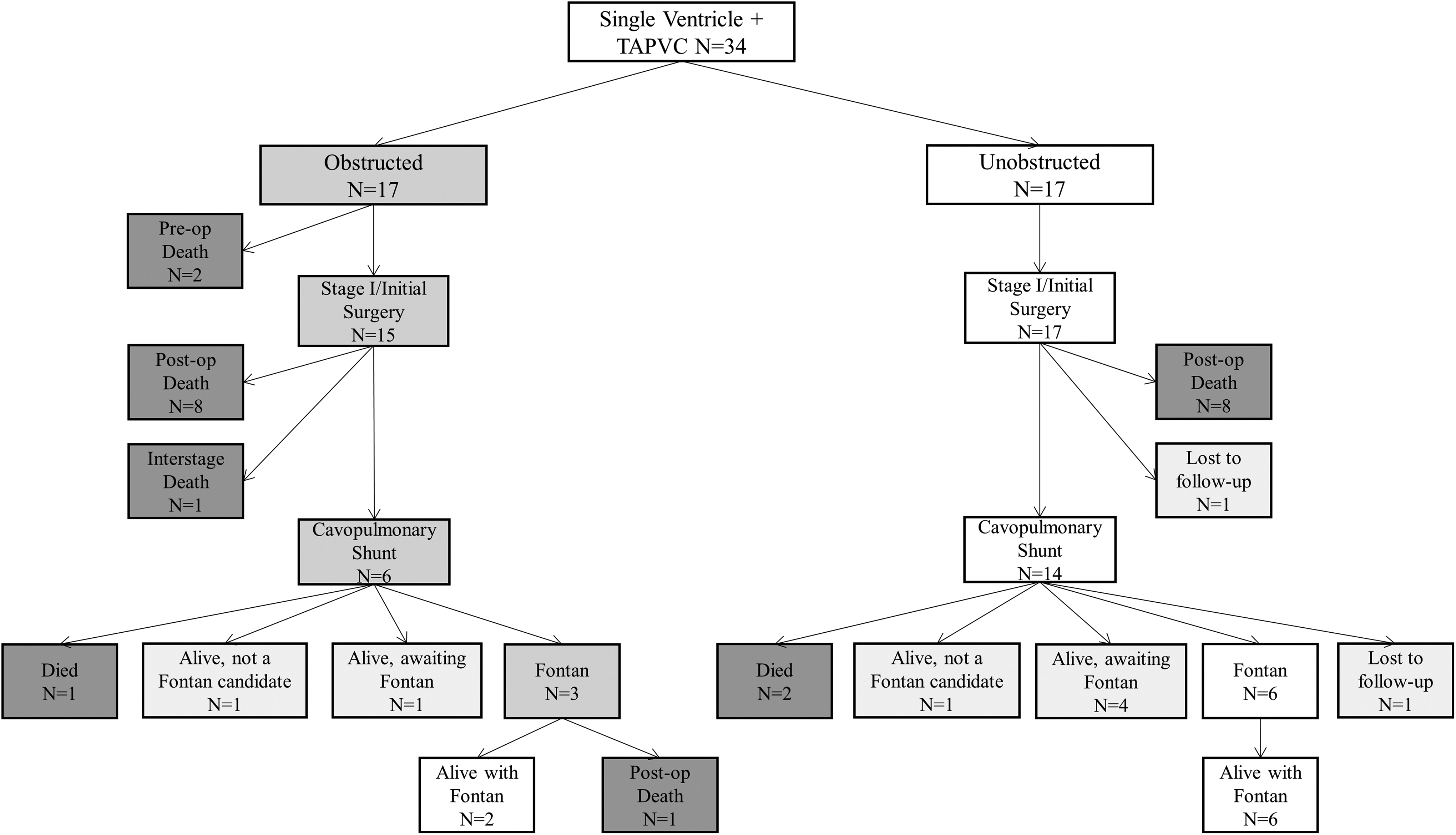
Flow diagram of single ventricle patients by obstructed and unobstructed total anomalous pulmonary venous connection (TAPVC).
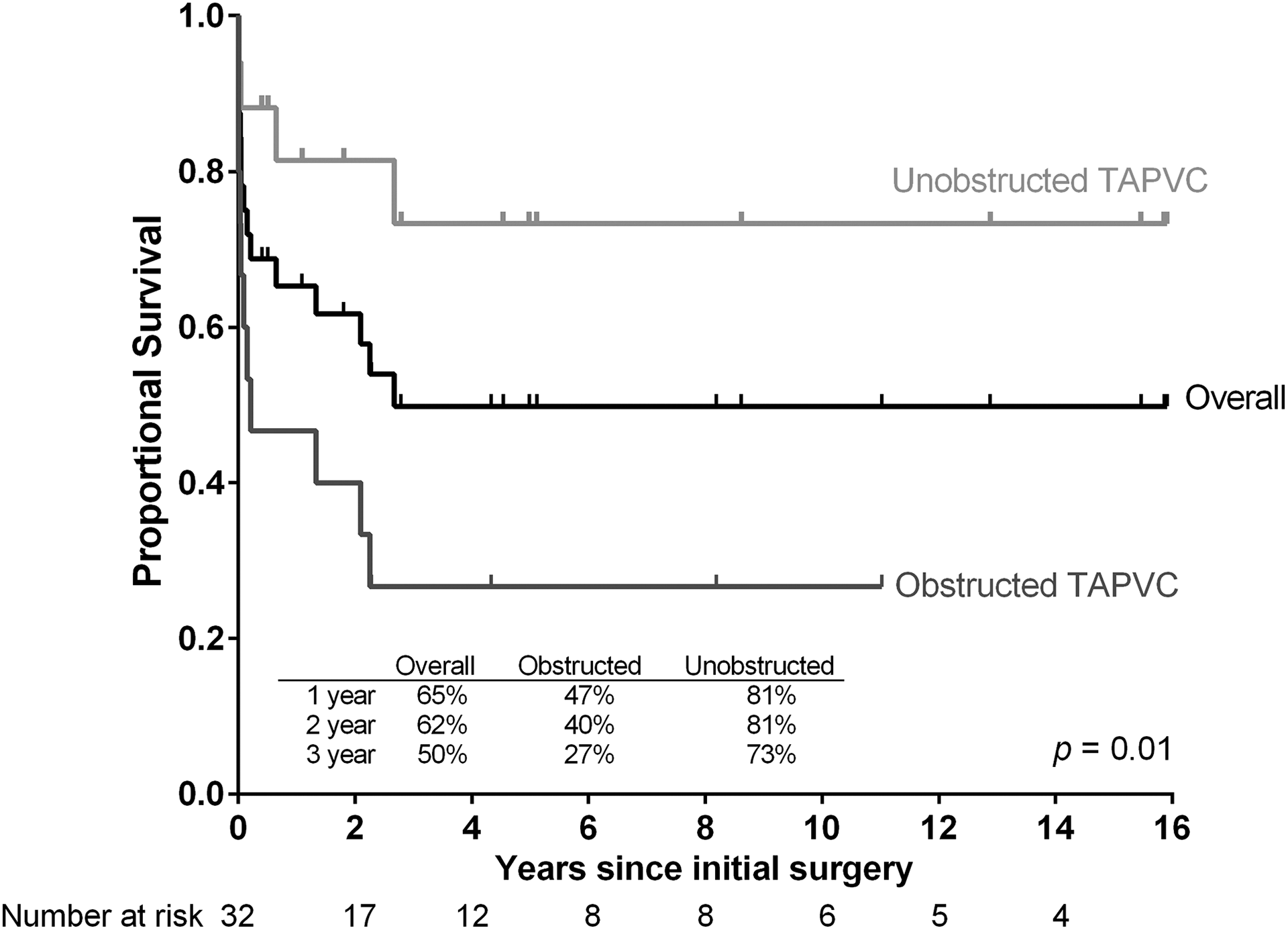
Survival after initial surgery in overall and by obstructed/unobstructed total anomalous pulmonary venous connection (TAPVC) in single ventricle patients (N = 32). Median overall survival was at 2.7 years after initial surgery.
Preoperative and Operative Characteristics Associated With Mortality After Initial Surgery for Single Ventricle Patients With Total Anomalous Pulmonary Venous Connection.a,b
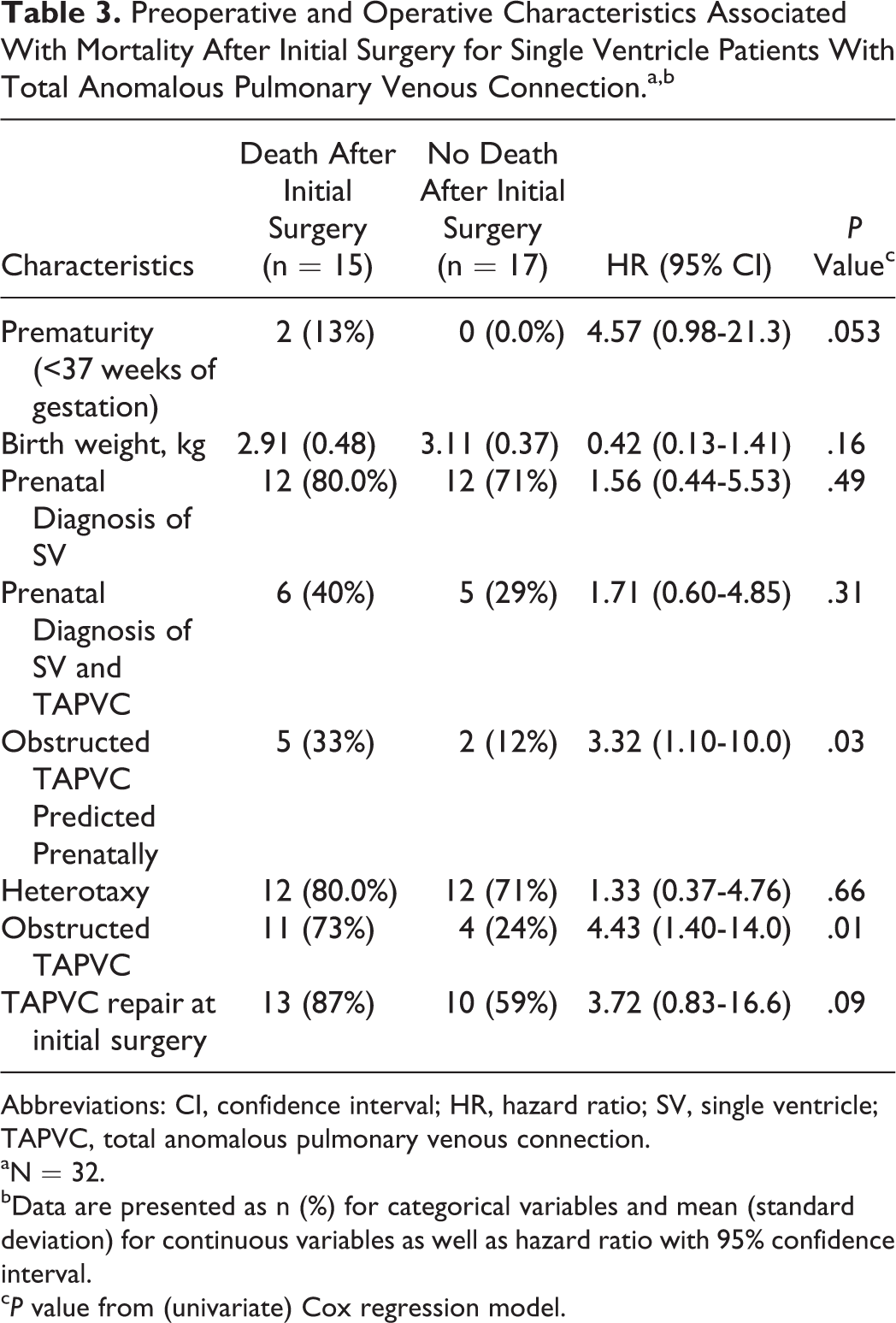
Abbreviations: CI, confidence interval; HR, hazard ratio; SV, single ventricle; TAPVC, total anomalous pulmonary venous connection.
aN = 32.
bData are presented as n (%) for categorical variables and mean (standard deviation) for continuous variables as well as hazard ratio with 95% confidence interval.
c P value from (univariate) Cox regression model.
Comment
Patients with SV heart disease and TAPVC are a high-risk group. A prior single-center report demonstrated improved early survival in a more contemporary cohort of patients, although intermediate survival remained approximately 50%. 1 A recent multicenter study evaluating contemporary outcomes in patients with TAPVC and heterotaxy syndrome reported that early outcomes of TAPVC repair in the subset of heterotaxy patients with SV physiology remain significantly worse than those with biventricular circulation. 6 The purpose of our study was to add to the currently small body of literature on this high-risk subset of SV patients and to examine the implications of a prenatal diagnosis of SV/TAPVC in the current era of prenatal diagnosis and counseling. Our data continue to demonstrate that this SV population with TAPVC remains a high-risk group of SV patients, and obstructed TAPVC is an even greater risk factor for mortality. Additionally, despite the often multiple fetal echocardiograms performed in fetuses with SV heart disease, prenatal detection of TAPVC remains challenging. However, a prenatal diagnosis of obstructed TAPVC in this group is predictive of postnatal obstruction.
The majority of data available in this complex subset of SV patients are based on single institutional studies. For example, Lodge et al reported improving early survival in patients with SV heart disease and TAPVC, with the 30-day survival being 89% in a group of 18 patients treated from 1998 to 2003 (of which, 33.3% had obstructed TAPVC). 1 This was in comparison to a prior study of 73 patients from the same institution in which the early mortality was 53% in patients from 1984 to 1997 (of which, 29% had obstructed TAPVC). 2 Another single institution study in 2005 from Hancock Friesen and colleagues reported on 39 patients with SV anatomy and TAPVC (22 [56%] with obstructed TAPVC) with one month survival of 65% with an early operative mortality of 36%. 3 In our study with a similar number of SV patients, we demonstrate overall hospital survival of 65% with an operative mortality of 31%, which was significantly worse for the obstructed TAPVC group at 53%. We found intermediate survival to be comparable to what has been previously reported of around 50% 1,10 for the entire cohort, with significantly worse intermediate survival in the obstructed group at 27% at 3 years. Despite it being a known operative risk factor for mortality, 6,11 the presence of heterotaxy syndrome was not significantly associated with operative mortality in our study, probably due to inadequate power for this analysis.
In the only multicenter study involving this complex group of SV patients with TAPVC, Khan et al described multi-institutional experience in heterotaxy patients with TAPVC with a subset of patients having SV physiology. Although data were collected on preoperative risk factors, this study did not report the impact of obstructed TAPVC in this recent cohort. Multicenter data on the long-term outcomes of patients with SV and obstructed TAPVC are also lacking. In our study, 7 of 17 patients with obstructed TAPVC survived to hospital discharge. Only 3 of these patients have undergone a Fontan operation, and one has died. Larger, multi-institutional experience is needed to further characterize the long-term outcomes in this very high-risk group of patients, in order to adequately counsel families presenting with a prenatal diagnosis.
However, prenatal diagnosis of TAPVC is difficult, as demonstrated by multiple studies. 12 –18 As part of a study evaluating a cohort of patients with heterotaxy syndrome with functional SV and the impact of prenatal diagnosis, low sensitivity for the diagnosis of anomalous pulmonary veins was demonstrated. 14 Similarly, in our study, only 12 (35%) of the 34 total patients were diagnosed prenatally with TAPVC. Interestingly, a prenatal diagnosis was more often made in the obstructed group, perhaps due to the ability to visualize some of the markers for TAPVC obstruction by fetal echocardiogram, including continuous turbulent flow present in a vertical vein or monophasic continuous flow in the pulmonary veins. 19 There was no difference in outcome in those with a prenatal diagnosis of obstructed TAPVC compared to those without a prenatal diagnosis of obstruction, although there was insufficient power for this analysis. However, if obstructed TAPVC is detected prenatally, it is predictive of postnatal obstruction. In our center, we identify fetuses with SV/TAPVC for specialized delivery care in the immediate neonatal period due to the potential need for immediate specialized procedures such as cardiac surgery or catheterization. A detailed delivery and immediate postnatal plan with a multi-specialty group including maternal fetal medicine, neonatology, pediatric cardiology, and pediatric cardiac surgery is made. Due to the very-high-risk nature of this lesion confirmed by this study and other studies, 1 –6 families are counseled regarding the increased risk of early operative mortality, the poor long-term survival for patients with obstructed TAPVC, and the option of comfort care after delivery.
Given the persistently poor outcomes in this high-risk group of SV patients, this may be a group to target for fetal intervention, an area of future investigation. Although preliminary data have not shown a significant survival benefit for fetal intervention for hypoplastic left heart syndrome with intact or highly restrictive atrial septum, research is ongoing, 20 and this technique is evolving.
The main limitation of this study is that it is a retrospective review from a single institution. Additionally, given that this is a rare subgroup of SV patients, only a small number of patients were available for analysis. Therefore, this may impact the study results, due to inadequate power. For instance, heterotaxy syndrome is a known operative risk factor for mortality in other studies but was not shown to be significantly associated with operative mortality in our study.
In conclusion, early operative mortality remains high for patients with SV heart disease and TAPVC and in those patients with obstructed TAPVC specifically. This subgroup of SV patients remains a high-risk group beyond the initial hospitalization, with 3-year survival being particularly poor in the obstructed patients. Identification of obstructed TAPVC in the prenatal period is predictive of postnatal obstruction and is important for optimal prenatal counseling and delivery planning. Prenatal diagnosis of TAPVC in the SV population, however, remains challenging, and future studies investigating additional fetal diagnostic techniques and therapeutic interventions may be advantageous.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.