
Abstract
Background:
Dexmedetomidine has been suggested as an arrhythmia prophylactic agent after surgery for congenital heart disease due to its heart rate lowering effect, though studies are conflicting. We sought to study the effect of dexmedetomidine in infants that are at highest risk for arrhythmias.
Methods:
Retrospective cohort study of infants less than six months of age undergoing cardiopulmonary bypass for congenital heart disease. The arrhythmia incidence in the first 48 hours after surgery in infants receiving dexmedetomidine for sedation was compared to those that did not receive dexmedetomidine.
Results:
A total of 309 patients were included, 206 patients who did not receive dexmedetomidine and 103 patients who did. The incidence of tachyarrhythmias was similar between the non-DEX group and the DEX group (19% vs 15%, P = .34). When adjusted for baseline differences, the non-DEX group did not have an increased risk of postoperative tachyarrhythmias (odds ratio [OR]: 1.4, 95% confidence interval [CI]: 0.5-3.8). The non-DEX group had an increased need for treatment for arrhythmias (18% vs 8%, P = .012). The three lesions with baseline higher risk for arrhythmias (tetralogy of Fallot, transposition of the great arteries, and complete atrioventricular canal) had an increased incidence of tachyarrhythmias in the non-DEX group (34% vs 6%, P = .027). This risk was not significant in multivariate analysis (OR: 2.5, 95% CI: 0.4-15.5).
Conclusions:
High-risk infants had decreased incidence of tachyarrhythmias when receiving dexmedetomidine, though this was not significant after accounting for baseline differences between groups.
Introduction
Arrhythmias are common after surgery for congenital heart disease, occurring in up to a third of patients within the first three days after surgery. 1,2 While postoperative arrhythmias are often treatable and self-limited, they can be detrimental to patients with diminished cardiac reserve after surgery, leading to increased morbidity and length of stay. 3,4 The treatments currently available can be associated with serious adverse effects. In a prospective study on the use of amiodarone for incessant tachyarrhythmia, 87% of children experienced adverse effects including hypotension, bradycardia, and heart block. 5 Due to these concerns, various preventive strategies have been studied with the goal of reducing postoperative arrhythmias while minimizing cardiovascular side effects.
Dexmedetomidine is a selective α2-adrenoreceptor agonist that is being increasingly used for sedation in children after cardiac surgery due to its favorable hemodynamic profile. 6,7 Dexmedetomidine has been found to depress sinoatrial and atrioventricular nodal function and reduce postoperative catecholamine levels. 8,9 These effects suggest that it may have a role as a prophylactic agent for arrhythmias. The perioperative use of dexmedetomidine was found to decrease both ventricular and supraventricular tachyarrhythmias in one small study. 10 However, a recent report of 1,593 patients found no association between dexmedetomidine exposure and arrhythmias after propensity score matching. 11 Additionally, symptomatic bradycardia may occur. 12,13
Current published studies include older children who are at low risk for arrhythmias and may not benefit from prophylaxis. The association between dexmedetomidine use and arrhythmias has not been studied specifically in young infants, though these patients are at higher risk for arrhythmias than older children. 1 Our aim was to evaluate the effects of dexmedetomidine on both tachy- and bradyarrhythmias in infants less than six months of age undergoing cardiopulmonary bypass for congenital heart surgery. We hypothesized that these patients would have a decreased incidence of postoperative tachyarrhythmias, but an increased incidence of bradyarrhythmias.
Patients
This study was performed at Children’s Mercy Hospital and approved by the institutional review board. All infants less than 6 months of age undergoing cardiopulmonary bypass for congenital heart disease from January 1, 2010, to June 30, 2014, were eligible for inclusion. Patients were excluded if they had received dexmedetomidine within the 72 hours prior to surgery or were in a nonsinus rhythm at admission to the pediatric intensive care unit (PICU). Only the first surgery during a hospital stay was included.
Use of dexmedetomidine in the operating room was at the discretion of the anesthesiologist and pre and postoperative use was determined by the PICU team. All patients had temporary pacing wires placed. The dexmedetomidine group (DEX) consisted of patients who received the drug for greater than 1 hour in the first 48 hours after PICU admission. The control group consisted of (non-DEX) patients who either never received the drug during the study time frame or did not receive it until after the start of an arrhythmia.
The primary outcome was the incidence of tachyarrhythmias and bradyarrhythmias in the first 48 hours after surgery. This was determined by a retrospective chart review of both cardiology and critical care documentation. Tachyarrhythmia was defined as any nonsinus rhythm with a rate greater than 100 bpm. Tachyarrhythmias were divided into subgroups: atrial tachycardias, junctional accelerated rhythm (100-165 bpm), junctional ectopic tachycardia (JET; >165 bpm), reentrant supraventricular tachycardia, and ventricular tachycardias. Treatment for tachyarrhythmia was defined as administration of an antiarrhythmic medication after the start of the arrhythmia, use of rapid atrial pacing, or cardioversion/defibrillation. Bradyarrhythmia was defined as any sinus or nonsinus rhythm that required temporary pacing due to an age-inappropriate rate. Bradycardia subgroups included complete heart block, junctional rhythm with a rate less than 100 bpm, and slow sinus rhythm requiring pacing. Sinus tachycardia was determined by review of vital sign charting and was defined as a sinus rhythm with a rate greater than 165 bpm. Secondary outcomes included sedative use, length of mechanical ventilation, and intensive care unit (ICU) and hospital length of stay.
Subgroup analysis was performed on the three lesions at highest risk for postoperative arrhythmias based on a review of the literature and our own internal data: transposition of the great arteries, complete atrioventricular canal, and tetralogy of Fallot. 3 Study data were collected and managed using REDCap (v 8.4.3) electronic data capture tools 14 hosted at Children’s Mercy Hospital. Statistical analysis was performed using IBM SPSS Statistics version 23 (Armonk, New York) and R Statistical Software version 1.1.414 (Vienna, Austria). Demographic and clinical data were compared between the non-DEX and DEX groups using the Pearson χ2 for categorical values and Wilcoxon rank sum test for continuous variables. Multivariate analysis of odds ratio was used to assess the strength and direction of association between demographic and clinical data with the response variables. All P values are two sided with the level of significance set at .05.
Results
A total of 362 patients were screened. Four were excluded for preoperative dexmedetomidine use and 49 for being in an arrhythmia at admission to the PICU. Of the 309 remaining patients, 206 did not receive dexmedetomidine or received it after the start of an arrhythmia and comprised our non-DEX group, while 103 received dexmedetomidine (DEX group). Preoperative patient characteristics are listed in Table 1. The non-DEX group was younger, had shorter cross-clamp time, and was more likely to have delayed sternal closure compared to the DEX group.
Patient Characteristics.a
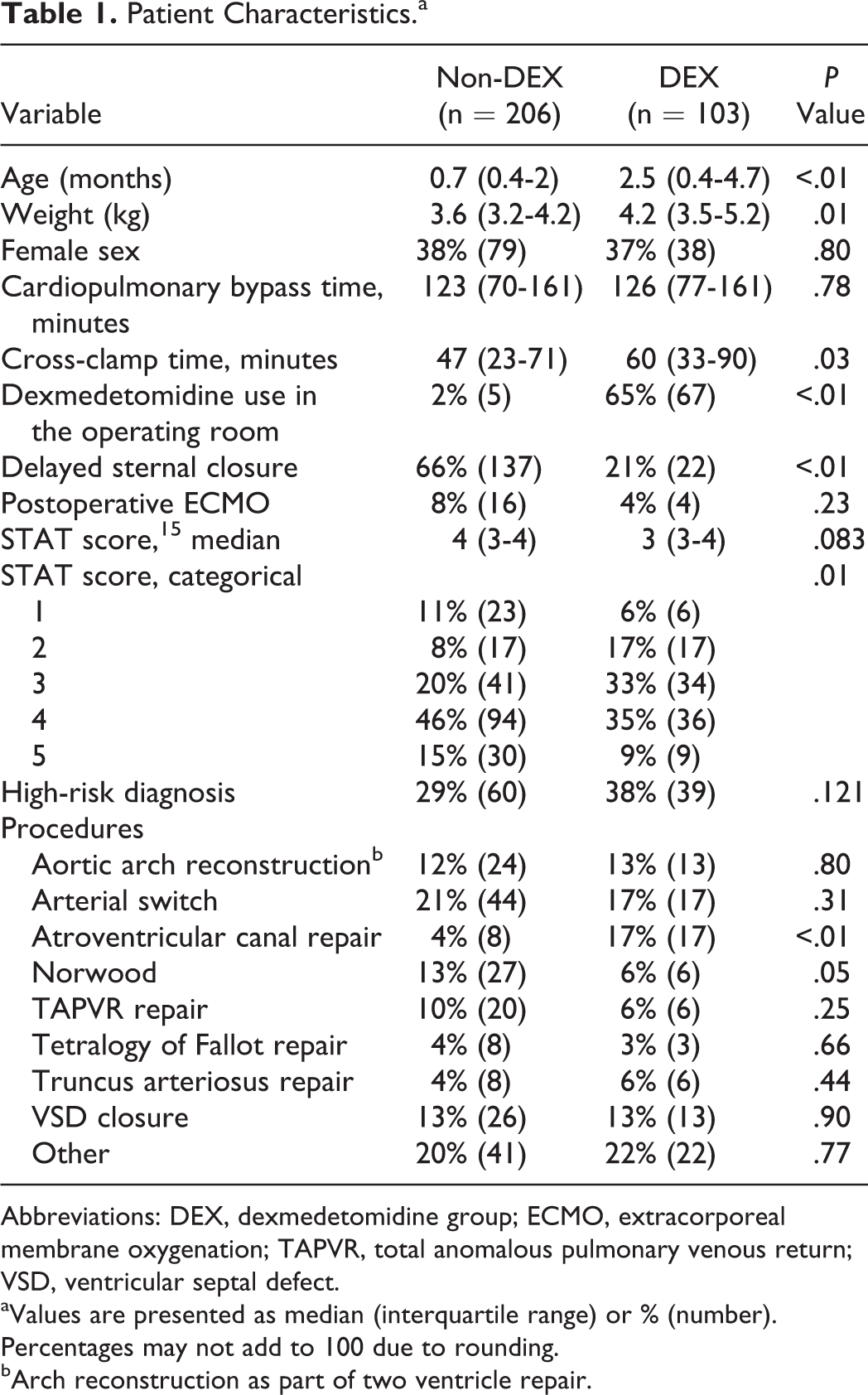
Abbreviations: DEX, dexmedetomidine group; ECMO, extracorporeal membrane oxygenation; TAPVR, total anomalous pulmonary venous return; VSD, ventricular septal defect.
aValues are presented as median (interquartile range) or % (number). Percentages may not add to 100 due to rounding.
bArch reconstruction as part of two ventricle repair.
The incidences of arrhythmias and treatments are shown in Table 2. The overall incidence of postoperative arrhythmias was similar between groups at 23%. There was no statistically significant difference in arrhythmia incidence between groups in any rhythm subcategory. Treatment for arrhythmias was increased in the non-DEX group, which was largely due to an increased use of amiodarone, 12.6% versus 4.9%, P = .03. There was no difference in bradyarrhythmias between groups. Logistic regression analysis was performed to assess the association of dexmedetomidine use and the incidence of arrhythmias, controlling for baseline differences between groups (Table 3). In this model, being in the non-DEX group did not increase tachyarrhythmias, (odds ratio [OR]: 1.40, 95% confidence interval [CI]: 0.51-3.84) or decrease bradyarrhythmias (OR: 0.89, 95% CI: 0.19-4.14).
Overall Incidence of Arrhythmias Between Groups.a
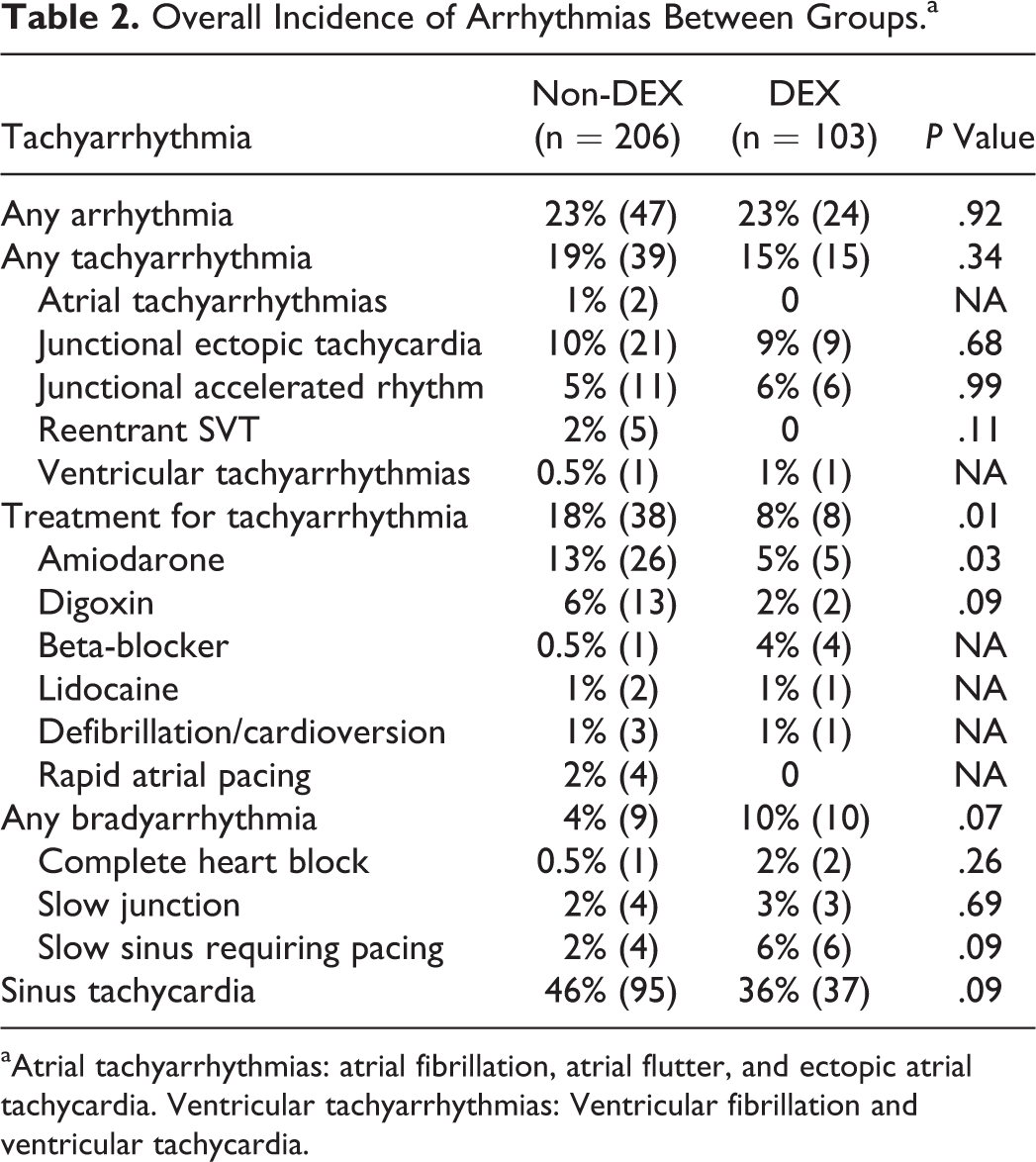
aAtrial tachyarrhythmias: atrial fibrillation, atrial flutter, and ectopic atrial tachycardia. Ventricular tachyarrhythmias: Ventricular fibrillation and ventricular tachycardia.
Multivariable Analysis of Postoperative Tachyarrhythmia Risk, Entire Cohort.
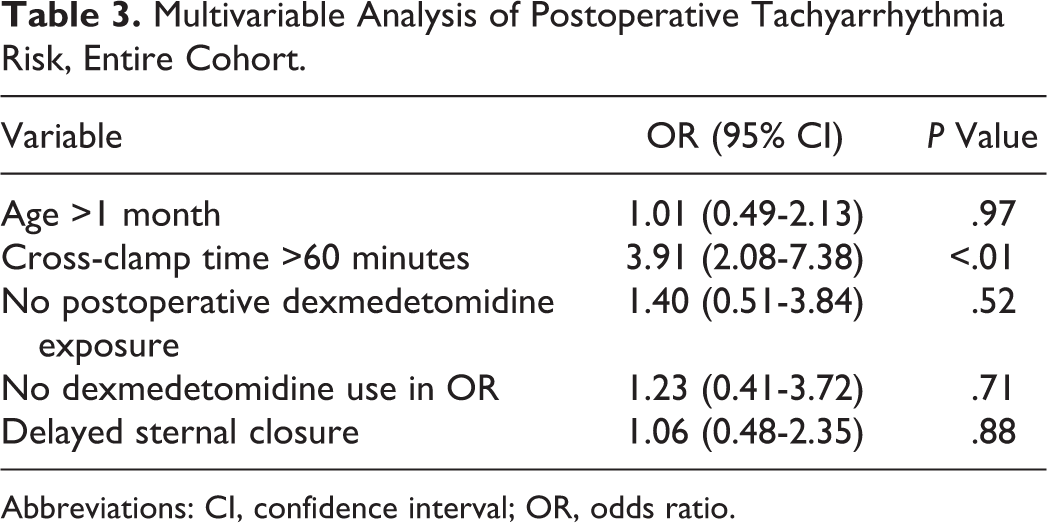
Abbreviations: CI, confidence interval; OR, odds ratio.
The incidences of arrhythmias for the three highest risk lesions are shown in Table 4, demonstrating a lower incidence of tachyarrhythmias in the high-risk DEX group. This lower incidence was primarily due to a reduction in junctional tachyarrhythmias (30% vs 10%, P = .02), which were the most common tachyarrhythmia. Among the high-risk patients, the only statistically significant baseline differences between the non-DEX and DEX groups was that the non-DEX group was less likely to receive dexmedetomidine in the operating room (15% vs 100%, P < .01) and more likely to have delayed sternal closure (69% vs 12%, P < .01). When adjusting for these variables along with age and cross-clamp time, the non-DEX group did not have significantly increased odds of tachyarrhythmia (Table 5). Multivariate analysis was not performed for the risk of bradycardia in this group due to the small number of patients.
Arrhythmia Incidence for High-Risk Lesions.
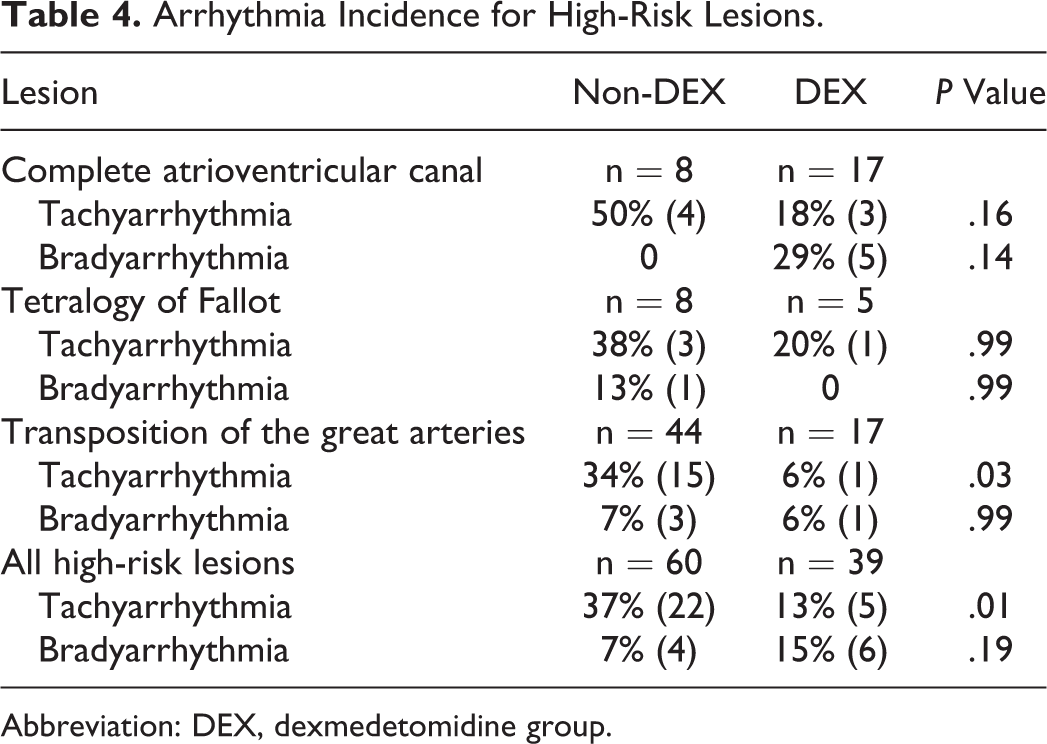
Abbreviation: DEX, dexmedetomidine group.
Multivariable Analysis of Postoperative Tachyarrhythmia Risk, High-Risk Group.
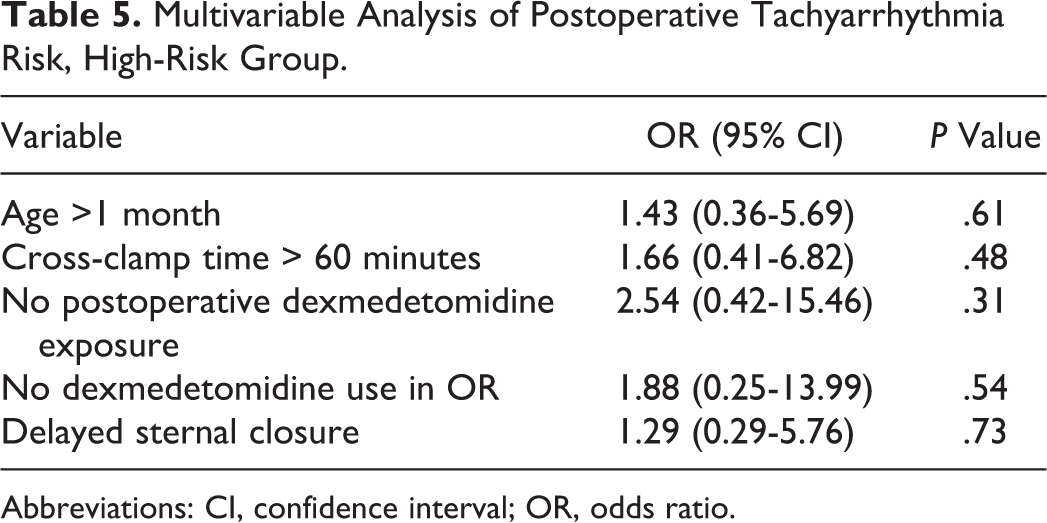
Abbreviations: CI, confidence interval; OR, odds ratio.
Other sedation use and secondary outcomes are shown in Table 6. Use of fentanyl and versed was significantly decreased in the DEX group. There was no difference in secondary outcomes of length of mechanical ventilation, length of hospital stay, or mortality for the entire cohort. For the high-risk patients, there were nonsignificant differences in length of mechanical ventilation (69 vs 44 hours, P = .05), hospital length of stay (12 vs 9 day, P = .12), and hospital mortality (7% vs 0%, P = .16) between the non-DEX and DEX groups, respectively.
Other Sedation Use and Patient Outcomes.a
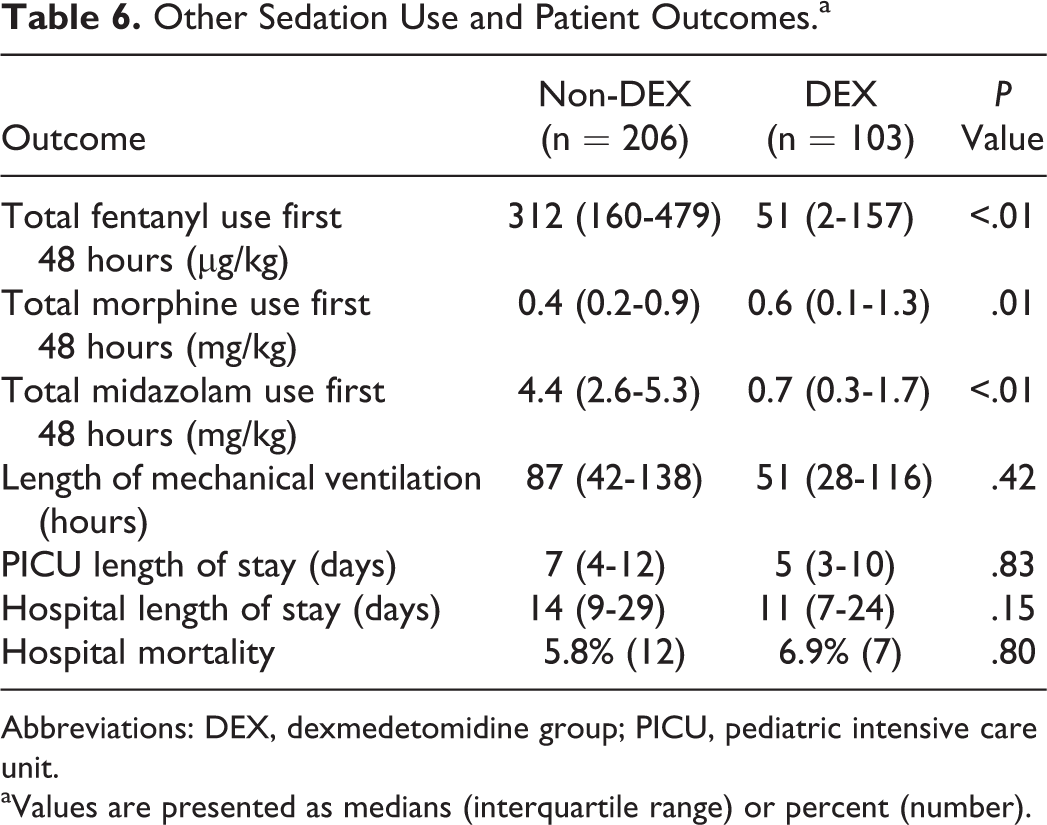
Abbreviations: DEX, dexmedetomidine group; PICU, pediatric intensive care unit.
aValues are presented as medians (interquartile range) or percent (number).
Comment
This retrospective study is the first to investigate the incidence of postoperative arrhythmias exclusively in young infants receiving dexmedetomidine for sedation. As infants are at higher risk for postoperative arrhythmias, our goal was to determine whether this subgroup of cardiac surgical patients would be more likely to benefit from dexmedetomidine’s heart rate lowering effect. While its use was not associated with a decreased risk of developing tachyarrhythmias, dexmedetomidine was associated with a decreased need for tachyarrhythmia treatment and less exposure to amiodarone. This suggests that those who did have tachyarrhythmias while on dexmedetomidine were more stable or had lower heart rates. Amiodarone has been associated with adverse effects and prolonged ICU stay in children receiving it for JET, 4 so less exposure may be clinically significant.
Postoperative arrhythmias continue to be common after heart surgery and can be associated with negative outcomes. 2 Multiple drugs have been studied for potential arrhythmia prophylaxis, but none has achieved widespread use in pediatrics. Beta-blockers are given to adults to prevent atrial fibrillation after heart surgery, 16 and amiodarone has been studied as a prophylactic agent in children. 17 but concerns about adverse effects remain. A pharmacologic agent that could safely lower arrhythmia risk could be embraced by critical care providers. Dexmedetomidine, with its favorable safety profile and widespread use in the ICU, has been suggested as that agent, but studies to date have shown mixed results.
Dexmedetomidine is approved for use in adults for short-term sedation in the ICU. Its use in the ICU is becoming more common due to growing concerns about the adverse effects of benzodiazepines, including prolongation of mechanical ventilation and ICU stay. 18 There is minimal respiratory depression with dexmedetomidine, making it an attractive sedative agent for children during ventilator weaning. Studies in pediatric cardiac patients have been encouraging and have reported few adverse effects. Lam et al reviewed the use of dexmedetomidine in critically ill children with cardiac disease and found that while there was a decrease in heart rate, the children maintained stability without the need for escalation in hemodynamic support and without adverse respiratory effects. 7 Chrysostomou et al specifically studied infants after cardiac surgery and found that dexmedetomidine provided adequate sedation with minimal effects on blood pressure and no respiratory depression. 19
Decreased heart rate is a commonly reported side effect of dexmedetomidine in children and adults. 7,20 –22 The mechanisms are incompletely understood. Dexmedetomidine has been found to decrease circulating epinephrine and norepinephrine though central sympatholysis 12 and may blunt the stress response to surgery. As several common postoperative arrhythmias in children are catecholamine sensitive, this effect could serve to reduce the risk of arrhythmias. Another proposed mechanism is increased parasympathetic tone by activation of α2-adrenergic receptors in the nuclei responsible for vagal neural activity. Kamibayashi et al found that while dexmedetomidine decreased induced arrhythmias in dogs, this benefit was absent when bilateral vagotomy was performed. 23 Increased vagal activity could explain the successful termination of reentrant tachycardia with dexmedetomidine. 24,25
Chrysostomou et al published the first study exploring the relationship between postoperative dexmedetomidine use and arrhythmias. 10 In this prospective observational study of 52 patients, the incidence of ventricular tachycardia decreased from 25% to 0% (P = .01) and supraventricular arrhythmias decreased from 25% to 6% (P = .05) in those receiving dexmedetomidine for sedation. While these results are intriguing, the incidence of ventricular tachycardia was significantly higher than what is typically seen in the PICU, suggesting other factors may have contributed to these results. The largest study to date was published by Shuplock et al and reviewed 1,593 patients undergoing surgery for congenital heart disease with 468 receiving dexmedetomidine. 11 After propensity score matching, there was no difference in tachyarrhythmias between groups (29 vs 31%, P = .66). They found an increased risk of bradyarrhythmias requiring intervention with dexmedetomidine use (OR: 2.18, 95% CI: 1.02-4.65). This study included all pediatric patients undergoing cardiac surgery.
Our study focused on infants less than six months of age as younger age increases the risk of postoperative tachyarrhythmias. 26 However, not all infants have similar baseline risk. For example, in our study, no patient undergoing an arterial–pulmonary shunt on bypass or the Glenn procedure had a tachyarrhythmia. These patients will not benefit from the potential antiarrhythmic effect of dexmedetomidine, but they still could experience the adverse effects of bradycardia.
Some studies have reported patients at high risk to benefit from dexmedetomidine. Kadam et al published a quasi-randomized controlled study of 94 children undergoing repair of tetralogy of Fallot, with the control group starting dexmedetomidine in the operating room and continuing postoperatively. The control group had an increased incidence of JET compared to those receiving dexmedetomidine (23% vs 8.5%), though there were no differences in secondary outcomes. 27 Another study by Gautam et al focused on 134 children undergoing ventricular septal defect repair. Dexmedetomidine use reduced the incidence of postoperative JET (OR: 0.17, 95% CI: 0.05-0.52). 28
In the present series, high-risk patients who received dexmedetomidine in the operating room were less likely to have postoperative tachyarrhythmias on univariate analysis, though this effect was no longer significant when accounting for postoperative dexmedetomidine exposure. The majority of patients who received postoperative dexmedetomidine also were exposed in the operating room, including all high-risk dexmedetomidine patients. As significant number of patients had arrhythmias on arrival to the ICU, starting a prophylactic medication in the operating room is logical and future randomized studies should focus on early dexmedetomidine exposure.
There are several limitations to our study. Because of the retrospective design, there are likely multiple confounders that cannot be fully accounted for. This design also would likely underestimate the true incidence of arrhythmias, though would likely capture most that were clinically significant or required treatment. Choice of sedation was tightly correlated with year of surgery as the sedation practices evolved over the study time frame from mostly benzodiazepines and narcotics to dexmedetomidine. No conclusions should be made in regard to whether dexmedetomidine use is associated with a decrease in narcotic and benzodiazepine exposure. There were other changes in practice, as evidenced by the difference in delayed sternal closure between groups, and these could have had an impact on the incidence of arrhythmias. Selection bias may also have played a role. As this was a retrospective study, use of dexmedetomidine was known to the care team and may have influenced the use of amiodarone or other antiarrhythmics in patients having tachyarrhythmias. Small sample size limits our ability to perform certain subgroup analysis and results in our study being underpowered for our primary outcome. We believe that this study is still valuable as it focuses on a high-risk population that has not previously been studied in detail and can inform future research. Our results suggest that a study focusing on high-risk infants with dexmedetomidine staring in the operating room would be most likely to yield clinically helpful results.
Conclusions
In this retrospective study, the use of dexmedetomidine for sedation after surgery for congenital heart disease was not associated with a decreased risk of tachyarrhythmias in young infants, supporting other recent studies concluding that dexmedetomidine does not have significant antiarrhythmic effect when used in the postoperative period. Dexmedetomidine use did reduce the need for treatment, which may be valuable.
Footnotes
Authors’ Note
All study procedures were performed at Children’s Mercy Hospital, Kansas City.
Acknowledgments
The authors would like to thank Amber Hughes-Schalk for her help with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Department of Pediatrics at Children’s Mercy Hospital.