
Abstract
Background:
Surgical repair of tetralogy of Fallot and major aortopulmonary collaterals (TOF/MAPCAs) involves unifocalization of MAPCAs and reconstruction of the pulmonary arterial circulation. Surgical and cardiopulmonary bypass (CPB) times are long and suture lines are extensive. Maintaining patency of the newly anastomosed vessels while achieving hemostasis is important, and assessment of transfusion practices is critical to successful outcomes.
Methods:
Clinical, surgical, and transfusion data in patients with TOF/MAPCAs repaired at our institution (2013-2018) were reviewed. Types and volumes of blood products used in the perioperative period, in addition to the use of antifibrinolytics and/or procoagulants (factor VIII inhibitor bypassing activity [FEIBA]; anti-inhibitor coagulant complex), were assessed. Outcome measures included days on mechanical ventilation (DOMV), postoperative intensive care unit and hospital length of stay (LoS), and incidence of thrombosis.
Results:
Perioperative transfusion data from 279 patients were analyzed. Surgical (879 ± 175 minutes vs 684 ± 257 minutes) and CPB times (376 ± 124 minutes vs 234 ± 122 minutes) were longer in patients who received FEIBA than those who did not. Although the indexed volume of packed red blood cells (128.4 ± 82.2 mL/kg) and fresh frozen plasma (64.2 ± 41.1 mL/kg) was similar in patients who did and did not receive FEIBA, the amounts of cryoprecipitate (5.5 ± 5.2 mL/kg vs 5.8 ± 4.8 mL/kg) and platelets (19.5 ± 20.7 mL/kg vs 20.8 ± 13 mL/kg) transfused were more in those who did receive FEIBA.
Conclusion:
Perioperative transfusion is an important component in the overall surgical and anesthetic management of patients with TOF/MAPCAs. The intraoperative use of FEIBA was not associated with a decrease in the amount of blood products transfused, DOMV, or LoS or with an increase in thrombotic complications.
Introduction
Unifocalization and reconstruction of the pulmonary circulation, incorporating all lung segments and addressing stenoses both proximal to and within the lung, is a central component of our management approach in patients with tetralogy of Fallot (TOF), pulmonary atresia, and major aortopulmonary collateral arteries (MAPCAs). 1 -4 These procedures involve extensive dissection of the pulmonary vasculature, followed by unifocalization of MAPCAs and pulmonary arteries (PAs) with multiple anastomoses and long suture lines. As such, anesthesia, surgical, and cardiopulmonary bypass (CPB) times are long. Consequently, these patients are at risk for both perioperative bleeding and pulmonary vascular thrombosis. 5,6 Thus, management of blood products is a critical aspect of intraoperative and perioperative care. Extensive blood loss and its replacement with blood products in order to achieve hemostasis is inevitable in patients undergoing unifocalization and repair of TOF/MAPCAs but has not been previously evaluated.
Transfusion of blood products has been associated with mortality and morbidity, including thrombotic complications and acute lung injury, in patients undergoing surgery for congenital heart disease. 7 -11 The use of antifibrinolytic agents in congenital cardiac surgery has been shown to improve coagulation test values. In observational studies, the ability to reduce blood loss and/or decrease blood product usage has been variable depending on the agent used. 12,13 The off-label use of procoagulant medications, such as anti-inhibitor coagulant complex (factor VIII inhibitor bypassing activity or FEIBA; package insert), 14 -16 is being used with increasing frequency, with the aims of reducing blood loss and transfusion. Although effective, these medications have been associated with thrombotic complications 17 -19 and have not been well studied in adult or congenital cardiac surgical patients. 20 -22
In this study, we sought to characterize our transfusion practice in patients with TOF/MAPCAs undergoing unifocalization and PA reconstruction. We also sought to characterize the impact of FEIBA on blood product transfusion and postoperative outcomes.
Methods
Patients
After Stanford University institutional review committee approval, we reviewed the records of patients who underwent complete repair of TOF/MAPCAs at Lucile Packard Children’s Hospital between 2013 and 2018. Complete repair was defined as unifocalization and PA reconstruction, establishment of a right vein-to-PA connection, and closure of the ventricular septal defect. Surgical management of TOF/MAPCAs at our center has been described in detail in prior reports. 5 -8 Although more than 650 patients with TOF/MAPCAs have undergone surgery at our center over the past 18 years, we limited our investigation to the most recent five years. This was an effort to limit the number of confounding variables associated with the development of the program over time. Demographic and diagnostic data collected included age and weight at repair, sex, and genetic abnormalities (chromosome 22q11 deletion, Alagille syndrome). Intraoperative data included surgical, CPB, and aortic cross-clamp times. Procedures not requiring CPB were excluded from analysis. Patients who underwent extracorporeal membrane oxygenation (ECMO) in the perioperative period were included in a separate analysis.
Cardiopulmonary Bypass Strategy
Our pump prime volume is weight based, as follows: 0 to 10 kg: 300 cc, 10 to 35 kg: 600 cc, 35 to 50 kg: 800 cc, 50 to 70 kg: 1,000 cc, and 70+ kg: 1,200 cc. We use a clear prime if the calculated dilutional hematocrit value is ≥30%. Otherwise, we use a blood prime consisting of red blood cell, fresh frozen plasma (FFP), 25% albumin (as well as heparin, bicarbonate, mannitol, steroids, calcium, and tranexamic acid for these patients). The amounts of packed red blood cell (PRBC), FFP, and albumin depend on the patient and circuit size. For our small circuit, utilized in patients <10 kg, we use 200 cc PRBC and 60 cc FFP. The goal during separation from CPB is to achieve a hematocrit of 40% to 45% prior to separation.
Blood Product Utilization
For this study, blood products evaluated included PRBCs, FFP, platelets (PLTs), and cryoprecipitate (CRYO). The types and amounts of blood products used intraoperatively and in the initial 24-hour postoperative period were determined from the electronic medical record. Blood products administered were documented in our institutional Society of Thoracic Surgeons (STS) database and confirmed via the surgeon’s operative note, electronic anesthetic record, and electronic transfusion services record. Blood products were documented in units, from which total mL and mL/kg were calculated. Our institution offers volume-reduced/plasma-free PLTs, which are used in patients weighing less than 10 kg. For this reason, we standardized our data to volume units, mL/kg, rather than units of product administered. The use of antifibrinolytic agents and the dosing of FEIBA, if given, were determined from the electronic anesthesia record. At our institution, transexemic acid is given according to the Boston Children’s Hospital dosing protocol. 23 Factor VIII inhibitor bypassing activity, if dosed, is at 10 U/kg, 24 with the initial dose usually being given after approximately 10 mL/kg of blood product has been administered. Though a firm protocol has not been established, an additional one to two doses are administered if warranted by clinical circumstances, that is, continued bleeding.
Data Analysis
Data were collected and maintained in institutional database of patients with TOF/MAPCAs treated at our institution. Baseline characteristics of the study participants were summarized using descriptive statistics. Normally distributed continuous variables were expressed as mean ± standard deviation. Non-normally distributed variables were expressed as median (25th-75th percentile). Categorical variables were expressed as number (%). Univariable comparison of differences between groups was performed with Student t test, Mann-Whitney U test, and χ2 or Fisher exact test. To account for differences between study groups, we computed propensity scores from a logistic regression model including all baseline characteristics, such as age, gender, genetic syndrome, weight, and times. A weighted approach, inverse probability weighting (IPWT), calculated from the propensity score (surgical and CPB times, riastap, antifibrinolytic, and chromosome 22q11 deletion), was then used to assess intergroup differences. To account for the potential confounding effect of including patients who went on ECMO, we also analyzed transfusion data in the cohort of patients who did not receive ECMO. A two-sided P value of .05 was considered statistically significant. All analyses were performed with SAS software, version 9.4 (SAS Institute Inc, Cary, North Carolina).
Results
Patients
We identified 279 patients who underwent complete repair of TOF/MAPCAs during the study period, of which 12 underwent perioperative ECMO. Of the 279 patients, 105 (37%) received FEIBA intraoperatively and 174 (62%) did not (Table 1). On unadjusted analysis, there were no differences between FEIBA groups in demographic or basic diagnostic features. Patients with Alagille syndrome comprised approximately 5% of the cohort and patients with a chromosome 22q11 deletion approximately 30%.
Demographic and Operative Details for All Patients and According to FEIBA Use.a
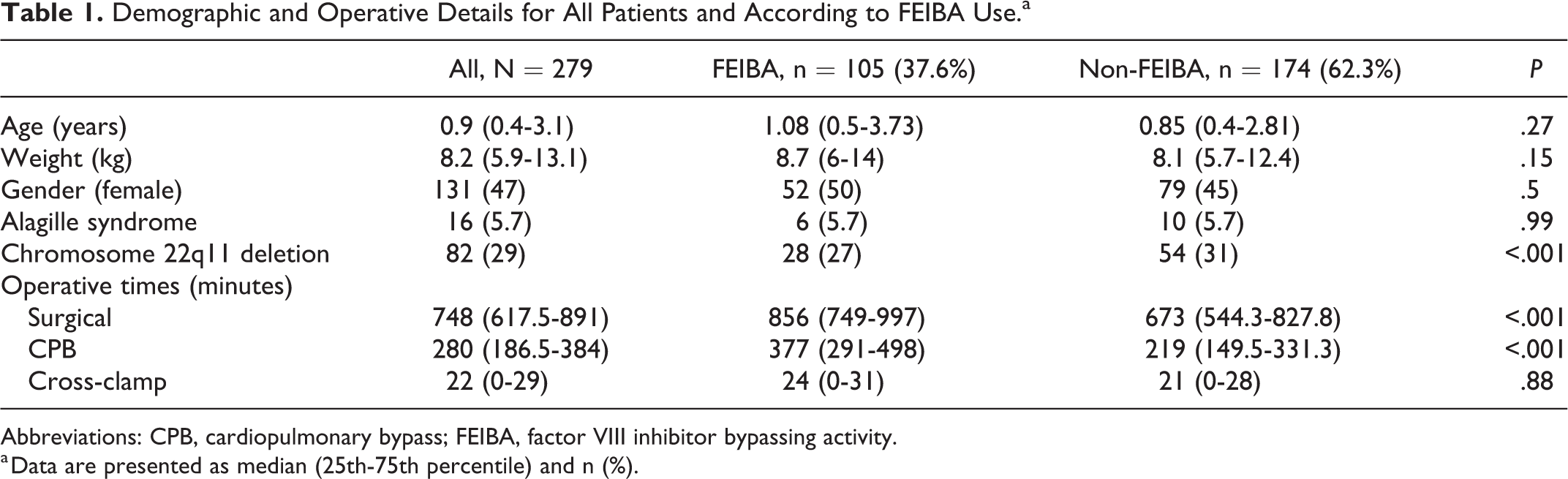
Abbreviations: CPB, cardiopulmonary bypass; FEIBA, factor VIII inhibitor bypassing activity.
a Data are presented as median (25th-75th percentile) and n (%).
Surgical
Surgical duration was 757 ± 248 minutes and was longer in the FEIBA group (879 ± 175 minutes) than the non-FEIBA group (684 ± 257 minutes; Table 1). Similarly, CPB time was 288 ± 141 minutes and was longer in the FEIBA (376 ± 124 minutes) than the non-FEIBA group (234 ± 122 minutes).
Blood Product Transfusion
Intraoperative
Perioperative transfusion data are summarized in Table 2. Most patients (n = 250; 90%) received transexemic acid. Most patients (94%) received PRBCs, FFP, and PLTs, and the majority (∼83%) received CRYO. The proportion of patients receiving PRBC, FFP, and PLT transfusions was similar between the FEIBA and non-FEIBA groups; however, a larger proportion of patients in the FEIBA group received CRYO than in the non-FEIBA group. There was no difference in intraoperative PRBCs or FFP transfusion volumes (indexed to weight) between FEIBA and non-FEIBA groups, both on unadjusted and IPWT-adjusted analysis. However, indexed CRYO and PLT volumes administered were larger in the FEIBA group on unadjusted and adjusted analysis (Table 3).
Perioperative Transfusion and Outcomes Data.a,b,c
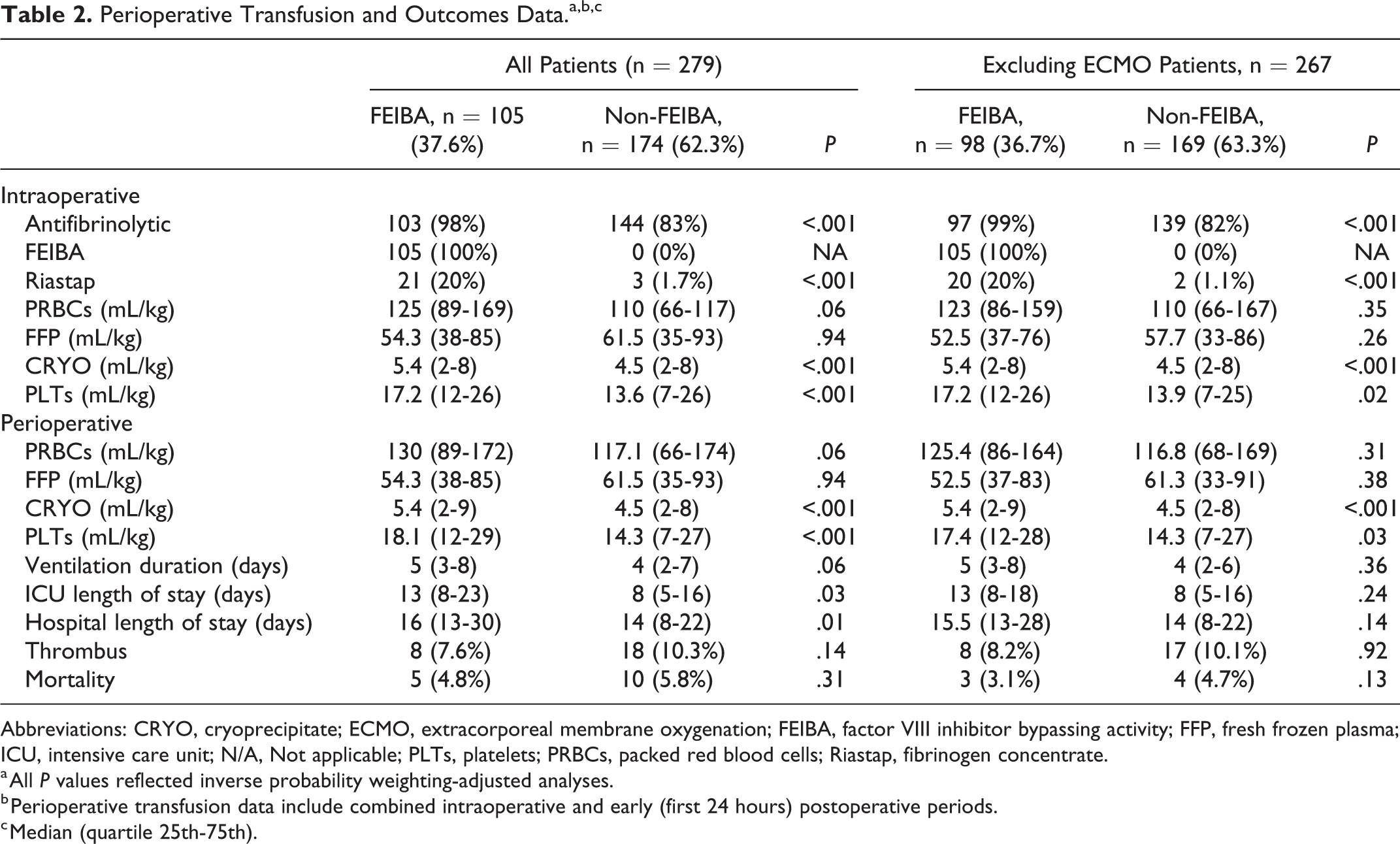
Abbreviations: CRYO, cryoprecipitate; ECMO, extracorporeal membrane oxygenation; FEIBA, factor VIII inhibitor bypassing activity; FFP, fresh frozen plasma; ICU, intensive care unit; N/A, Not applicable; PLTs, platelets; PRBCs, packed red blood cells; Riastap, fibrinogen concentrate.
a All P values reflected inverse probability weighting-adjusted analyses.
b Perioperative transfusion data include combined intraoperative and early (first 24 hours) postoperative periods.
c Median (quartile 25th-75th).
Demographic, Operative, and Outcome Data for the Alagille and Non-Alagille Cohorts.a
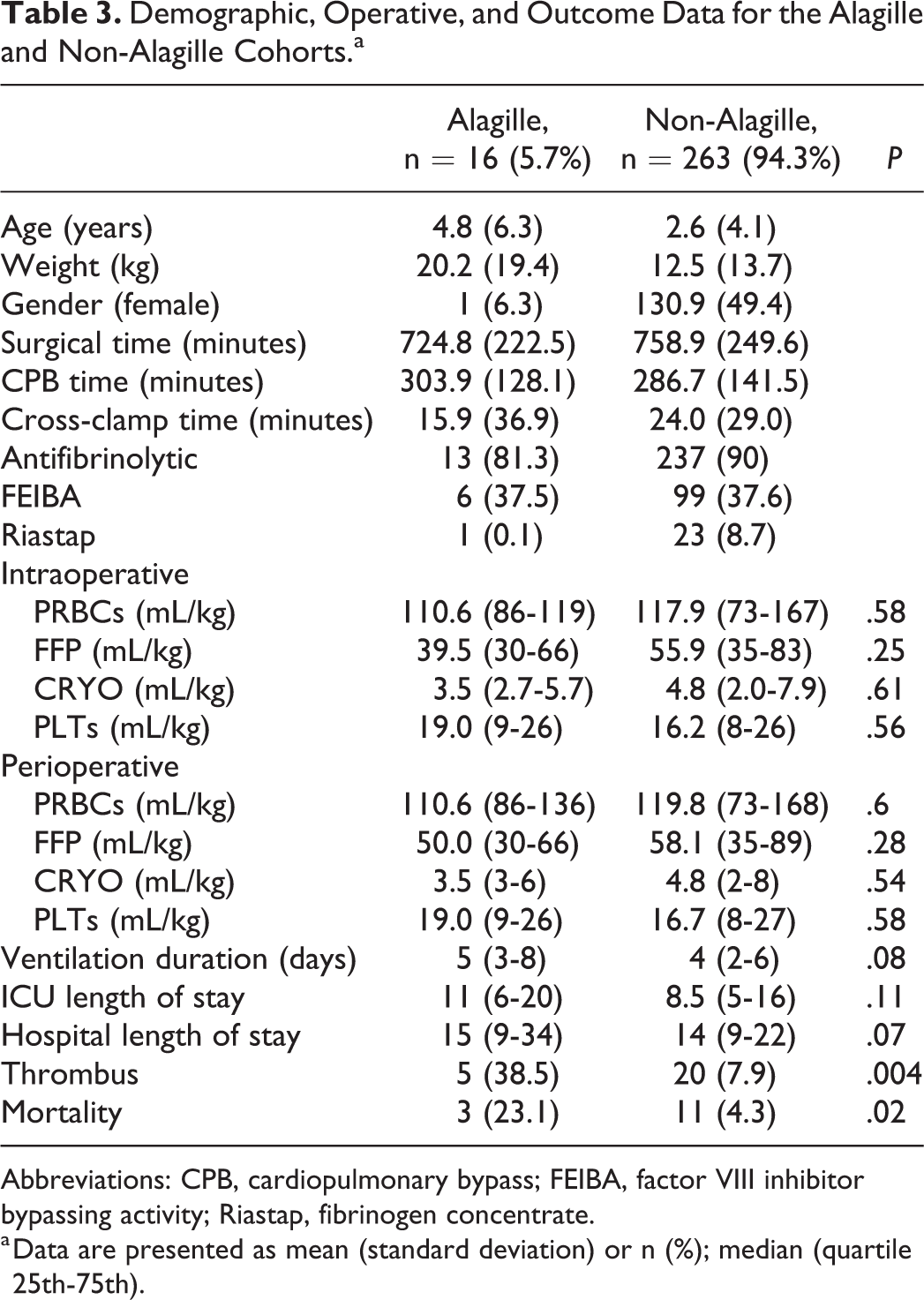
Abbreviations: CPB, cardiopulmonary bypass; FEIBA, factor VIII inhibitor bypassing activity; Riastap, fibrinogen concentrate.
a Data are presented as mean (standard deviation) or n (%); median (quartile 25th-75th).
Postoperative (initial 24 hours)
The proportion of patients who received postoperative PRBCs, FFP, PLTs, and CRYO did not differ statistically between FEIBA and non-FEIBA groups, either on unadjusted or adjusted analysis (Table 3).
Perioperative (intraoperative and perioperative)
In the perioperative period, overall, the total indexed volumes of PRBCs and FFP did not differ between FEIBA and non-FEIBA groups (Table 2). However, larger total indexed volumes of PLT and CRYO were administered to patients who received FEIBA (Table 2).
Extracorporeal Membrane Oxygenation
Twelve patients went on ECMO either directly in the operating room or within 24 hours of transfer to the cardiovascular intensive care unit (ICU; Table 2). Patients who received FEIBA were more likely to be supported with ECMO on unadjusted analysis (6.7% vs 2.9%, P = .007). There were no differences in demographics or disease characteristics between the groups whether or not ECMO patients were included in the analyses. Similarly, there were no differences in anesthesia, surgery, cross-clamp, or CPB times whether or not ECMO patients were included in the analyses. Despite exclusion of ECMO patients in the data, statistical differences in CRYO administration between FEIBA and non-FEIBA groups remained. The use of ECMO was associated with the perioperative administration of PRBCs and PLTs (Table 2).
Durations of mechanical ventilation, ICU length of stay (LoS), and hospital LoS were longer in patients who received FEIBA on both unadjusted and adjusted analyses, both with and without exclusion of patients who went on ECMO (Table 2). There was no difference in the incidence of thrombus or mortality between FEIBA and non-FEIBA groups, either on unadjusted or adjusted analysis.
Genetic Syndromes
Alagille syndrome
Of the 279 patients, 5.7% were documented to have Alagille syndrome (Table 3). These patients were older and weighed more. Most (94%) patients with Alagille syndrome were male. The surgical, CPB, and aortic cross-clamp times were similar in patients with and without Alagille syndrome. Most patients received antifibrinolytic (81%), but only 38% received FEIBA. Indexed volumes of PRBCs and CRYO were similar between patients with and without Alagille syndrome. However, less FFP and more PLT were given in patients with Alagille syndrome than those without. Patients with Alagille syndrome did have a higher incidence of thrombus (P = .004) and mortality (P = .02; Table 3).
Chromosome 22q11 deletion
Eighty-two (29%) patients had a chromosome 22q11 deletion and were similar to their non-22q11 deletion counterparts in terms of age, weight, gender, and intraoperative times. There were no differences noted in terms of amount of blood products administered, or use of FEIBA or antifibrinolytic, in patients with a chromosome 22q11deletion.
Comment
In this study, we documented our transfusion practice in a large series of patients who underwent complete repair of TOF/MAPCAs. Although this study represents a single-center institutional experience/practice in the surgical repair TOF/MAPCAs, it demonstrates the considerable amount of blood products transfused during these procedures that involve extensive dissection and multiple suture lines and the potential impact on outcome. Factor VIII inhibitor bypassing activity was implemented into our practice empirically, with the expectation that it would reduce bleeding risk and blood product utilization. However, in this high-risk patient population, we did not observe any appreciable difference in product related or other outcomes, although there were potentially confounding factors that are discussed below.
Though a retrospective study, the design represents a change in practice over time. Appreciating the extent of revascularization in these procedures, and the need for maintaining patency of the newly anastomosed vessels, an understanding for the potential for bleeding due to extensive suture lines is inherent. At our institution, the use of an antifibrinolytic agent in these patients began in 2013 and became a well-established practice by 2014. Amicar was the antifibrinolytic used until September 2017, but it was replaced with tranexamic acid due to lack of availability. The use of FEIBA was first introduced in our surgical transplant population 24 and later introduced to our TOF/MAPCAs population in late 2014.
The change in practice, the use of antifibrinolytic agents and FEIBA, was motivated in part by a better understanding of postoperative outcomes in these patients. 25 Reperfusion pulmonary edema was a recognized issue in 50% of postsurgical patients with TOF/MAPCAS, although it did not explain prolonged respiratory failure and the need for prolonged mechanical ventilation in these patients. 26 An initial hypothesis for the prolonged respiratory insufficiency observed was transfusion-related lung injury, which was consistent with the significant amount of blood product administration in these patients. Thus, practices to limit perioperative blood product administration seemed prudent. 27,28 However, as our program continued to grow, with expanding national and international referrals, the complexity of patients referred to our center also increased over the past several years, potentially confounding our assessment of bleeding, transfusion, and other outcomes.
It is possible that transfusion and bleeding outcomes may be impacted by underlying genetic factors. For example, Alagille syndrome is associated with a tendency toward bleeding related to a vasculopathy caused by a mutation in the JAG1 gene. 29,30 We have previously observed that patients with TOF/MAPCAs and Alagille syndrome are among the most complex and often have worse outcomes. 1 However, bleeding- and transfusion-related outcomes have not been evaluated. Although liver disease is common in patients with Alagille syndrome, the PLT count and prothrombin times are usually normal. 30 In our study, Alagille syndrome was associated with mortality and thrombosis, but not with an increased transfusion of blood products, although the number of patients was small. Large PLTs and thrombocytopenia have been associated with the chromosome 22q11 deletion syndrome. 31 -33 Platelet dysfunction as a result of PLT glycoprotein abnormalities and a tendency for bleeding has been described in patients with chromosome 22q11 deletion undergoing surgical repair of congenital heart disease. 32,33 In this current cohort, however, we did not observe any difference in transfusion or perioperative outcomes.
In reviewing the STS and Congenital Cardiac Anesthesia Society database, blood product administration is related to both age and surgical complexity. 34 Not surprisingly, the amount of blood products administered in this current cohort of extremely complex patients, in whom operative, anesthesia, and bypass times were very long, approximates an exchange of approximately three blood volumes.
Although we did not observe any difference in postoperative transfusion outcomes between FEIBA and non-FEIBA cohorts, it is possible that FEIBA conferred benefits that were not detectable in the outcomes we analyzed, such as quicker or more straightforward hemostasis and fewer exploratory procedures for bleeding. Due to a combination of factors, comparison of FEIBA and non-FEIBA cohorts was likely confounded. In particular, we introduced FEIBA into our practice relatively recently and have started using it more frequently in the past few years. Thus, there may have been an era effect in outcomes, particularly as our growing experience and expanding referral base has likely engendered a higher risk population and more extensive operations.
In an effort to mitigate such confounding, we performed IPWT adjustment, but there may have been residual confounding. Also, patients who were supported with ECMO from the operating room or in the early postoperative period received more products. Extracorporeal membrane oxygenation was more commonly employed in the FEIBA cohort, which may be due to chance or related to the increasingly complex population we treat. To account for this potential source of bias, we analyzed patients both including and excluding the subset who received ECMO, with no notable difference in findings. An additional potential confounder was the slight imbalance of antifibrinolytic use between groups and the transition from Amicar to tranexamic acid at a particular point in time, although there is no reason to believe these factors had a major impact on outcomes. The use of antifibrinolytics in pediatric cardiac surgery is well established 12,13 and a previous institutional comparison of Amicar and tranexamic acid in adult cardiac surgical patients showed equivalent red cell transfusion and postoperative bleeding. 35
Factor VIII inhibitor bypassing activity is a four-factor procoagulant complex that contains inactivated factors II, IX, and X and activated factor VII. The use of FEIBA in pediatric patients for bleeding diathesis such as hemophilia has been described; however, there are insufficient data for its use in children under the age of 6 years. Dosing in this subset of pediatric patients is 100 U/kg/d and not to exceed 200 U/kg/d (package insert). 14 Our dosing regimen is 10 to 15 U/kg, 24 and based on our investigation, 2 ± 1 intraoperative doses were administered after protamine and PLTs were administered. We cannot comment on the potential benefit or risk of other dosing regimens.
Thrombotic complications (8.2/100,000 infusions) are a concern with the administration of procoagulants such as FEIBA and are vascular (myocardial infarction, pulmonary embolus, stroke). 18,19 The use of FEIBA in cardiac surgery has been described in adults 20 ; however, the number of institutions using procoagulants in pediatric cardiac surgery is limited and FEIBA use represents a very small percentage of overall procoagulant use. 36,37 Congenital heart disease and indwelling catheters are risk factors for thrombosis in pediatric patients. 38,39 An 11% overall incidence of thrombotic complications has been described in pediatric cardiac surgery patients. 39 Twenty-six (9.3%) patients in our investigation had thrombotic complications, but there was no association with FEIBA (P = .31).
Our PRBC transfusion practice in patients with TOF/MAPCAs is similar to that described by Cholette et al from the pediatric critical care transfusion and anemia expertise initiative. 40 Although intraoperative monitoring of coagulation parameters has been useful in guiding perioperative transfusion of coagulation factors such as PLTs, FFP, and CRYO, our experience in over 500 patients with TOF/MAPCAs has empirically guided our transfusion practice. Though not yet standardized or guided by intraoperative coagulation studies, the need for postoperative transfusion in these patients is limited, as demonstrated by comparing intraoperative to overall perioperative transfusion of blood products. Postoperative transfusion of any blood product occurred in only 30 (11%) of our patients, 12 of whom received products while supported with perioperative ECMO.
In summary, in our experience, transfusion of a large amount of blood products is inevitable during surgical unifocalization and repair of TOF/MAPCAS. Despite the addition of antifibrinolytics and the use of procoagulants, such as FEIBA, we were unable to reduce the amount of blood product transfusion or improve outcomes. Although we accounted for the increased complexity of our surgical cases using IPWT adjustment and accounted for the tendency toward ECMO in the more complex cases, complexity may not be completely reflected in surgical and CPB duration. An appropriate prospective controlled study, with laboratory confirmation using thromboelastography, may be necessary to clarify this issue convincingly.
Footnotes
Authors’ Note
All research was approved by the institutional review board of Stanford University. The authors had full control of the design of the study, methods used, outcome parameters, analysis of data, and production of the written report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant support from The Gerber Foundation.