
Abstract
Levoatriocardinal vein without left-sided valvular atresia is rare. We hereby present an image of the levoatriocardinal vein in a patient with multiple muscular ventricular septal defect with small atrial septal defect and mitral regurgitation.
A nine-month-old female child was admitted with complaints of recurrent respiratory tract infection. Echocardiography showed a mid-muscular ventricular septal defect (VSD) and moderate eccentric mitral regurgitation (Figure 1A and B). Echocardiography also showed a connecting vein from the left atrium (LA) to the left brachiocephalic vein (LBCV) with anomalous connection of the left upper pulmonary vein (LUPV) to the left-sided connecting vein with left-to-right shunt (Figure 1 C). For further delineation, contrast-enhanced computed tomography was performed, which confirmed the presence of a levoatriocardinal vein with partial anomalous pulmonary venous connection (PAPVC) of the LUPV. Also shown are two muscular VSDs and a small patent foramen ovale (Figure 2).
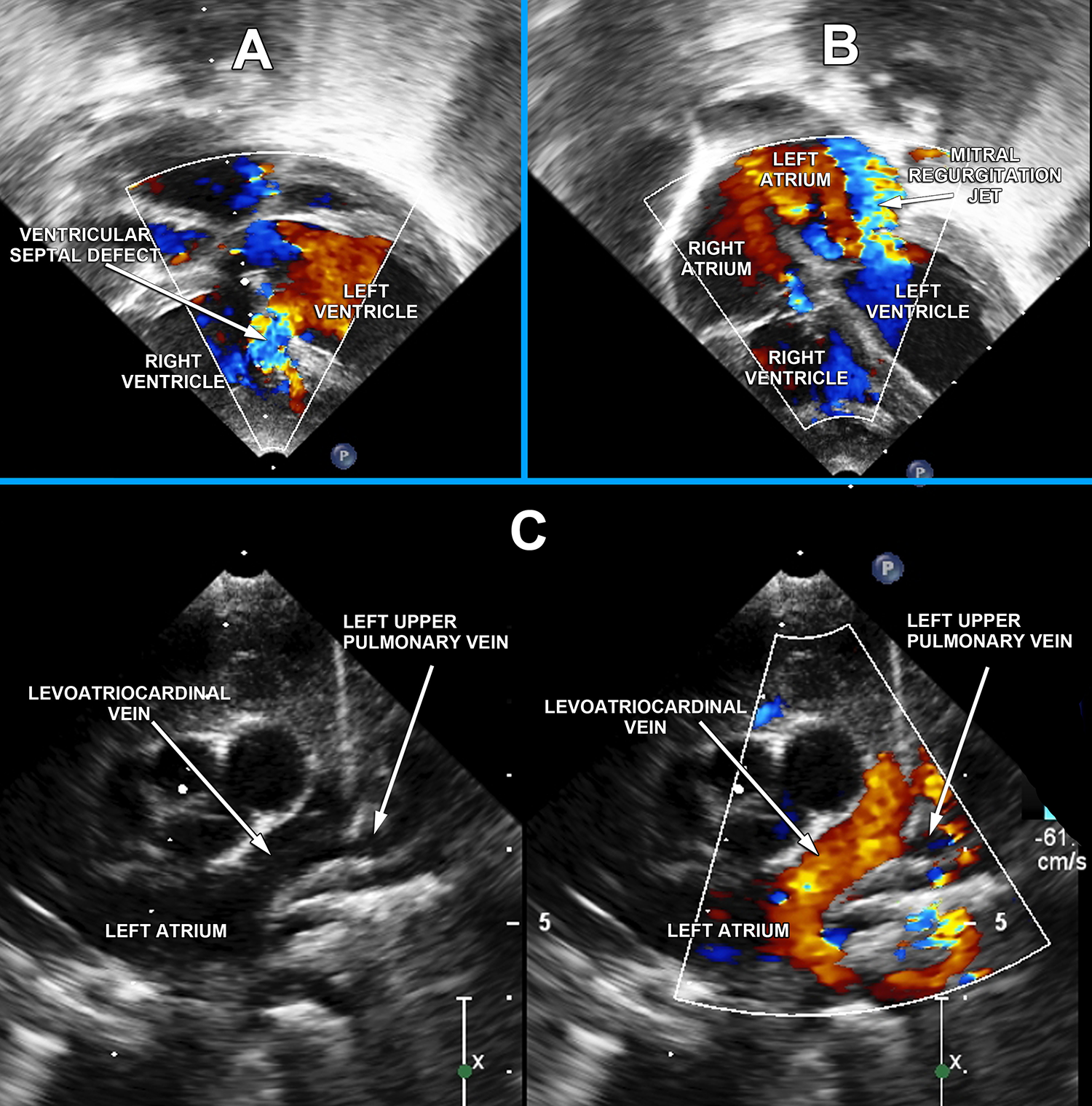
Two-dimensional echocardiography showing (A) mid-muscular ventricular septal defect with left-to-right shunt, (B) moderate eccentric mitral regurgitation, and (C) a connecting vein from the left atrium to the left brachiocephalic vein with left-to-right shunt and anomalous connection of the left upper pulmonary vein into the connecting vein.
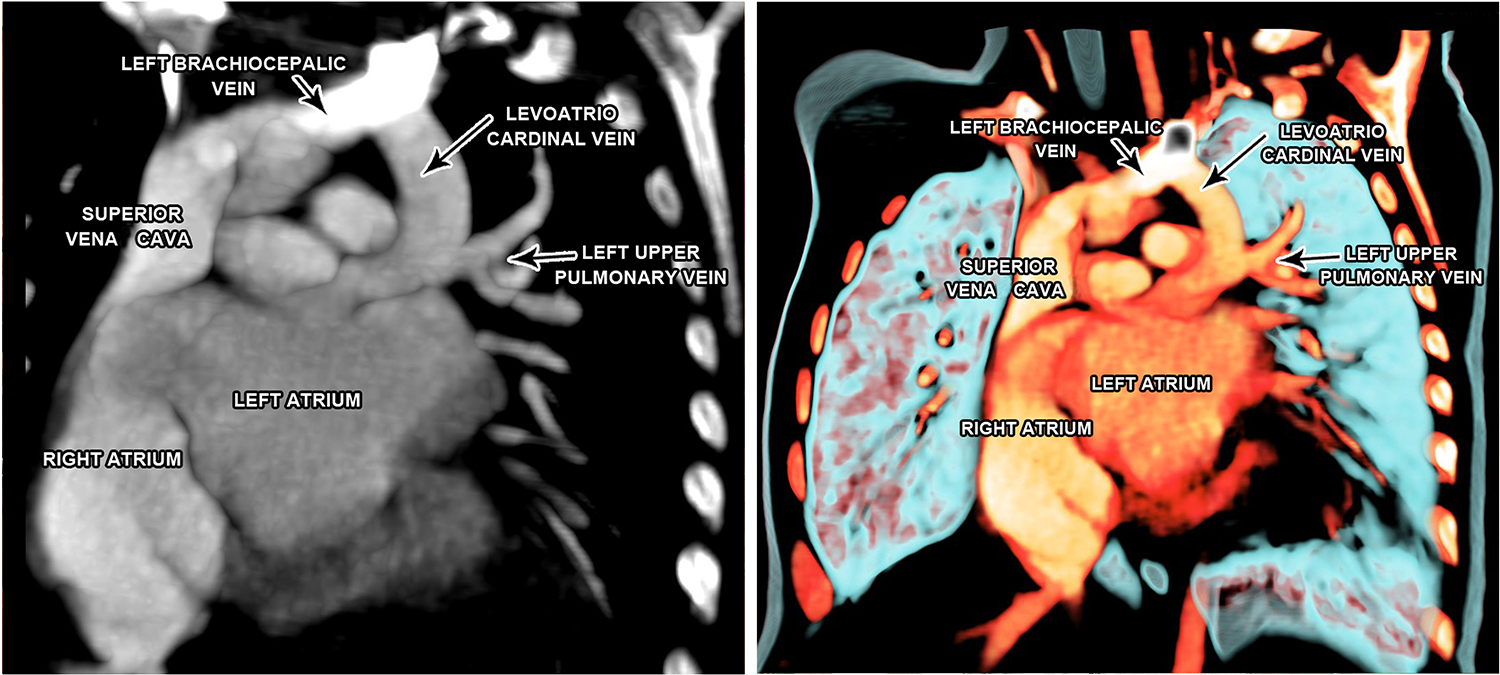
Contrast computed tomography angiography showing the levoatriocardinal vein with anomalous connection of the left upper pulmonary vein into the levoatriocardinal vein.
The patient underwent surgical repair by midline sternotomy with mild hypothermic cardiopulmonary bypass using aortic and bicaval cannulation. Intraoperatively, the levoatriocardinal vein was seen to be located at the usual site of a left-sided vertical vein, as seen in PAPVC. The levoatriocardinal vein was dissected extrapleurally and extrapericardially and was looped at the junction with the LBCV (Figure 3). The levoatriocardinal vein opened into the roof of the LA just lateral to the atrial appendage without any apparent narrowing. The LUPV opening into the levoatriocardinal was also without narrowing. Ligation of the levoatriocardinal vein just before insertion into the LBCV was performed. The VSDs were then closed with two polytetrafluoroethylene patches. The mitral annulus appeared to be dilated. Appearance of the leaflets and subvalvular apparatus were normal. Accordingly, mitral posterior commissural suture annuloplasty was performed to reduce mitral regurgitation. The patient had an uneventful recovery without any residual defects seen on echocardiography.
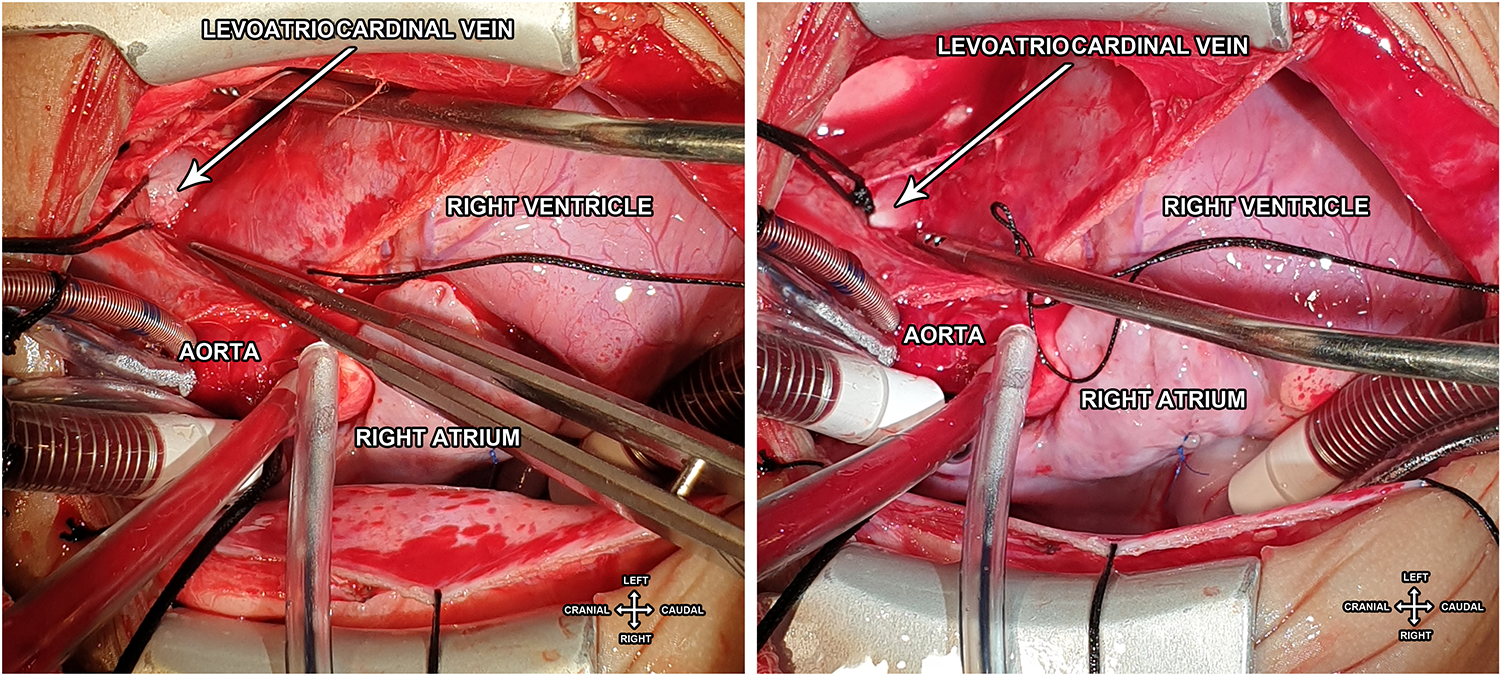
Intraoperative photograph showing the levoatriocardinal vein connected to the left atrium, ascending vertically extrapleurally and extra pericardially and connecting to the left brachiocephalic vein.
The levoatriocardinal vein is seen in patients with obstructive lesions of the left side of the heart such as hypoplastic left heart or mitral atresia associated with an intact or significantly restrictive atrial septum. 1 In such cases, the levoatriocardinal vein acts as a decompressing vessel for pulmonary venous return.
Although instances of the levoatriocardinal vein in association with well-developed left heart without any obstructive lesions have been reported, 2 concomitant presence of VSD and mitral regurgitation are unique aspects of our case.
Footnotes
Authors’ Statement
The patient’s parents consented to the submission and publication of this report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.