
Abstract
Background:
The optimal surgical management of patients with transposition of the great arteries (TGA), ventricular septal defect (VSD), and left ventricular outflow tract obstruction (LVOTO) is debatable. This is our initial experience with pulmonary root translocation (PRT), a technique that aims to preserve the pulmonary valve function.
Methods:
From July 2012 to October 2019, 16 patients underwent anatomical repair for TGA, VSD, and LVOTO. The median age was 12 months (range: 7 months to 13 years), and the median weight was 7.75 kg (range: 5.6-29.5 kg). Thirteen patients had a diagnosis of d-TGA and three had congenitally corrected transposition of the great arteries (cc-TGA). The surgical technique involved PRT from the left ventricle (LV) to the right ventricle and routing the LV to the aorta. The left ventricular outflow tract orifice resulting from the pulmonary root extraction was closed with a pericardial patch. In patients with cc-TGA, an atrial switch operation was added. A bidirectional Glenn was necessary in four patients with a long LV to aorta tunnel. One patient required a transannular patch to reconstruct the right ventricular outflow tract (RVOT).
Results:
The median follow-up was 27 months. There was one hospital death due to residual mitral regurgitation. One patient died at home four months after hospital discharge. The remaining patients are doing well with adequate RVOT function and no valve regurgitation.
Conclusions:
Complete correction of TGA, VSD, and LVOTO using PRT was achieved with acceptable risk in patients with pliable and nondysplastic pulmonary valve. The translocated pulmonary root performed well in this short follow-up.
Keywords
Introduction
The ideal surgical treatment for transposition of the great arteries (TGA) with ventricular septal defect (VSD) and left ventricular outflow tract obstruction (LVOTO) has always been a matter of debate among surgeons across the world. Early surgical techniques of anatomical repair of this defect included the Rastelli operation 1 and the LeCompte procedure. 2 Aortic root translocation (Bex-Nikaidoh procedure) was introduced by Bex et al in 1980 3 and was later popularized by Nikaidoh in 1984. 4 The same surgical concept of the Nikaidoh procedure has been extended to the repair of double outlet right ventricle (RV) and congenitally corrected transposition of the great artery (cc-TGA) with VSD and LVOTO. 5
In contrast to the posterior translocation of the aortic root in Nikaidoh procedure, Da Silva et al from Brazil introduced pulmonary root translocation (PRT) as surgical treatment for this defect. 6 In this procedure, the pulmonary root is harvested from the posteriorly placed left ventricular outflow tract (LVOT) and translocated anteriorly to the RV without doing a LeCompte maneuver and bringing the pulmonary root to the left of the aorta. The aim of this surgical technique has been to overcome the limitations of the earlier procedures which included the absence of a competent pulmonary valve in the right ventricular outflow tract (RVOT), requirement of a conduit in the RVOT position, and more importantly avoiding incising and mobilizing the aorta and handling the coronary arteries. 5,7 Describing their initial experience with this technique, Da Silva et al documented growth of the RVOT in patients during follow-up. 7 The concept of the PRT was extended by the same group as part of the double switch operation in cc-TGA with VSD and LVOTO. 8,9 We present our early experience with the surgical technique of PRT in the setting of TGA with VSD and LVOTO.
Patients and Methods
From July 2012 to October 2019, 16 patients underwent anatomical repair for TGA with VSD and LVOTO. The age ranged from 7 months to 13 years (median: 12 months). There are eight males and eight females. The weight ranged from 5.6 to 29.5 kg (median: 7.75 kg). Table 1 describes the clinical profile of the patients. All the patients presented with cyanosis and failure to thrive. The hematocrit ranged from 42% to 60% (median: 44%).
Patient Demographics Including Date of Surgery, Age, Weight, Diagnosis, and Operative Procedure Details.
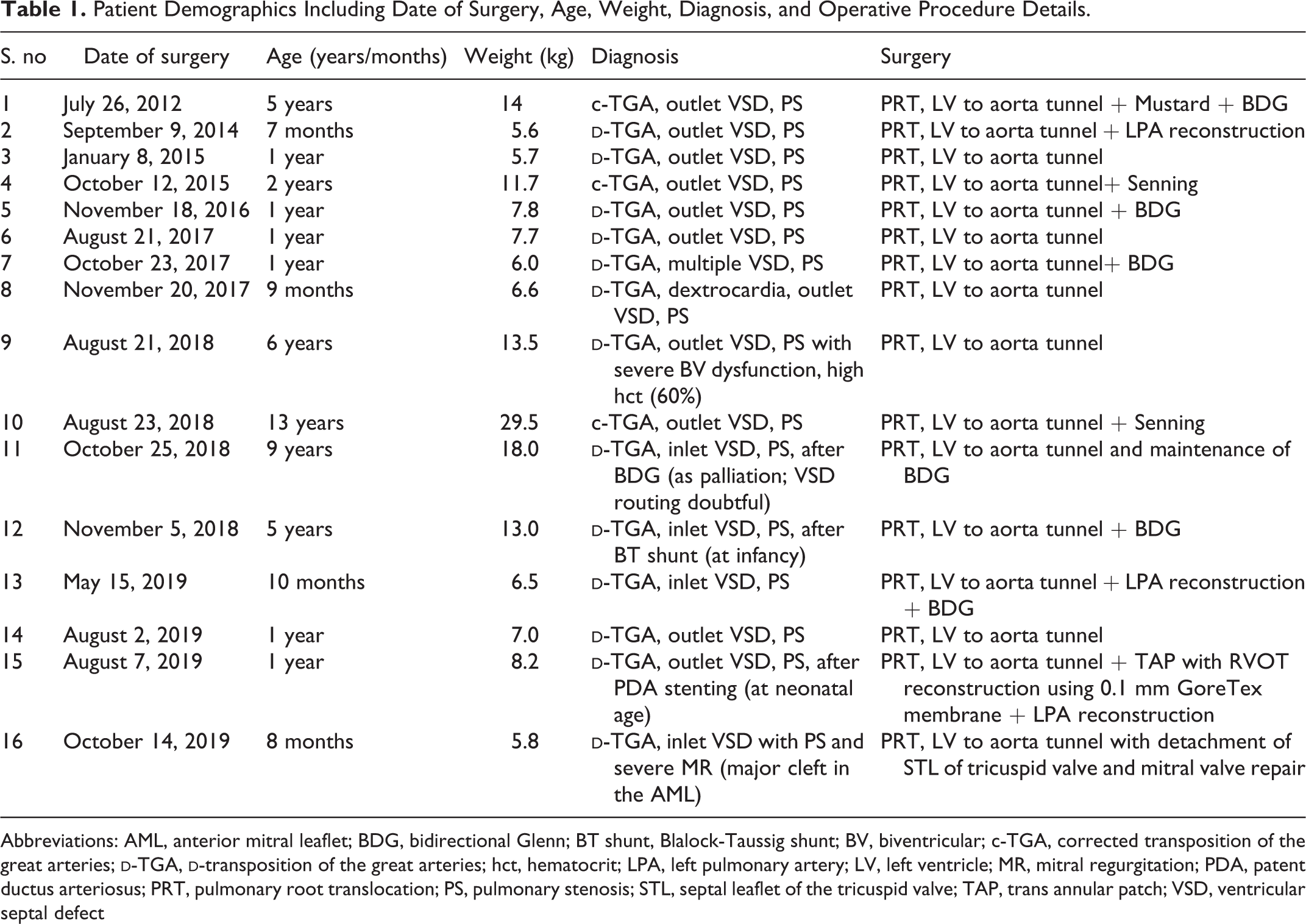
Abbreviations: AML, anterior mitral leaflet; BDG, bidirectional Glenn; BT shunt, Blalock-Taussig shunt; BV, biventricular; c-TGA, corrected transposition of the great arteries;
Informed consent for the operative procedure, including the surgical technique of PRT, was obtained from the parent(s) or guardian of each patient. In addition, a retrospective review of the data for purposes of this study was approved by the institutional review board (IRB) and permission was granted by the IRB for publication of the report.
Preoperative z Score and the Left Ventricular Outflow Tract Obstruction
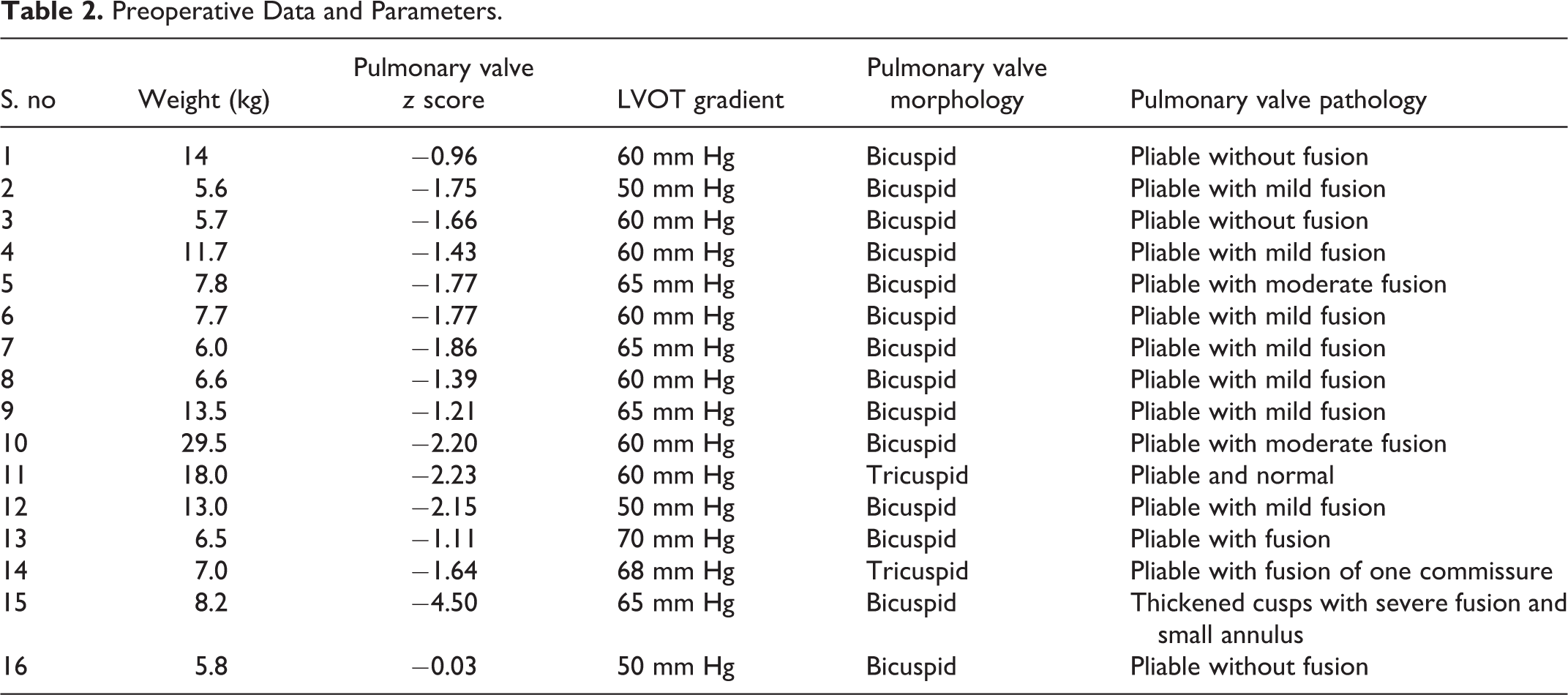
Table 2 shows the preoperative parameters that include the pulmonary valve z score, LVOT gradient, and the morphology and pathology of the pulmonary valve. In all patients, the LVOTO was subvalvular consisting of dense fibromuscular tissue.
Preoperative Data and Parameters.
Operative Technique
The great arteries were dissected as completely as possible to mobilize both the roots before the commencement of the cardiopulmonary bypass (CPB). After CPB, further dissection was done to start separating the pulmonary root from the aorta and LVOT using cautery. The branch pulmonary arteries were aggressively mobilized till the hilar branches on both sides and the ductus divided to enable mobility of the pulmonary root during translocation.
After cardioplegic arrest, a small vertical incision was made in the anterior wall of the main pulmonary artery (PA) and the pulmonary valve inspected for the pliability of the cusps and dysplasia. The valve was bicuspid in the majority of patients (Table 2). After ascertaining the suitability for PRT, a ventriculotomy was performed in the RV wall below the aortic root to assess and confirm the routability of the VSD and the left ventricle (LV) to the aorta tunneling. Following this, pulmonary root harvesting was started using both cautery and sharp scissors to separate the root from the neighboring structures that include the aortic root on the left side, LVOT below, and the right atrial base on the right side (Online Video 1). Because of the dense fibromuscular obstruction, entering the LVOT without damage to the pulmonary valve was always an issue. To manage this problem, after appropriate dissection of the pulmonary root, a right-angled instrument was passed from the main pulmonary artery (MPA) across the pulmonary valve into the LVOT (Online Video 1) to identify the correct place to incise the muscle to enter the LVOT. Using this incision, further harvesting of the pulmonary root was done proceeding first toward the aortic root. At this stage, care was taken not to injure the aortic valve cusp because of the close proximity. On two occasions, we inadvertently entered the aortic root injuring the base of the adjacent coronary cusp. It was repaired primarily using interrupted 7-0 polypropylene sutures simultaneously repairing the rent in the aortic root.
After this, the harvesting was proceeded to separate it from the mitral valve annulus. Again, care was taken not to injure the mitral valve and the cusp base. Using sharp scissors, the appropriate plane of separation between the mitral valve and pulmonary root is reached correctly (Online Video 1). During this dissection, extreme care was taken not to injure the pliable and thin pulmonary valve cusps. However, on two occasions, the pulmonary valve cusps were inadvertently injured. They were repaired finally before implanting into the RV with interrupted sutures of 7-0 polypropylene simultaneously closing the rent in the pulmonary root.
After complete harvesting of the pulmonary root from the LVOT, the root was examined and sized appropriately with the appropriately sized Hegar dilators. Looking from the MPA side, the pulmonary valve commissures were assessed and appropriately divided with a sharp blade to release the commissural fusion. One patient (patient number 15 in Tables 1 and 2) required an incision in the annulus in view of the small size of the annulus. In the same patient, the patent ductus arteriosus stent was removed from the MPA end after cardioplegia and the left pulmonary artery (LPA) origin was reconstructed with a pericardial patch that was used to augment the anterior wall of the MPA.
The pulmonary root was pulled behind the aorta and brought to the left side of the aorta to reach the RV. After this, the VSD was routed with a long oval pericardial patch to construct the LV to aorta tunnel. This was done from the ventriculotomy in all the patients. Following this, the gap in the LVOT was closed with an appropriately sized pericardial patch using interrupted pledgetted polypropylene sutures (Online Video 1). At the end, the pulmonary root was translocated to the RV and sutured to the ventriculotomy. In all cases, an anterior pericardial hood was used for the reconstruction of the RVOT. As described earlier, in patient number 15 (Tables 1 and 2), the reconstruction was done with a 0.1 mm polytetrafluroethylene (PTFE) membrane in a similar fashion as described by us earlier in the patient series of tetralogy of Fallot (TOF) requiring a transannular patch. 10 In all patients, the main PA incision site was augmented with a generous piece of the pericardial patch.
Enlargement of the Ventricular Septal Defect
In 50% of the cases, the VSD was enlarged by cutting in the outlet septum to make the LV to aorta tunnel bigger. An example of this enlargement and cutting is shown in Online Video 1. To accommodate a wider patch for the LV to aorta tunnel, the bites of the suturing near the VSD enlargement were taken on the RV aspect of the tunnel.
Patients With cc-TGA, VSD, and Pulmonary Stenosis
Three patients had cc-TGA in the series (Table 1). In one patient (patient number 1), a Mustard operation (inferior vena cava baffle to the pulmonary ventricle) was done along with a bidirectional Glenn. In the other two patients (patient number 4 and 10), a Senning operation was done.
Addition of Bidirectional Glenn
In four patients with <SC>D</SC>-TGA in the series (Table 1), a bidirectional Glenn (BDG) was added due to a concern that the long LV to aorta tunnel patch might make the RV smaller. In one patient (patient number 11), the already existing BDG was maintained.
Left Pulmonary Artery Origin Reconstruction
In three patients (Table 1), the origin of the LPA was reconstructed with a pericardial patch in continuation of the augmentation patch used to augment the main PA incision site.
Statistical Analysis
All the statistical analysis are performed on SPSS software version 16 version for windows (SPSS, Inc). The study cohort is small; hence, the data are represented in median and minimum and maximum value. The outcome is presented by the Kaplan-Meier curve. The outcome variables selected were death and development of moderate RVOT gradient.
Results
The CPB time ranged from 250 to 460 minutes (median: 310 minutes). The aortic cross-clamp time ranged from 180 to 330 minutes (median: 242 minutes). In the postoperative period, the total ventilation time ranged from 10 to 240 hours (median: 60 hours). Among them, six patients required ventilation for more than 120 hours.
There was one hospital mortality (patient number 16 in Table 3). In this patient, intraoperatively, to expose the VSD for routing the LV to the aorta with a long tunnel patch, we had to detach the septal leaflet of the tricuspid valve (STL; Table 1). In fact, this was the only case in the series where a detachment of the STL had to be done. In addition, the mitral valve was repaired. The patient developed features suggestive of pulmonary edema. This was secondary to significant residual mitral regurgitation.
One patient died four months after discharge at home (patient number 9 in Table 1 and 3). The morbidity postoperatively was secondary to significant ventricular dysfunction. At the time of discharge, the ventricular dysfunction recovered completely. The death at home could not be explained. All the remaining 14 patients are doing well, and the results are summarized in Tables 3 and 4.
Outcomes.
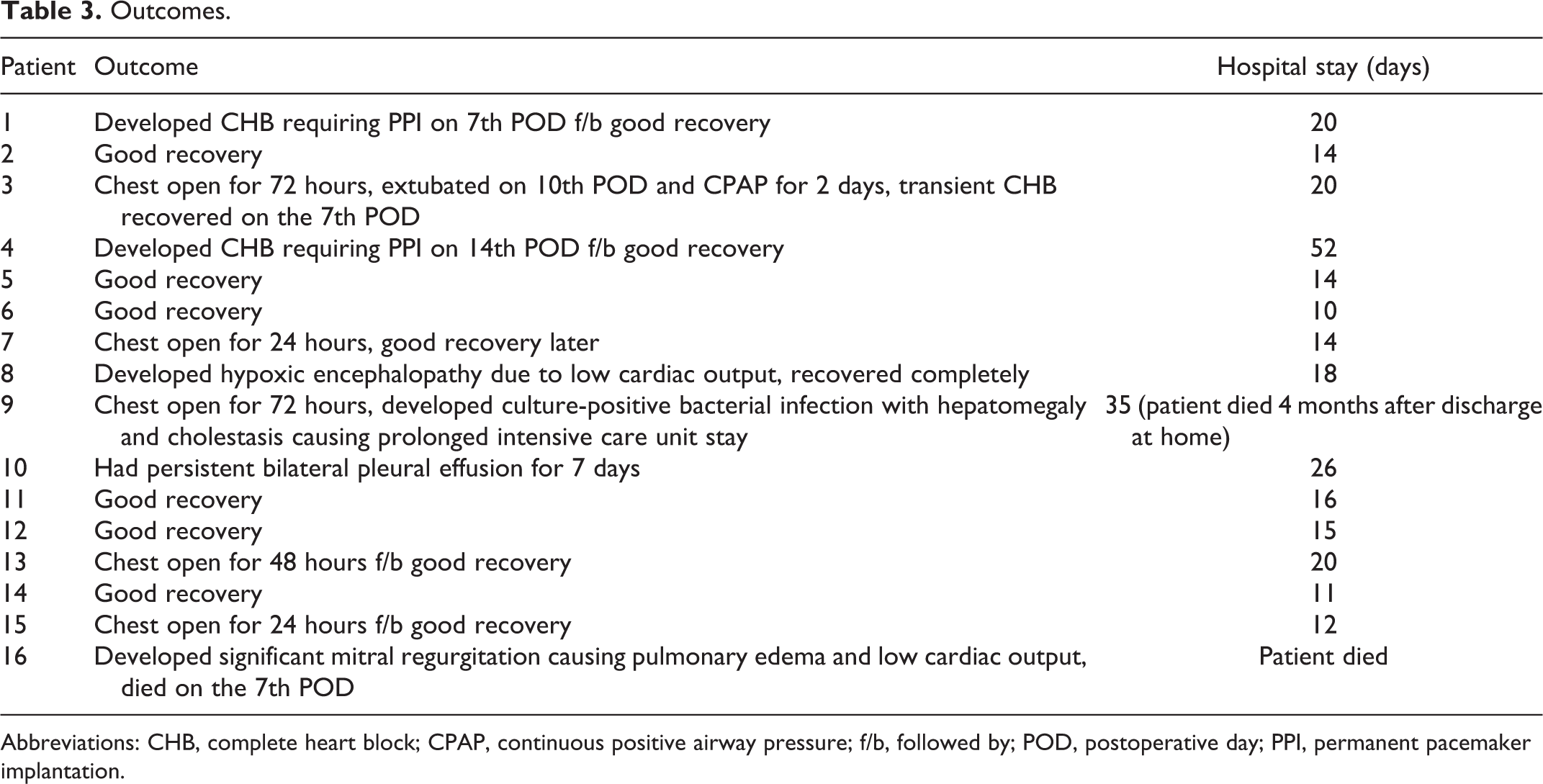
Abbreviations: CHB, complete heart block; CPAP, continuous positive airway pressure; f/b, followed by; POD, postoperative day; PPI, permanent pacemaker implantation.
Postoperative Data and Parameters.a
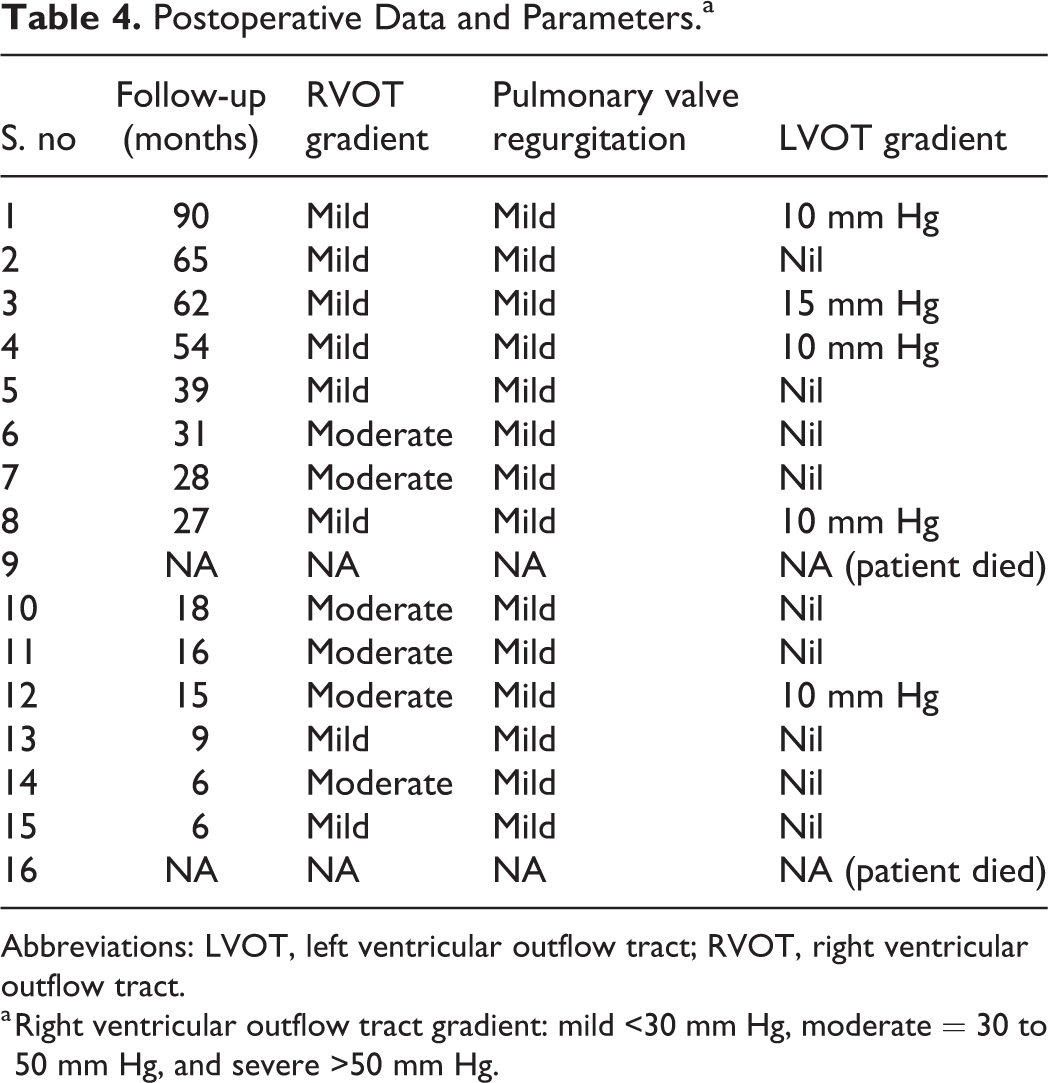
Abbreviations: LVOT, left ventricular outflow tract; RVOT, right ventricular outflow tract.
a Right ventricular outflow tract gradient: mild <30 mm Hg, moderate = 30 to 50 mm Hg, and severe >50 mm Hg.
The median hospital stay is 16 days (range: 10-52 days). The median follow-up is 27 months (range: 4-90 months). Survival free from moderate or greater right ventricular outflow tract (RVOT) obstruction (gradient >40 mm Hg mean) is 57.1% at a maximum follow-up of 90 months (Figure 1). No patient developed a severe gradient (>50 mm Hg mean) across the RVOT. Overall survival at follow-up is 87.5% (Figure 2). Pulmonary regurgitation was trivial to mild in all the cases and did not change throughout the period of follow-up.
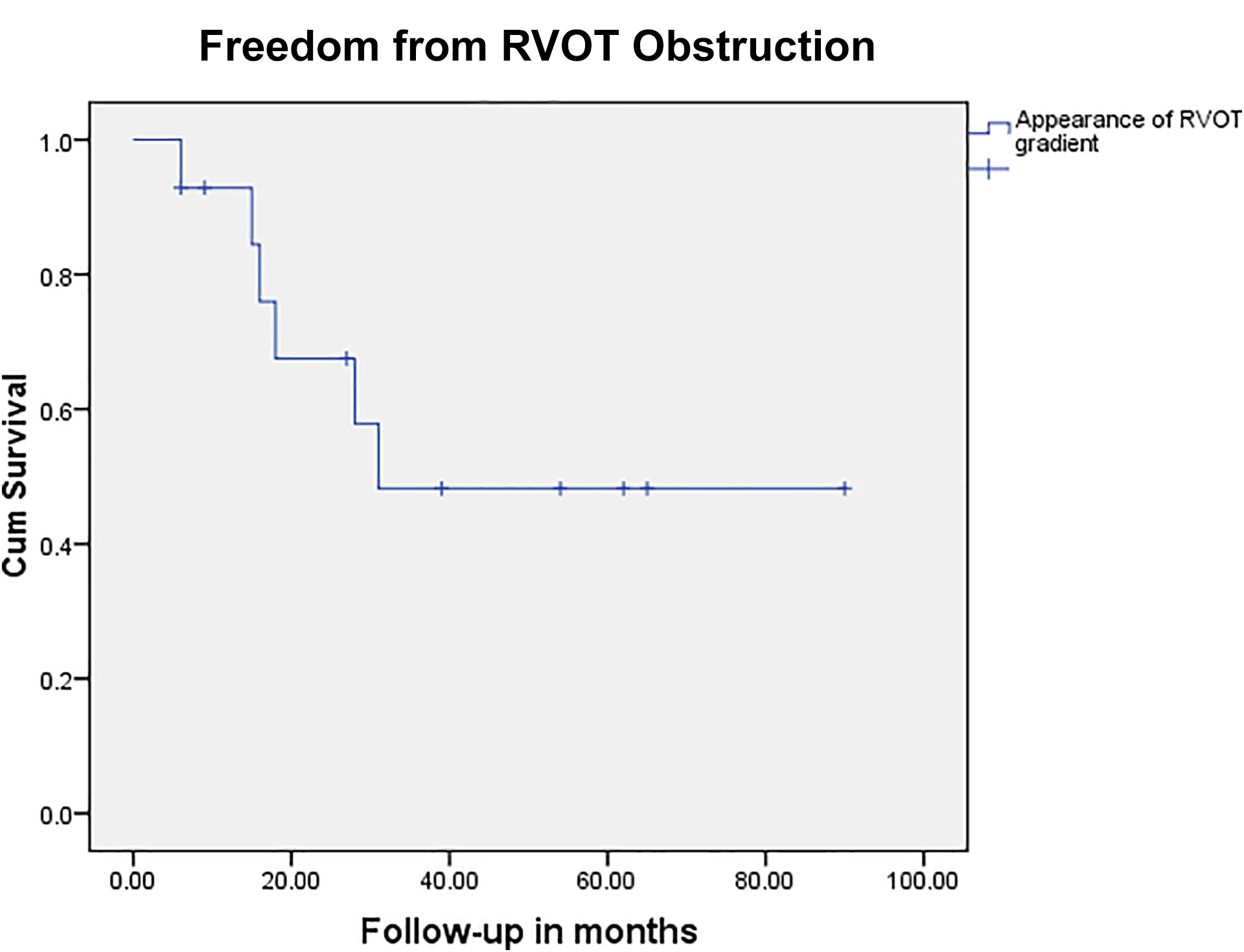
Kaplan-Meier curve showing freedom from moderate or greater right ventricular outflow tract (RVOT) obstruction (gradient >40 mm Hg mean across the RVOT).
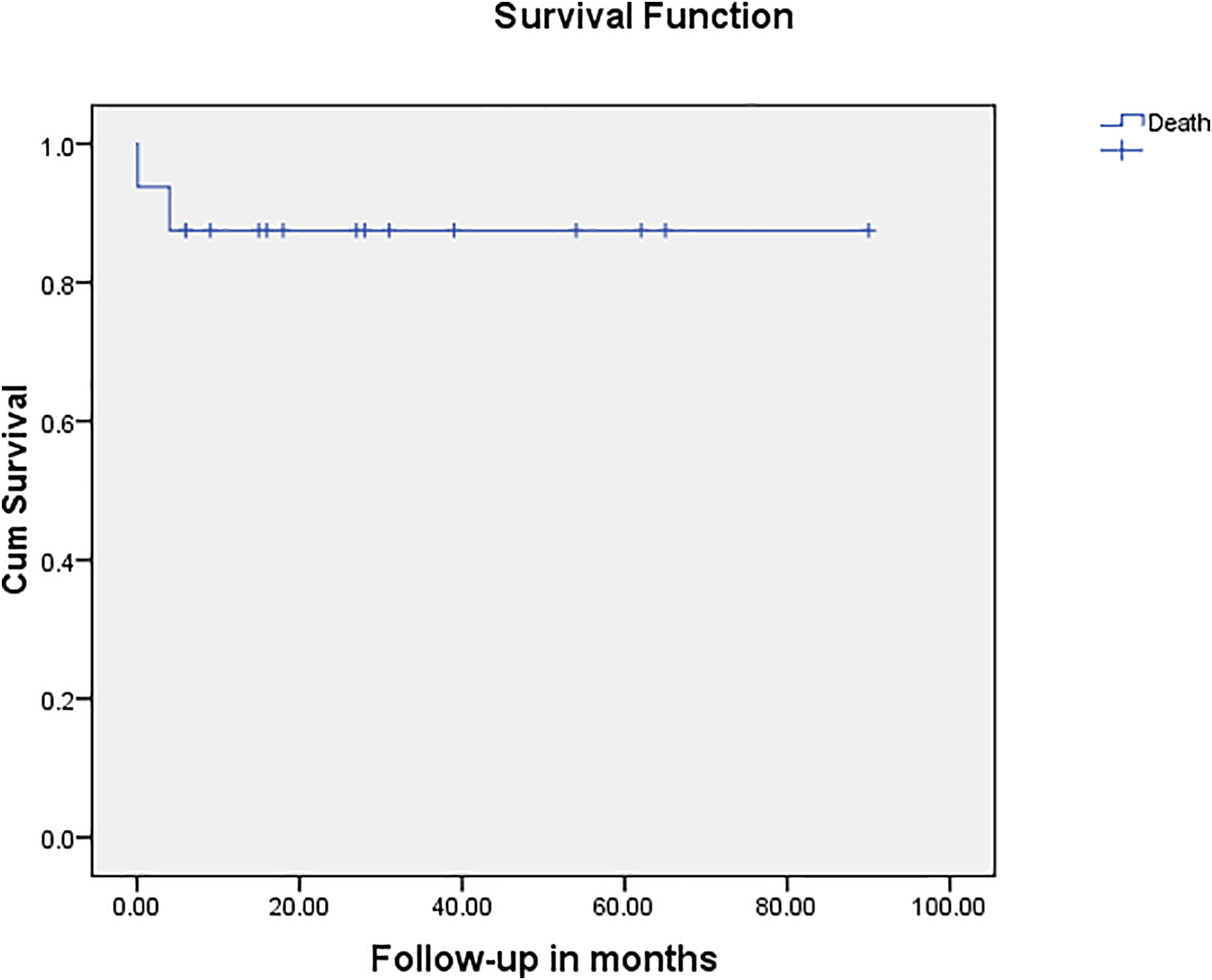
Kaplan-Meier curve showing survival outcome after pulmonary root translocation.
Right Ventricular Outflow Tract Assessment During Follow-Up
Online Videos 2 and 3 show the early follow-up 2D echocardiography assessment of the RVOT (gradient and valve leak). Online Video 2 is of patient number 13 with intact annulus, and Online Video 3 is of patient number 15 who had a transannular patch with RVOT reconstruction with 0.1 mm PTFE membrane.
Comment
In this article, we have described our early experience with anatomical repair of TGA with VSD and LVOTO using the surgical technique of PRT. In our limited early experience with this operation, we realized that this is a good surgical technique to avoid the use of RV to PA conduits 7 and is more important in a country like ours where it is very difficult to procure RV to PA conduits and homografts. In other words, the Rastelli operation, which was initially devised for the surgical treatment of TGA, VSD, and pulmonary stenosis (PS), involves the use of RV to PA conduit. Even though this is the standard operation for this subset of patients, there are problems noticed in the long term. 11 In this context, the translocated pulmonary valve after PRT is an ideal substitute for an RV to PA conduit especially with the potential for growth. 7,8,11
In all patients, the pulmonary valve morphology was favorable for repair by translocation. The preoperative z score and the intraoperative trans esophageal echocardiography (TEE) assessment of the LVOT and the pulmonary valve never dictated the decision to go ahead with the translocation. In other words, the decision to perform translocation was done purely on the intraoperative judgment after opening the main PA and inspecting the valve. This philosophy of repair based purely on the morphology of the pulmonary valve is similar to our own experience in our unit with repair of TOF patients using the annulus and valve-sparing technique (Dharmapuram, 2020). Based on this concept, we noticed in our experience that the pulmonary root after explantation and repair of the valve leaflets appeared more supple and bigger. In patient number 15, the bicuspid valve was not dysplastic and the leaflets were very much supple and pliable. Since the annulus was small (z score = −4.50) and did not engage the required size of the Hegar dilator, we had to resort to a transannular patch repair of the RVOT with reconstruction. In this case, both the leaflets of the valve were sutured together to make a unicuspid posterior cusp in the RVOT that would coapt with the 0.1 mm PTFE membrane to make a competent valve (Online Video 3).
In our early experience, the pulmonary valve has performed fairly well after this procedure. We have demonstrated in our early follow-up that the RVOT is adequate with acceptable gradient which is mild or moderate. In other words, no patient developed significant or severe obstruction requiring reintervention for the RVOT.
The management and prevention of LVOTO is always an issue during surgery for TGA, VSD, and PS. Left ventricular dysfunction and residual LVOTO are known to happen after Rastelli operation. 12 -14 In our experience in this series, LVOT enlargement was done in 50% of cases to get a better alignment of the LV to aorta tunnel without obstruction. We did not encounter any obstruction of the LVOT in our patients (Table 4). Also, none of our patients had developed LV dysfunction postoperatively. However, patient number 9 in our series had severe biventricular dysfunction preoperatively that continued in the postoperative period. The heart function had recovered before discharge; we do not know the exact cause of the death four months after discharge.
In our series, the VSD was routable to the aorta in all the cases; in some of them, the routing was a long LV to aorta tunnel and especially when there was an inlet extension of the VSD. For this reason, in some patients, a BDG was added concomitantly for the concerns of the RV cavity becoming smaller in the presence of a long LV to aorta tunnel. In the same context, the addition of the BDG was never determined by the z score of the pulmonary valve annulus.
While harvesting the pulmonary root, injury to the neighboring structures must be kept in mind. As shown in the Online Video, the mitral valve anterior leaflet is very close to the root on the right side and little anteriorly. This can be handled when we enter the LVOT in the correct place and after that the fibrous tissue separating the pulmonary root and the mitral valve can be carefully incised. The separation of the pulmonary root from the mitral valve should always be done with sharp scissors and not by cautery since cauterization can cause damage to the valve. In our experience, we never had an injury to the mitral valve. In patient number 16 where a concomitant repair of the mitral valve was done, the patient had significant residual mitral regurgitation and hence died in the postoperative period. This valve regurgitation was definitely not related to the harvest of the pulmonary root because of the clear demarcation of the separation by fibrous tissue. The mitral valve repair was done after the pulmonary root was harvested and the base of the anterior leaflet of the valve was very much intact and was not damaged during the harvest. The residual mitral regurgitation was present in the cleft portion of the valve that was repaired. The other two structures in close proximity are the aortic root on the left side and the right atrium on the right side more posteriorly. As described in the surgical technique, on two occasions, a minor injury to the aortic root and the pulmonary valve was effectively handled.
Chronic and long-standing cyanosis in patients with TGA, VSD, and PS can cause irreversible myocardiopathy and hence may be the reason for a bad outcome after operation. In our series, the late death that happened in patient number 9 could be attributed to this reason; however, this was not proven in the investigations that were done. In other words, the optimal timing of surgical correction for PRT should be planned earlier at least below two years of age. In our series, the majority of patients underwent surgery below two years of age.
In our series, three patients belong to the cc-TGA group. This is a small number to comment on the technique of PRT in this setting. However, we feel that it is still a good technique in this subset to avoid a conduit. Unfortunately, two patients among the three developed complete heart block requiring a permanent pacemaker. It is very unfortunate that a complete heart block occurred in these two patients. It occurred despite all care during the VSD closure and pulmonary root harvesting to avoid damaging the bundle in the anterior portion of the VSD and crossing the LVOT, respectively. However, both these patients are doing very well with good heart function and unobstructed RVOT.
To conclude, complete correction of TGA with VSD and LVOTO using PRT can be achieved with acceptable risk in patients with pliable and nondysplastic pulmonary valve. The translocated pulmonary root performed fairly well in this short follow-up. The main advantage of this technique is that the aorta is totally untouched and the coronary arteries are not handled. Even though the harvesting of the pulmonary root from the LVOT is difficult and technically demanding, it is still easily reproducible. This procedure also helps to avoid a conduit in the RVOT; the translocated pulmonary root has the potential to grow without the requirement of a second operation. Even in smaller annuli, this operation can be performed with a transannular patch and reconstruction of the RVOT with competent valves.
Footnotes
Abbreviations and Acronyms
Meeting Presentation
Presented as a surgical video in the video presentation session of the Regional Scientific Meeting of the WSPCHS, Bali, Indonesia during November 2019.
Acknowledgments
The authors are thankful to the following overseas visiting professors to our unit for helping us during their mission with the surgical management of some patients in this series: Dr V. Mohan Reddy from Stanford University, California, and Dr Jose Pedro Da Silva from University of Pittsburgh.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.