
Abstract
Rhabdomyoma in the absence of tuberous sclerosis presenting as a large solitary atrial mass is an atypical finding. We hereby present images from an infant with a fetally diagnosed large left atrial mass with no evidence of mitral valve dysfunction who subsequently developed persistent arrhythmias requiring surgical resection of the mass in the neonatal period.
A newborn female infant with a large left atrial mass noted on fetal echocardiogram at 32 weeks’ gestation was born at term with no perinatal complications. A postnatal echocardiogram confirmed the presence of the mass which appeared to be attached to the posterolateral left atrial wall just above the mitral valve annulus with possible tethering to the posterior leaflet (Figure 1). The mass was mobile but did not protrude through the mitral valve orifice (Video 1). Despite its large size and location, there were no signs of mitral valve inflow obstruction or regurgitation (Video 2). The infant was hemodynamically stable with no other anomalies. Given the characteristic of the mass as a single lesion and its location in the left atrium, our initial diagnosis was an atypical myxoma and the consensus was to electively resect the mass at around two to three months of age to allow the newborn to grow before putting her on cardiopulmonary bypass. However, she was readmitted at one month of life for episodes of hemodynamically unstable supraventricular tachycardia (SVT), which required administration of multiple doses of adenosine and synchronized cardioversion for control. Her refractory arrhythmia prompted earlier surgical resection of the mass. Intraoperatively, a large mass was found occupying the majority of the left atrium. The mass was attached to the posterior annulus of the mitral valve in a broad-based stalk and was densely adherent to the posterior leaflet of the mitral valve with no secondary attachments to the valve. Once the mass was removed in its entirety, there were two leaflet perforations that were evident. As this was a friable newborn mitral valve that was attached to the tumor, the concern was that there was potential to tear further, creating more severe mitral regurgitation; hence, these perforations were repaired with 7-0 Prolene sutures and an autologous pericardial pledget. The resected mass was noted to be smooth and homogenous, measuring 9 × 12 mm (Figure 2). Pathology confirmed a cardiac rhabdomyoma. Her brain magnetic resonance imaging (MRI) did not identify any masses and genetic testing was negative for tuberous sclerosis. Although there was a risk of a nidus of thrombus formation derived from the stitches in her mitral valve, postoperative anticoagulation was not initiated given the overall low risk of this potential occurrence along with the absence of thromboemboli on her brain MRI. She had a relatively uncomplicated immediate postoperative course and was initially discharged on propranolol for control of her SVT. However, she developed recurrent SVT a week after discharge and was started on a second agent, flecainide. Her arrhythmia was well controlled after starting on dual therapy with no evidence of recurrence on her serial Holter monitor tracings. She continued to do well and was weaned off both medications at one year of age. Her follow-up echocardiograms showed no evidence of recurrence of the mass, and she continued to have a normal mitral valve and ventricular function. She continues to be followed annually for at least the next five years. Our case highlights atypical presentation of a cardiac rhabdomyoma as a solitary lesion detected prenatally in the left atrium in the absence of tuberous sclerosis. Although the natural history of rhabdomyomas is often characterized by spontaneous regression with time, even patients who present with stable hemodynamics may be at risk for significant arrhythmogenic presentations requiring earlier surgical intervention.
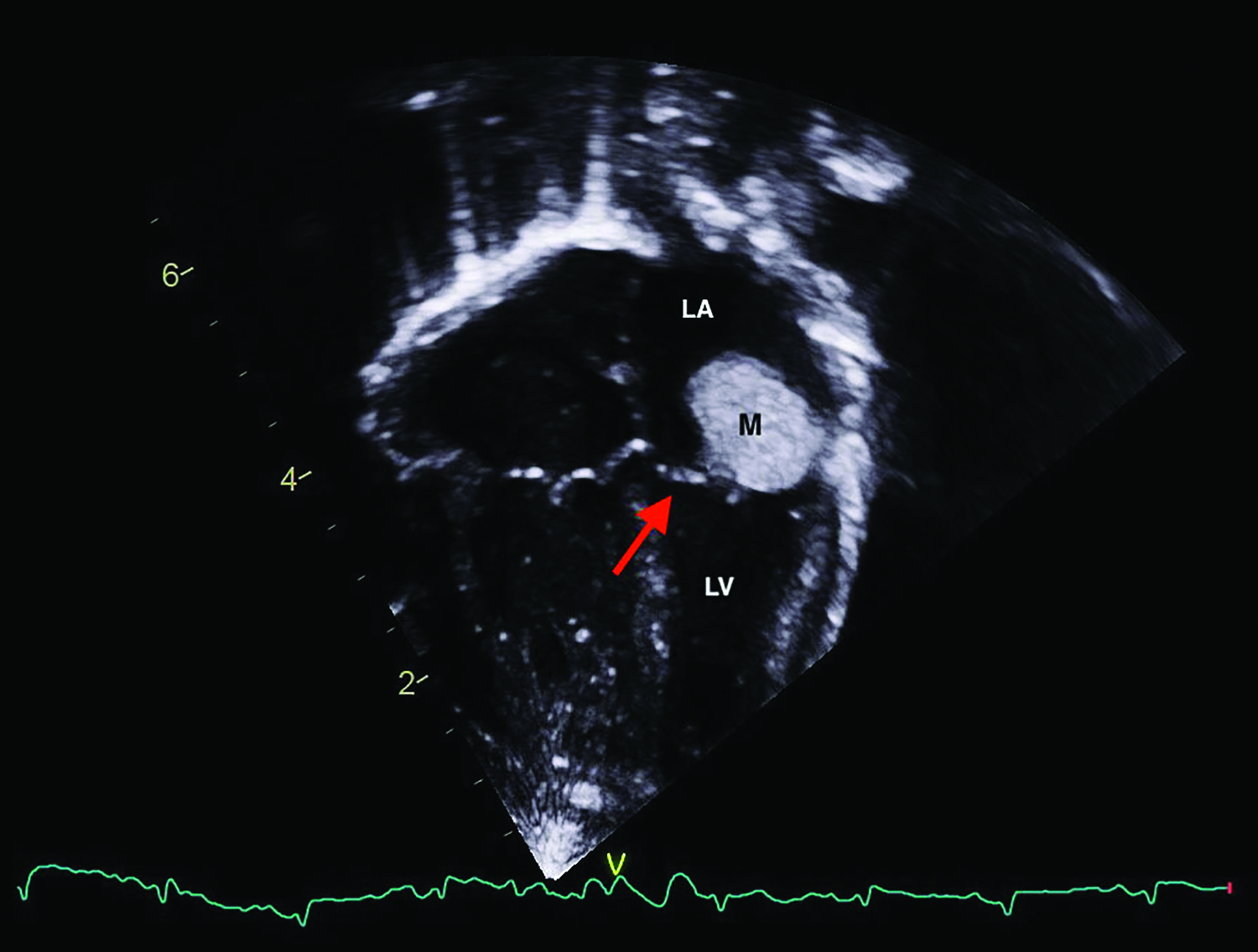
An apical 4-chamber view of transthoracic echocardiography showing a well-circumscribed homogenous hyperechoic mass in the LA just above the mitral valve (red arrow). LA indicates left atrium; LV, left ventricle; M, mass.

Gross specimen revealed a well-circumscribed homogenous mass measuring 9 × 12 mm.
Footnotes
Author’s Statement
The patient’s parents consented to the submission and publication of this report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.