
Abstract
We report an anterior translocation of the right pulmonary artery procedure to relieve severe left bronchial obstruction that was caused by right pulmonary artery stent placement in a 1-year-old patient with truncus arteriosus and interrupted aortic arch. After neonatal repair, the patient re-presented with severe truncal valve regurgitation, right pulmonary artery stenosis, and severe biventricular dysfunction, which was treated with truncal valve repair and right pulmonary artery plasty. The patient suffered from left bronchial compression from right pulmonary artery stent placement, which was successfully treated by the translocation procedure. Bronchial stenosis was successfully relieved by the translocation procedure. Indications, advantages, and disadvantages of this procedure are discussed.
Keywords
Introduction
Repair for truncus arteriosus (TA) and interrupted aortic arch (IAA) is complex and creates a unique postoperative geometrical problem where a larger and shorter ascending aorta leaves little room for the branch pulmonary arteries (PAs) and the bronchus. Children with conotruncal abnormalities are at risk for bronchial compression after intracardiac repair due to increased truncal root size, especially following reinterventions to the branch PAs. 1 Anterior or posterior aortopexy is an option, 2 however it is less successful in cases with large anterior structures. We report a novel translocation procedure to relieve severe left bronchial obstruction that was caused by right PA stent placement.
Case Report
The female patient underwent uneventful repair of TA/IAA and truncal valve repair. At 13 months of age, the child re-presented with severe truncal valve regurgitation, right PA stenosis, and severe biventricular dysfunction. The child underwent a truncal valve repair, conduit exchange, and right PA plasty. The ascending aorta was transected in order to access the truncal valve and the right PA. When suturing the aorta together, it was clear that the aorta would compress the right PA, however extending the aorta with a graft in a 1-year-old child did not seem ideal, so a direct anastomosis was completed. The child required extracorporeal membrane oxygenation (ECMO) for biventricular dysfunction. While on ECMO, residual severe right PA stenosis was treated with a stent. The patient was weaned from ECMO but CT scans indicated severe left main bronchial stenosis and complete collapse of the left lung (Figure 1). Posterior aortoplexy was performed with no effect.
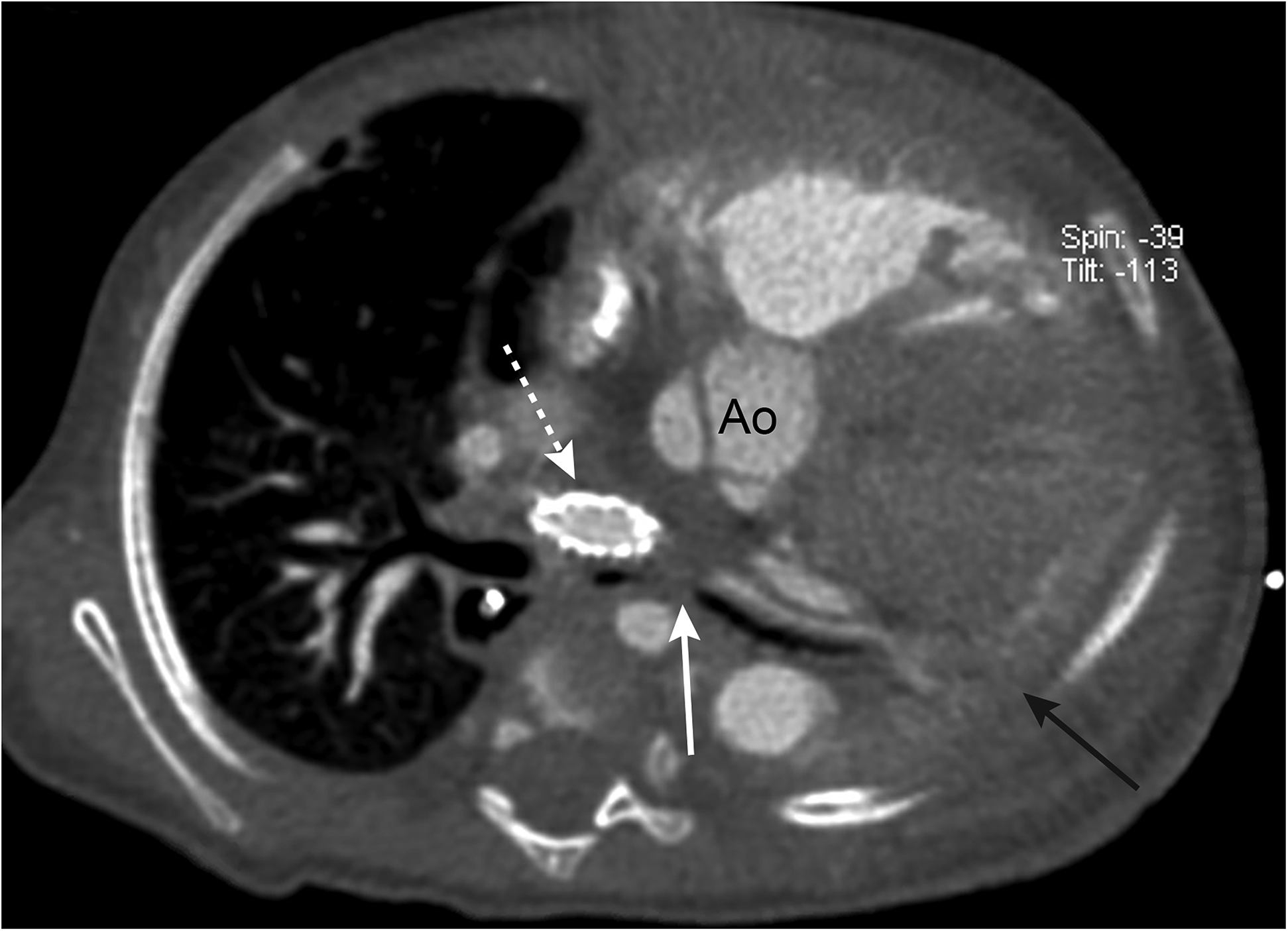
Preoperative cardiac CT shows obliteration of the left bronchus (solid white arrow) by the stented right PA (dashed white arrow) and left lung collapse (black solid arrow)
Translocation Procedure
Under cardiopulmonary bypass (CPB), the right PA was transected and brought to the right side of the ascending aorta and the stent was removed. A 10 mm ringed GoreTex graft (W. L. Gore & Associates, AZ) was sewn to the distal right PA, and was brought in front of the ascending aorta. The right PA origin was oversewn and the graft was anastomosed to a new location on the conduit at its rightward anterior aspect. The child was extubated on postoperative day 6. Postoperative CT scans indicated significant improvement in left bronchial geometry and patency (Figure 2).
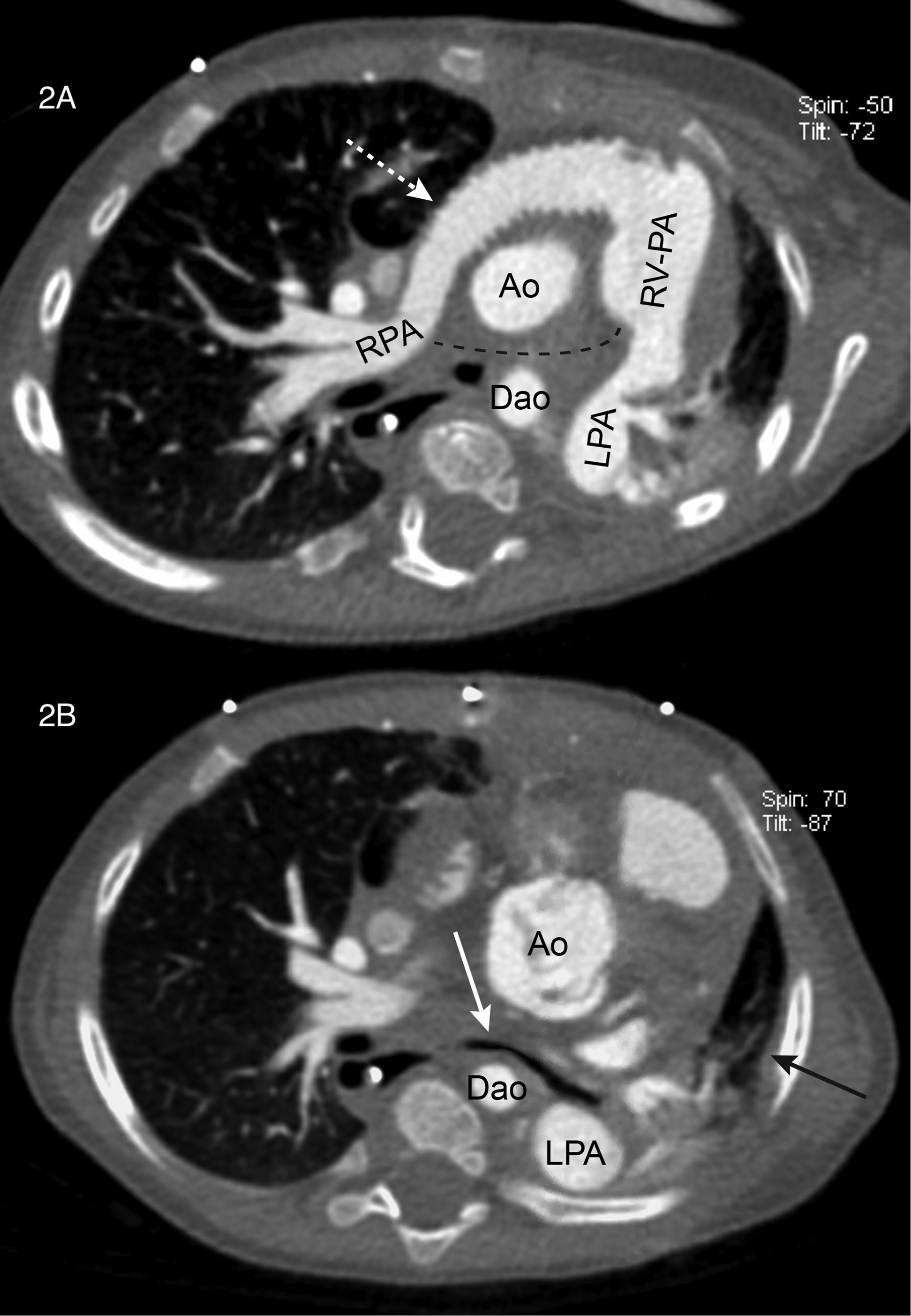
Postoperative CT shows a relocated right PA with a graft (dashed white arrow), previous right PA location (dashed black line, A), improved left bronchus (solid white arrow, B), and re-expanded left lung (solid black arrow).
Comment
This report demonstrates the effectiveness of the translocation procedure to relieve the airway obstruction and highlights the geometrical challenge of TA/IAA, ie, limited space underneath the large and short neo-ascending aorta, and multifactorial nature of bronchial compression in patients with conotruncal abnormalities. The effectiveness of the translocation procedure to relieve airway compression has been described in Tetralogy of Fallot with absent PA syndrome. 3,4 This approach is particularly effective when the branch PA is disproportionally large and occupies substantial space in the window underneath the aorta. 3 The problem in this case was unique where the airway compression was caused by the right PA stent, which is also a recognized phenomenon. 5 The right PA stenting was necessary to wean from ECMO in the context of the failing right ventricle. The left PA was not contributing to bronchial compression and therefore relocation of the left PA was not necessary.
This procedure does not require extensive mobilization of the conduit and/or branch PAs or transection of the ascending aorta. In theory, this procedure can be done without cardioplegic cardiac arrest although we commenced cardioplegic arrest due to the presence of intraatrial communication. Having an interposition graft with no growth potential is a disadvantage. We intentionally oversized the graft so that the graft remains unobstructed until the next intervention. The anteriorly-relocated right PA may increase the risk of sternal reentry.
An alternative strategy is to extend either ascending aorta 6 or transverse aortic arch. 7 We did not employ this strategy for 2 reasons: (1) placing an interposition aortic graft in a growing child is not ideal and (2) extending the aortic arch requires deep hypothermic circulatory arrest. Given this patient's ventricular dysfunction, we explored the less invasive surgical option. Another option is to translocate the right PA at the time of primary repair, 8 which in this case would be at the time of truncal valve repair. Lastly, careful right PA stent dilation under bronchoscopy guidance may have prevented obliteration of the left bronchial lumen. 9
The use of an anterior translocation of the right PA procedure was effective to relieve refractory left bronchial compression without additional surgery to the aorta. The procedure can be an attractive option in selective pediatric population with challenging great vessel anatomies.