
Abstract
Objective
We reviewed our center's prenatal detection and surgical experience with high-risk, 2-ventricle patients, with complex congenital heart disease that underwent stage-1 hybrid palliation.
Methods
We retrospectively identified those born between March 2008 and March 2021 with 2-ventricle hearts, complex congenital cardiovascular malformations, and ductal-dependent systemic circulation that underwent stage-1 hybrid palliation consisting of surgical bilateral pulmonary artery banding and interventional catheterization placed ductus arteriosus stents.
Results
We identified 30 patients. Of the 30, 19 (63%) were male. For the 30, median gestational age was 35 weeks (29-39 weeks), and median birth weight was 2.2 kg (0.6-4.5 kg). Of the 30, 1 was transferred from an adjacent state, and 29 were born in Nevada. Of the 29 born in Nevada, overall statewide prenatal detection was 18 of 29 (62%); however, for 2008 to 2011 the prenatal detection rate was 3 of 10 (30%) and 15 of 19 (79%) for 2012 to 2021, P = .03. For the last 5 years, prenatal detection for Nevada-born patients was 8 of 8 (100%). Two full-term newborns, without a prenatal diagnosis, presented postnatally in extremis. For the 30 patients, there were 0 stage-1 hybrid palliation mortalities, 1 subsequent repair mortality, and 3 late nonsurgical deaths.
Conclusions
Stage-1 hybrid palliation may result in excellent surgical outcomes for high-risk, 2-ventricle patients. Additionally, high rates of population-wide prenatal detection are possible for high-risk congenital heart disease, allowing prenatal planning and possibly reducing postnatal extremis presentations.
Introduction
For neonates undergoing open-heart palliative or reparative surgical procedures, mortality substantially increases with prematurity, birth weights <2.5 kg, dysmorphic syndromes, extremis presentations with multiorgan dysfunction, and associated noncardiac malformations.1-6 In 2007, our center began applying stage-1 hybrid palliation for low- and high-risk hypoplastic left heart syndrome patients.7-9 Shortly afterward, we extended stage-1 hybrid palliation to include high-risk, 2-ventricle patients with ductal-dependent systemic circulation. We previously reported stage-1 hybrid palliation mortality rates of 0%, 3%, and 18%, respectively, for high-risk 2 ventricles, low-risk hypoplastic left heart, and high-risk hypoplastic left heart patients. 10 This report details results from a larger cohort of high-risk, 2-ventricle patients with complex congenital heart disease and ductal-dependent systemic circulation.
Methods
The study protocol conformed to the principles of the Declaration of Helsinki. The local Sunrise Health Institutional Review Board approved this study and exempted it from requiring consent. We accessed data for this retrospective, observational report by inquiring our research database (Epi-Info™), a congenital heart disease prenatal detection database, and our electronic medical records (EMR). The Epi-Info database is maintained by the Congenital Heart Center Nevada's research director, and data is exclusively entered from coding sheets completed by our center's physicians from each patient encounter or procedure. No individual or other party external to our center can access our Epi-Info database, congenital heart disease database, or EMR. All data were collected and managed internally to the Congenital Heart Center Nevada; thus, additional inquiry of third-party databases, either hospital or governmental, was unnecessary for data extraction. For the searchable parts of our EMR, we used Perceptive Software by Lexmark International, Inc. As the sole provider of prenatal and postnatal congenital cardiology services in the state, our electronic databases include information on all patients diagnosed with congenital heart disease in Nevada. Following the database and EMR inquiry, we reviewed patient records and collated data for analysis. For statistical testing, we used SPSS version 13.0 by SPSS Inc. We used nonparametric testing, including the Mann–Whitney U test, and we set a P-value of <.05 as significant.
Patients
We retrospectively identified patients born between March 2008 and March 2021 with 2-ventricle hearts, complex congenital cardiovascular malformations, and ductal-dependent systemic circulation that underwent stage-1 hybrid palliation, consisting of surgical bilateral pulmonary artery banding and interventional catheterization placed ductus arteriosus stents. One patient thought initially to be amenable to a 2-ventricular repair who ultimately required Fontan palliation, was excluded from the analysis. No patients with initially diagnosed functional univentricles that underwent stage-1 hybrid palliation ultimately had biventricular repairs. No syndromic patients were excluded. No families, when offered stage-1 hybrid palliation, elected comfort care. One 28-week, 510-g infant, with a balanced atrioventricular septal defect and hypoplastic aortic arch, died preoperatively. No patients were included that underwent bilateral pulmonary artery banding and continued prostaglandin use until open-heart surgical palliation or repair. Presurgical cardiovascular physiology and anatomical imaging, including cardiovascular measurements, were undertaken by postnatal echocardiography, rapid computed tomography, or cardiac catheterization and angiography. As outpatients, approximately every 2- to 4-week evaluation was undertaken with a complete echocardiographic assessment to guide the timing of possible post stage-1 hybrid interventional catheterization or diagnostic cardiac catheterization or computed tomographic studies before subsequent surgical procedures.
Fetal-Cardiology Program
We have described our statewide fetal-cardiology program elsewhere.11-13 Briefly, the program encompasses ongoing educational symposia for general obstetric and specialized perinatal sonographers and on-site fetal cardiologists that supervise all diagnostic, comprehensive fetal echocardiograms at each of the state's perinatology clinics 5 days a week with 24/7 on-call services. General obstetric sonographer training includes a series of half-day didactic lectures that detail the 5-axial view fetal echocardiographic screening method (transverse abdominal, 4-chamber, left outflow, right outflow, and 3-vessel trachea views), 14 which we continued online during the COVID-19 pandemic. Program personnel includes 7 fetal cardiologists that provide coverage to 11 maternal-fetal-medicine offices, throughout Nevada, in 5 different perinatal groups, with a total of 40 perinatal sonographers, all trained to perform comprehensive fetal echocardiograms, with each diagnostic study under the supervision of a fetal cardiologist. Deliveries, whether premature or term, were either spontaneous or secondary to obstetric management. Fetal cardiologists did not recommend early delivery for any patient in this study's cohort.
Stage-1 Hybrid Palliation and Other Surgical Techniques
Patients were maintained on prostaglandins until stage-1 hybrid palliation was initiated with off-pump, bilateral pulmonary artery banding through a median sternotomy, using 3.5-mm polytetrafluoroethylene bands (Gore-Tex, W.L. Gore & Associates) for patient weights >2.5 kg and 3.0-mm bands for patient weights <2.5 kg. Between the years 2008 and 2011, ∼24 to 38 h post pulmonary artery banding, interventional cardiac catheterization was undertaken with anesthesia and percutaneous placement of eV3 Everflex Protégé stents (Medtronic) into the ductus arteriosus to complete stage-1 hybrid palliation. After 2011, ductal stenting was performed simultaneously with bilateral pulmonary artery banding in a hybrid operating room via the placement of a 6-French sheath directly into the main pulmonary artery during open expose for the interventional-cardiology ductal stent delivery. Open-heart surgical palliation and reparative procedures following stage-1 palliation included Norwood/Damus–Kaye–Stansel procedures with aortopulmonary artery or cavopulmonary shunts. Reparative procedures included hypoplastic or interrupted arch repairs, ventricular septal defect closures, arterial switch operations, and right ventricle-to-pulmonary artery conduits, with either aortic or pulmonary allografts, when required.
Additional technical surgical aspects included the following. Bilateral pulmonary artery debanding, ductus arteriosus stent removal with the reconstruction of the pulmonary artery on the site of the stent and reconstruction of the aortic arch. If required, pulmonary artery reconstruction was achieved using autologous pericardium. Cannulation of the brachiocephalic vessels is performed either directly or later in the series with a Gore-Tex (W.L. Gore & Associates Flagstaff) chimney graft, which may serve as the aortopulmonary shunt at the end of the surgical sequence. Both selective cerebral and selective cerebral-coronary perfusion were utilized, and we cooled to 18 °C to 24 °C, depending on the case. We were liberal about using 2 arterial cannulas whenever the ductal stent was obstructing distal aortic flow (second arterial cannula in the pulmonary artery or ductus arteriosus). A pulmonary artery allograft, typically a hemipulmonary artery patch, was used for the aortic arch repair or the Damus Kaye Stansel procedure. If the chimney graft was converted to an aortopulmonary artery shunt during warming the Damus Kay Stansel was recannulated. Full dose del Nido cardioplegia (constituted by the inpatient pharmacy) was utilized prior to cross-clamp or halting of coronary perfusion.
Results
We identified 30 patients. Of the 30, 19 (63%) were male. For the 30, median gestational age was 35 weeks (29-39 weeks), and median birth weight was 2.2 kg (0.6-4.5 kg). Of the 30, 1 was transferred from an adjacent state, and 29 were born in Nevada. Of the 29 born in Nevada, all with documented prenatal care, overall statewide prenatal detection was 18 of 29 (62%); however, for 2008 to 2011, the prenatal detection rate was 3 of 10 (30%) and 15 of 19 (79%) for 2012 to 2021, p = .03. For the last 5 years, prenatal detection for Nevada-born patients was 8 of 8 (100%).
The 30 patients underwent stage-1 hybrid at 21 ± 15 days old with 0 mortality. Table 1 lists each patient in order of date-of-birth by birth year and includes primary cardiac diagnosis, prenatal detection, gestational age, birth weight, aortic annulus Z values (Boston), 15 syndromes, indications for stage-1 hybrid palliation (risk factors for initial 2-ventricle repair), and long-term outcome. Two full-term newborns (patient numbers 10 and 22), without a prenatal diagnosis, both presented postnatally in extremis, following well newborn nursery discharge. Summary of the risk factors for initial 2-ventricle repair: 10 with aortic annulus Z < −3 16 ; 18 with 1 or more of the following, birth weight <2.5 kg, syndrome, heterotaxy, or extremis; 1 with borderline right ventricular size in a common arterial trunk; and 1 with aortic atresia and ventricular septal defect in a 2-ventricle heart. Figure 1 displays the graph of length of stay in days versus birth weight following birth to discharge after stage-1 hybrid, with a length of stay negatively correlating with birth weight, R = −0.65 and P = .0002. Table 2 summarizes the syndromes encountered. Following stage-1 hybrid and before additional surgery, 3 patients had an interventional cardiac catheterization: 2 for patent ductus arteriosus stent dilations and 1 for a pulmonary artery band dilation. There were no interventional cardiac catheterization morbidities or mortalities for these 3 patients. Table 3 lists additional noncardiac surgical procedures performed during the initial hospitalization.
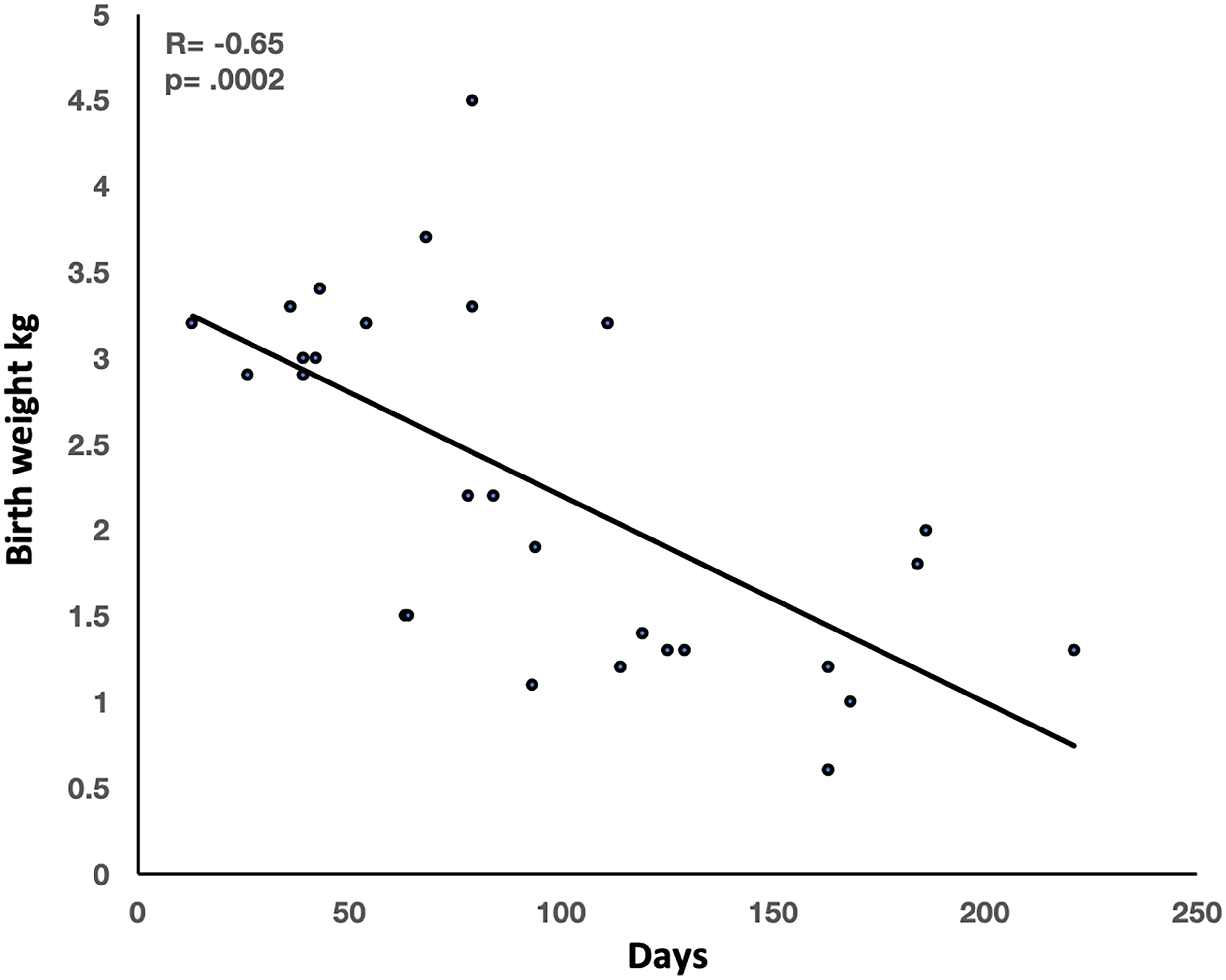
Length of stay from birth to discharge after stage-1 hybrid palliation.
Patient List.
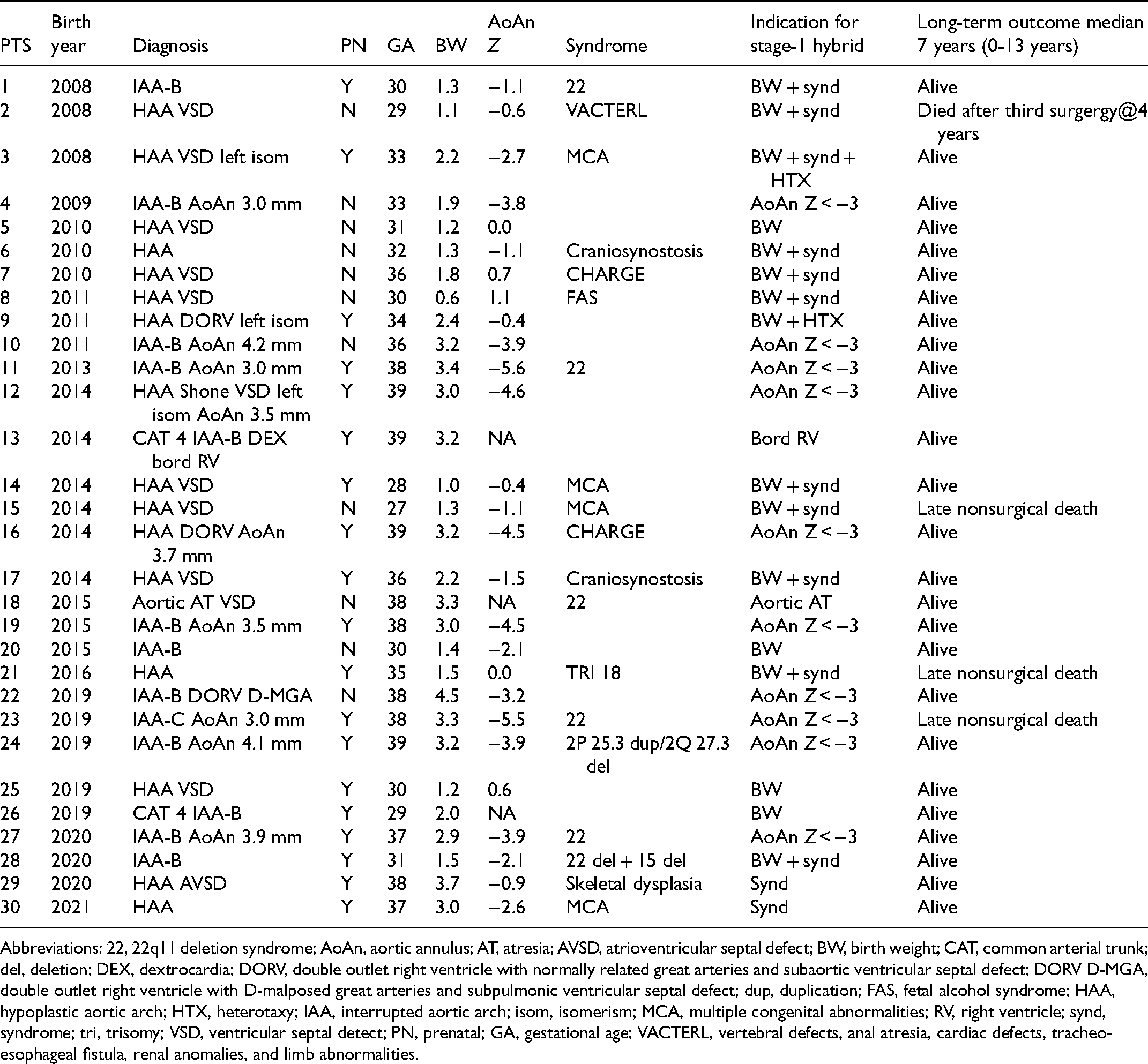
Abbreviations: 22, 22q11 deletion syndrome; AoAn, aortic annulus; AT, atresia; AVSD, atrioventricular septal defect; BW, birth weight; CAT, common arterial trunk; del, deletion; DEX, dextrocardia; DORV, double outlet right ventricle with normally related great arteries and subaortic ventricular septal defect; DORV D-MGA, double outlet right ventricle with D-malposed great arteries and subpulmonic ventricular septal defect; dup, duplication; FAS, fetal alcohol syndrome; HAA, hypoplastic aortic arch; HTX, heterotaxy; IAA, interrupted aortic arch; isom, isomerism; MCA, multiple congenital abnormalities; RV, right ventricle; synd, syndrome; tri, trisomy; VSD, ventricular septal detect; PN, prenatal; GA, gestational age; VACTERL, vertebral defects, anal atresia, cardiac defects, tracheo-esophageal fistula, renal anomalies, and limb abnormalities.
Syndromes.
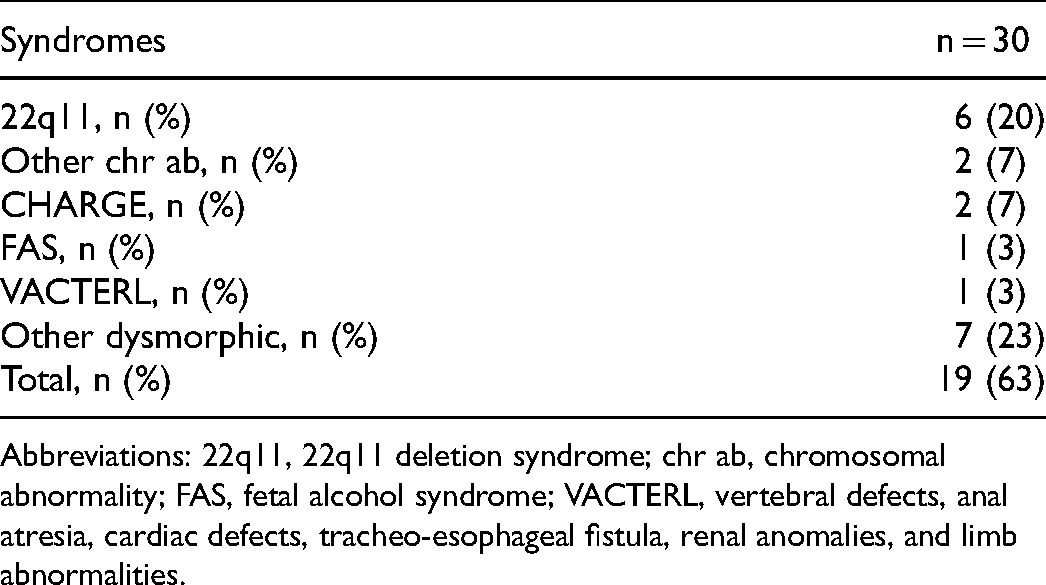
Abbreviations: 22q11, 22q11 deletion syndrome; chr ab, chromosomal abnormality; FAS, fetal alcohol syndrome; VACTERL, vertebral defects, anal atresia, cardiac defects, tracheo-esophageal fistula, renal anomalies, and limb abnormalities.
Noncardiac Surgeries.
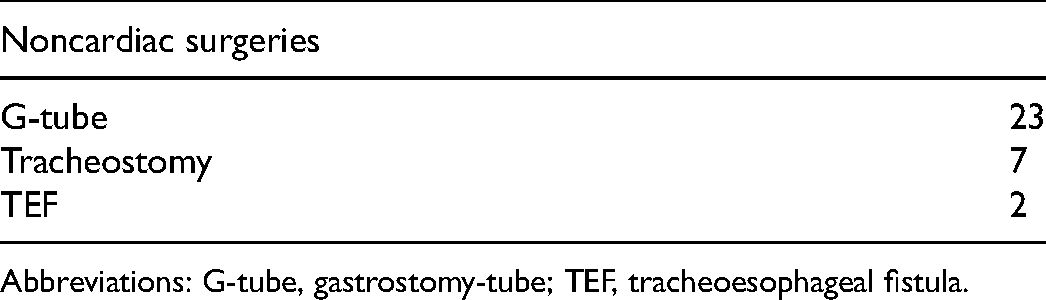
Abbreviations: G-tube, gastrostomy-tube; TEF, tracheoesophageal fistula.
Figure 2 outlines the subsequent surgical procedures for 29 of the 30 patients, with 1 patient awaiting repair. Second surgeries were performed at 6 ± 3 months old at 7.2 ± 1.3 kg with 0 mortality, third surgeries at 26 ± 14 months old with 1 mortality, and a fourth surgery at 35 months old without mortality. There were no surgical reinterventions for pulmonary arterioplasty. Of the 10 patients with an initial aortic annulus Z < −3, 4 had Damus–Kaye–Stansel’s, 1 had an arterial switch, and 5 underwent repair after the initial stage-1 hybrid. Of the later 5, initial average aortic annulus measurements and Z scores were 3.8 mm (3.4-4.5 mm) and −4.2 (−3.5 to −4.5) and at repair average age was 7 months (2-10 months), and average aortic annulus measurements and Z scores were 7.0 mm (6.6-8.0 mm) and −2.2 (−1.6 to −2.8). Following reparative procedures that were performed by 6 months of age, after initial stage-1 hybrid, 3 patients had reoperations for subaortic stenosis: 1 at 46 months with interrupted aortic arch type B and an initial aortic annulus Z value of −4.6, 1 at 35 months with a hypoplastic aortic arch and double outlet right ventricle and an initial aortic annulus Z value of −4.5, and 1 at 13 months with interrupted aortic arch type B and an initial aortic annulus Z value of −2.1. For all 3 patients, there appeared to be no initial consistent anatomical subaortic features discrepant from other patients that predicted the potential development of significant subaortic stenosis. Following reparative procedures, 3 patients had an interventional cardiac catheterization, 1 for a left pulmonary artery stent, 1 for bilateral pulmonary artery angioplasties, and 1 for an aortic valvuloplasty. There were no interventional cardiac catheterization morbidities or mortalities for these 3 patients.
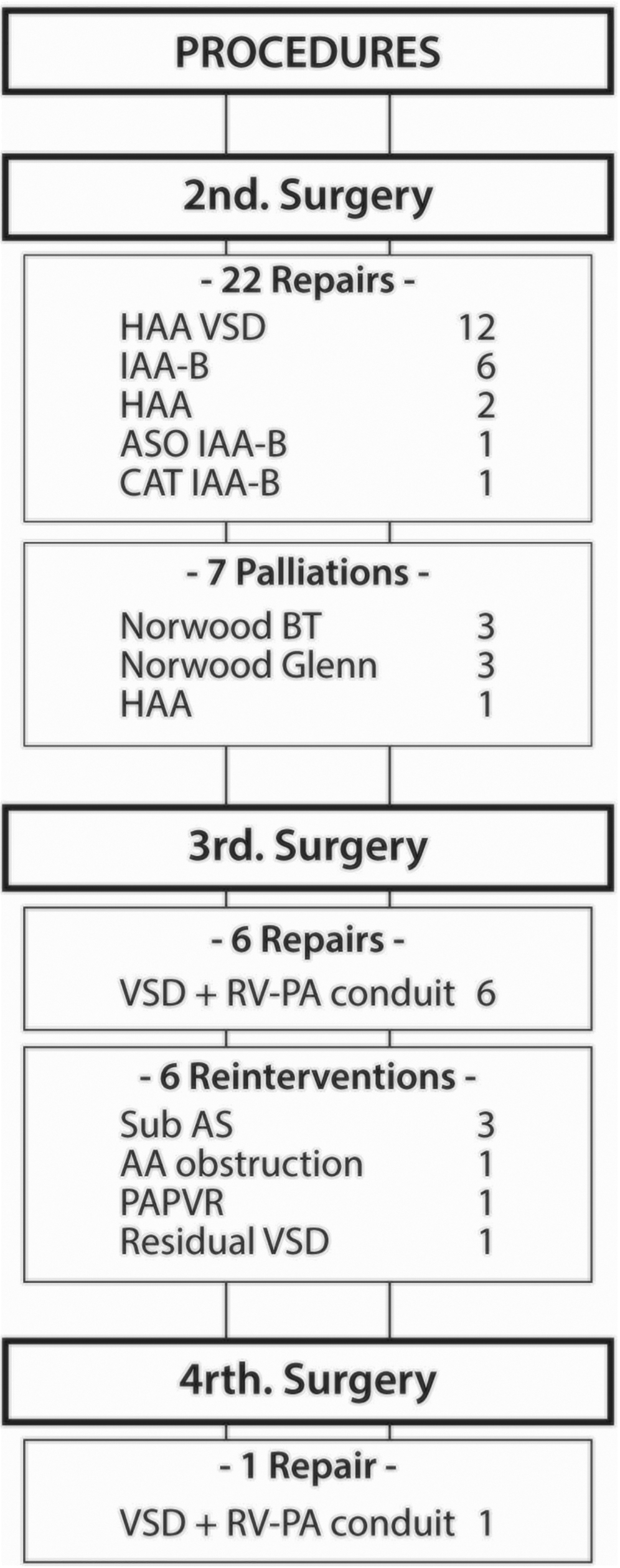
Procedures following state-1 hybrid palliation.
Discussion
Our center has adopted neonatal stage-1 hybrid palliation for 2-ventricle hearts with complex congenital cardiovascular malformations and ductal-dependent systemic circulation if accompanied by prematurity, low birth weights, dysmorphic syndromes, and extremis presentations with multiorgan dysfunction. Additional indications include borderline ventricular sizes and aortic valve diameters. Using a staged approach, our series of 30 patients experienced only 1 post-surgical death out of 82 total cardiovascular surgical procedures. To the best of our knowledge, there are few reports that have analyzed a series of high-risk, 2-ventricle neonates undergoing stage-1 hybrid palliation. Yerebakan et al 17 reported the long-term results of biventricular repair after initial stage-1 hybrid palliation for hypoplastic left heart variants. However, as per their method's section, they excluded severe syndromes with prognostic relevance. Also, their smallest patient weighed 1.6 kg. Additionally, Sakurai et al 18 reported a series of high-risk, 2-ventricle patients with ductal-dependent systemic circulation lesions treated with long-term prostaglandin and later additional surgical intervention; however, none had successfully placed ductal stents, primarily because approved stents were not available in their region during most of the study period. Further, Sakurai's patient cohort average weights were greater than ours; plus, their method's section made no mention of those with dysmorphic syndromes. Although we utilize bilateral pulmonary artery banding and continued prostaglandin administration for both 1 and 2-ventricle patients (none of which are included in this report), ductal stenting allows either open-heart palliative or reparative procedures to be undertaken well beyond the neonatal period. Otherwise, except for a small case series of 6 patients from Erek et al, 19 most publications describing the use of stage-1 hybrid palliation for high-risk, 2-ventricle patients with complex congenital heart disease are limited primarily to case reports.
In contrast to hypoplastic left heart syndrome with severe aortic and mitral valve hypoplasia or atresia, 10 there were no significant hemodynamic issues resulting from restricted interatrial or retrograde aortic arch flow, as forward aortic and unrestricted mitral flow were present, other than the single patient with aortic atresia and ventricular septal defect, who did not develop retrograde aortic arch obstruction. Nevertheless, considerable alternative comorbidities were present, often resulting in additional noncardiac surgical procedures such as gastrostomy-tube placements and tracheostomy.
A major limitation of this analysis is the number of patients, inherent in studying rare conditions. Also, we are comparing our results with others from the literature rather than undertaking a randomized study between stage-1 hybrid palliation versus neonatal open-heart palliation or reparative procedures. Other than avoiding the discharge of an affected neonate from the newborn nursery, we can make no additional conclusions regarding the effect of high prenatal detection rates on the outcome; nevertheless, prenatal detection is preferable to postnatal detection for a group of highly complex congenital heart patients. Further prenatal detection in Nevada is a result of our program's approach, which includes robust internal data management, simultaneously tracking maternal, fetal, and neonatal information for a regional population, rather than relying on third-party data, such as hospital discharge coding, insurance claims, or other administrative information. From a recent review, the reliance on third-party data is a possible limitation to quality improvement initiatives directed at enhancing prenatal detection of congenital heart disease. 20
In conclusion, stage-1 hybrid palliation may result in excellent surgical outcomes for high-risk 2-ventricle patients with complex congenital heart disease and ductal-dependent systemic circulation. Additionally, high rates of population-wide prenatal detection are possible in this high-risk patient population, allowing prenatal planning and possibly reducing postnatal extremis presentations.
Footnotes
Acknowledgments
This work would not be possible without the contributions of many. The authors first thank the perinatologists and the perinatal sonographers at the following Nevada maternal-fetal-medicine programs: High-Risk Pregnancy Center in Las Vegas and Reno, Desert Perinatal Associates in Las Vegas, UNLV Perinatology in Las Vegas, and Perinatology Associates of Northern Nevada in Reno. Finally, we thank all the fetal cardiologists in Las Vegas and Reno at the Congenital Heart Center Nevada.
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.