
Abstract
Keywords
Introduction
Isolated cleft of the anterior leaflet of the mitral valve—in the setting of otherwise normal mitral valve morphology and normal atrioventricular and ventriculoarterial connnections—is a rare congenital defect. The term “cleft” is used in this setting to describe a triangular separation between two portions of the anterior mitral leaflet. The apex of the cleft is typically oriented toward the left ventricular outflow tract (Figure 1). Isolated cleft of the anterior leaflet of the mitral valve is an entirely different anomaly from the “zone of apposition” that is a feature of the left atrioventricular (AV) valve component of hearts with atrioventricular septal defect (AVSD). That the latter is referred to by some as a “cleft,” may be a source of confusion. But importantly, isolated cleft of the anterior leaflet of the mitral valve is entirely different in terms of both development and orientation from the zone of apposition between the facing surfaces of the left ventricular components of the bridging leaflets of the common AV valve in hearts with partial or complete AVSD. Surgical management of the zone of apposition in the setting of AVSD has been studied and debated extensively. It is however, an entirely separate matter from the subject of this report, the focus of which is isolated congenital mitral valve cleft.
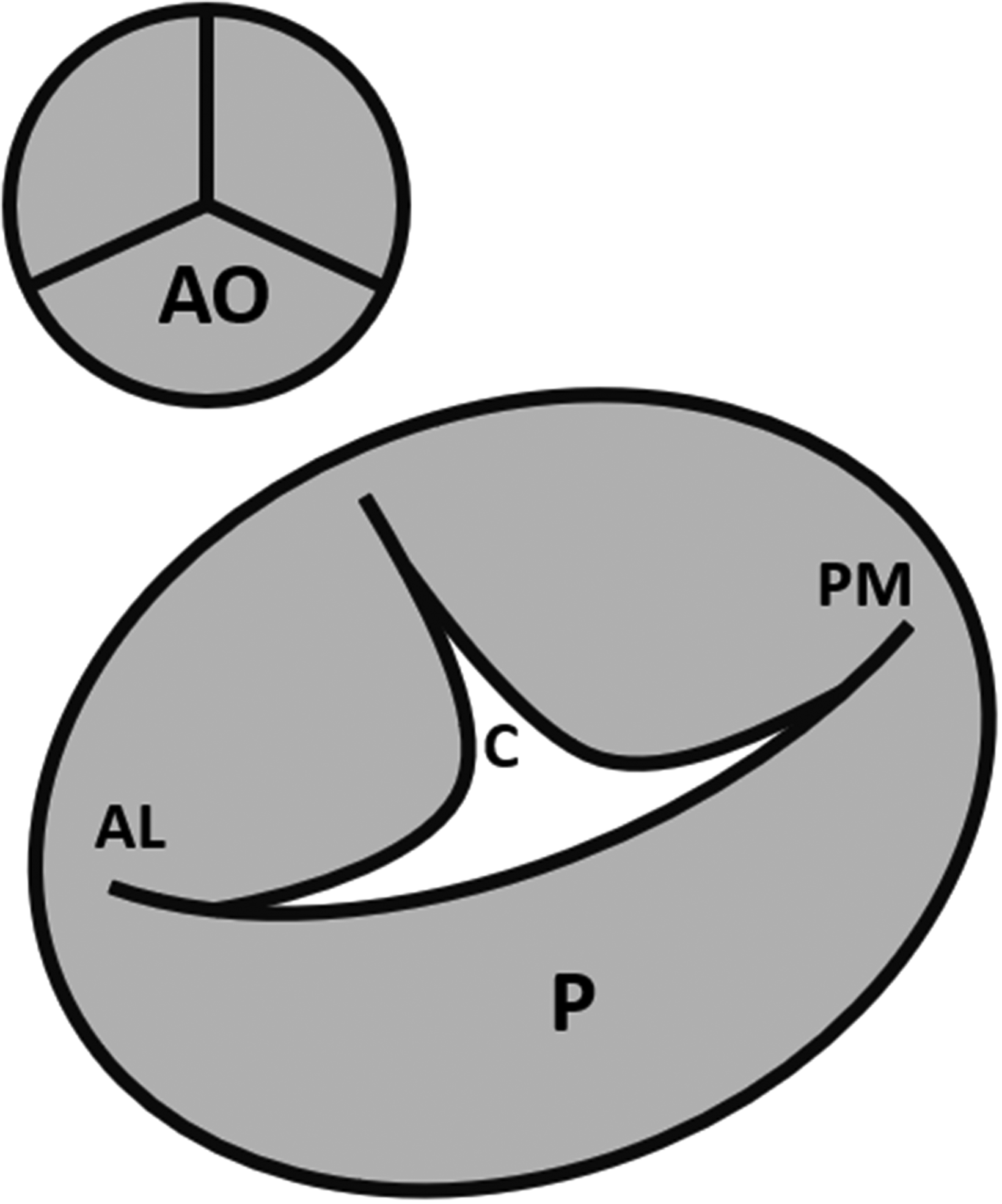
Schematic diagram of the mitral valve demonstrating the location of a typical anterior mitral valve cleft (C). AO, aortic valve; AL, anterolateral commissure; PM, posteromedial commissure; P, posterior leaflet.
In the setting of clinical signs and symptoms of mitral regurgitation (MR), echocardiography is the gold standard for diagnosis of congenital cleft in the anterior mitral leaflet, demonstrating the findings above as shown in Figure 2A. Treatment of isolated congenital clefts depends upon the significance of associated MR. We sought to report our experience with isolated, congenital anterior leaflet clefts and outcomes of surgical repair.
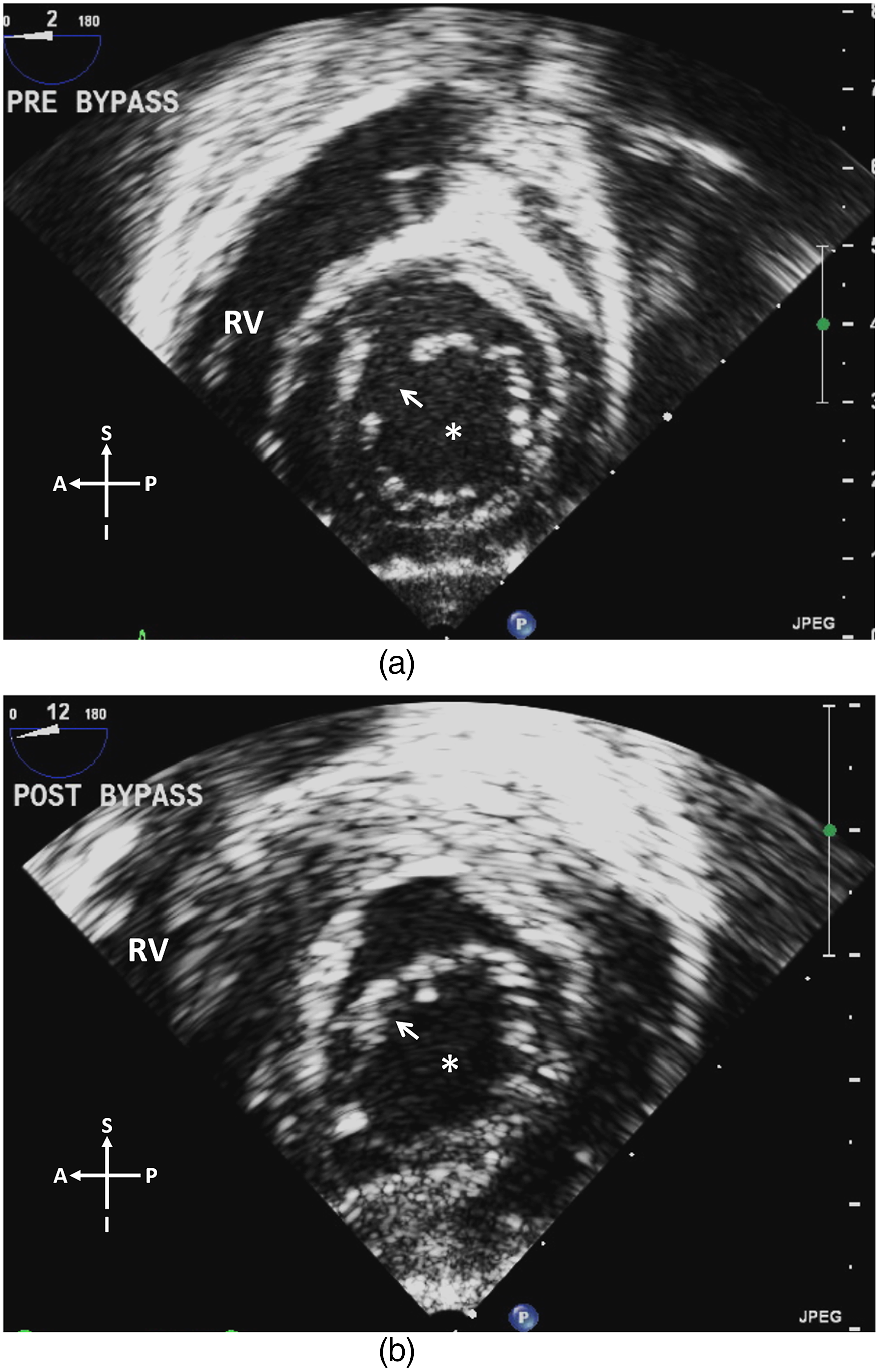
Transesophageal (transgastric) view of a mitral valve cleft (arrow) before (A) and after (B) suture repair. The asterisk denotes the mitral valve orifice. RV, right ventricle; A, anterior; S, superior; P, posterior; I, inferior.
Patients and Methods
We conducted a retrospective review of all patients with an isolated congenital anterior cleft of the mitral valve who were evaluated at Mayo Clinic in Rochester, Minnesota between 1993 and 2020. Acknowledging the fundamental differences between a left AV valve (in the setting of an AVSD) and a true mitral valve, we excluded patients with AVSD from this study. Patients with any additional structural cardiac malformations or defects, were also excluded. The study design was reviewed by the Institutional Review Board and was deemed exempt from patient consent.
Data were collected from electronic and archived paper medical records. Patients were separated into two cohorts: those who underwent surgical repair of the MVC and those who had not undergone surgical repair by the time of data collection. Demographic information was collected from date of initial diagnosis through the most recent available follow–up. Baseline patient characteristics (eg, age, degree of MR, and NYHA functional class) were derived from the last preoperative evaluation (in the case of the surgical cohort) or latest available evaluation (in the case of the nonsurgical cohort).
For the surgical cohort, baseline echocardiographic values were collected from the last presurgical transthoracic (TTE) or nonintraoperative transesophageal echocardiogram (TEE) and from the latest follow-up TTE. For the nonsurgical cohort, echocardiographic data were collected from the most recent TTE. The severity of mitral valve regurgitation (MR) was graded using a standard scale (none/trivial = 0, mild = 1, moderate = 2, moderate-severe = 3, severe = 4). Severity was assigned by the cardiologist reading the study based upon contemporary published American Society of Echocardiography guidelines for assessing MR severity. 1
Operative and perioperative data were collected from operative notes and hospital dismissal summaries. The primary outcome for the surgical cohort was the degree of mitral valve regurgitation at latest follow-up. New York Heart Association (NYHA) functional classes were recorded for all patients as documented in the medical records. If not explicitly reported in the records, classes were assigned by the investigators using NYHA criteria based upon clinical symptoms described in the patient's record.
Pooled quantitative, continuous data are reported as medians (interquartile range [IQR]). Categorical data (eg, MR grade, NYHA class) are reported as median (range). Comparisons were performed using Microsoft Excel analytic software. Pre- and postoperative data were compared using a paired t test. Statistical significance was defined as P < .05.
Results
A total of 22 patients with isolated congenital MVC were identified: 8 patients (5 female) in the surgical cohort and 14 patients (11 female) in the nonsurgical cohort. Baseline data comparing the surgical and nonsurgical cohorts are shown in Table 1.
Baseline Characteristics of the Surgical and Nonsurgical Cohorts.
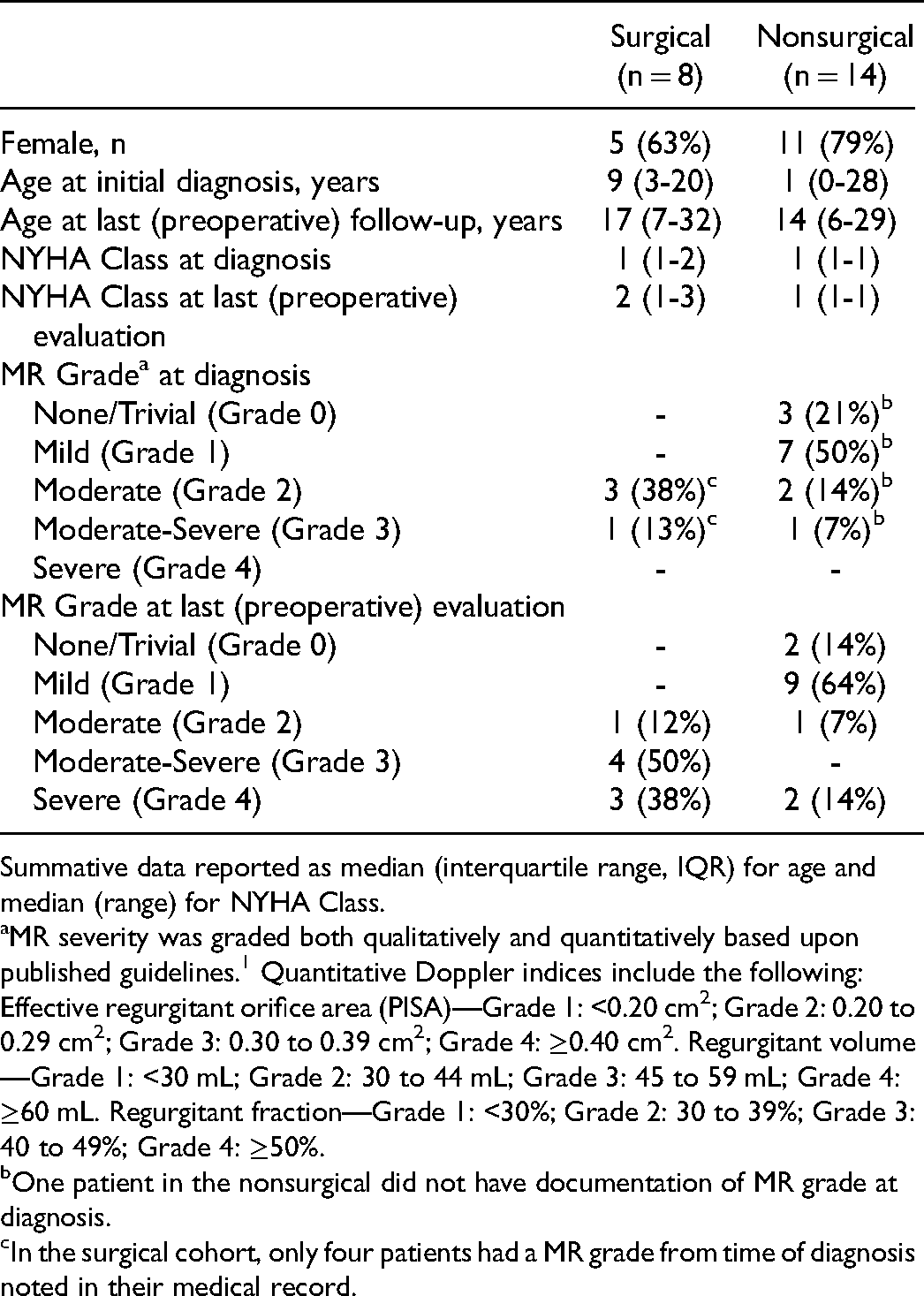
Summative data reported as median (interquartile range, IQR) for age and median (range) for NYHA Class.
MR severity was graded both qualitatively and quantitatively based upon published guidelines. 1 Quantitative Doppler indices include the following: Effective regurgitant orifice area (PISA)—Grade 1: <0.20 cm2; Grade 2: 0.20 to 0.29 cm2; Grade 3: 0.30 to 0.39 cm2; Grade 4: ≥0.40 cm2. Regurgitant volume—Grade 1: <30 mL; Grade 2: 30 to 44 mL; Grade 3: 45 to 59 mL; Grade 4: ≥60 mL. Regurgitant fraction—Grade 1: <30%; Grade 2: 30 to 39%; Grade 3: 40 to 49%; Grade 4: ≥50%.
One patient in the nonsurgical did not have documentation of MR grade at diagnosis.
In the surgical cohort, only four patients had a MR grade from time of diagnosis noted in their medical record.
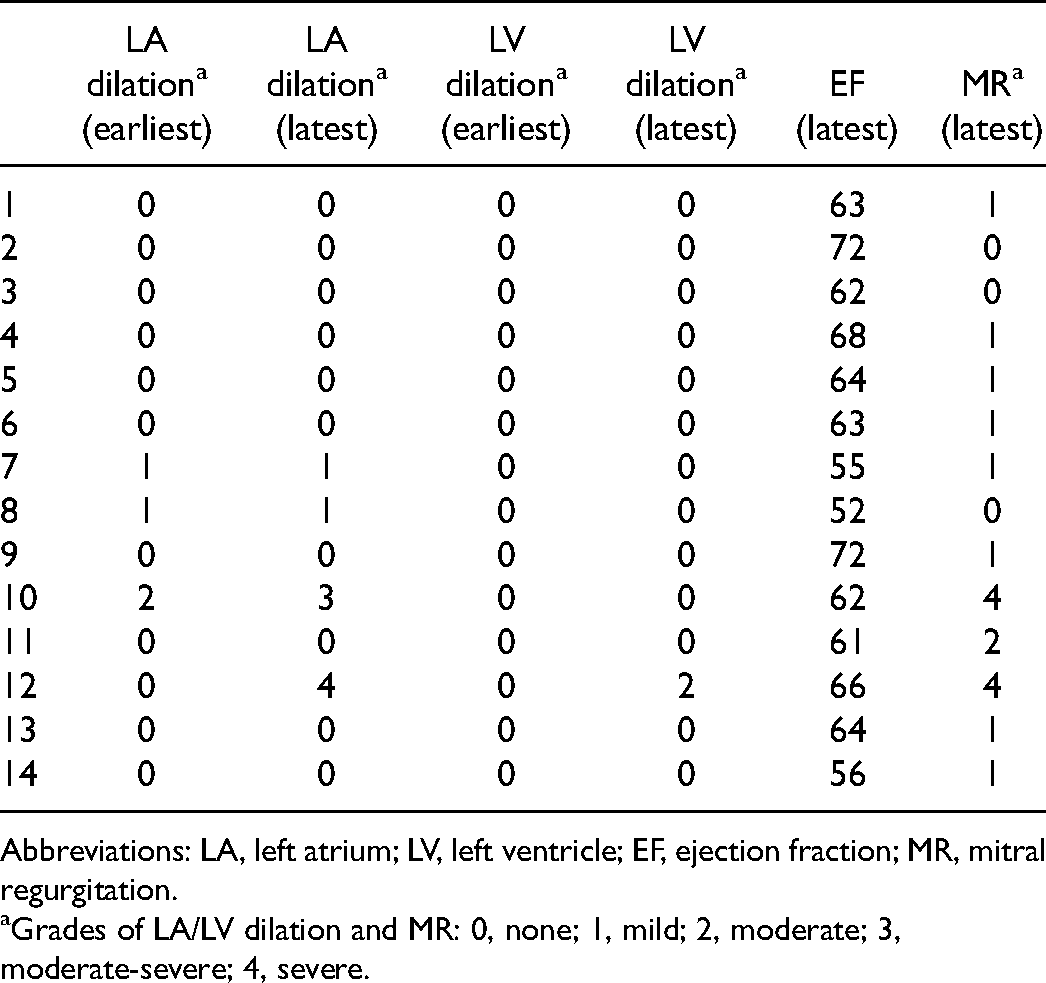
Echocardiographic data and clinical symptoms for the surgical cohort are shown in Table 2. In addition, patients were retrospectively assigned to a class of recommendation (COR) for mitral valve intervention based upon the recent ACC/AHA guidelines. 2 Of note, seven of the eight patients had class 1 or 2a indications for surgical intervention based upon the guidelines for the management of chronic primary MR.
Immediate Preoperative Clinical and Echocardiographic Details of the Surgical Cohort and Indication for Surgical Intervention.
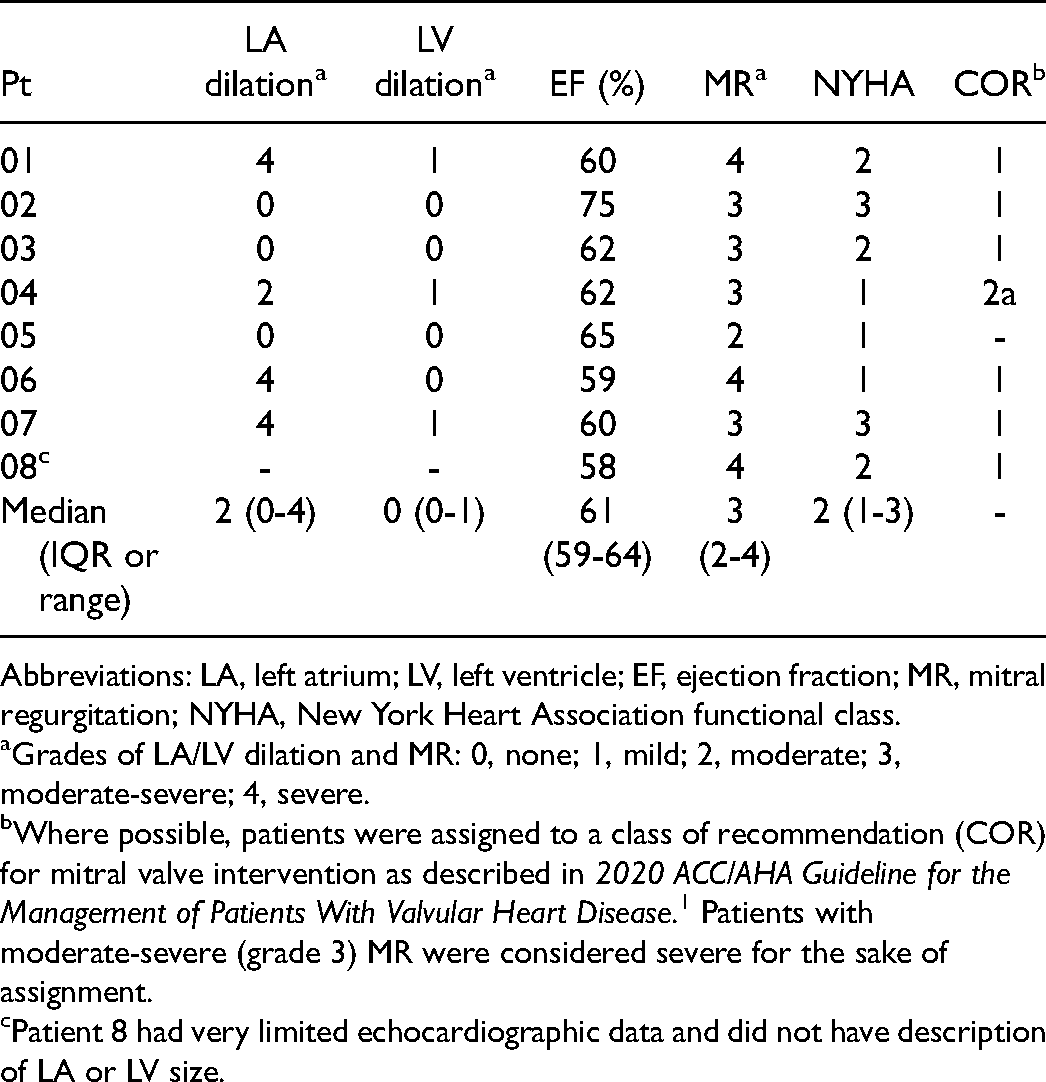
Abbreviations: LA, left atrium; LV, left ventricle; EF, ejection fraction; MR, mitral regurgitation; NYHA, New York Heart Association functional class.
Grades of LA/LV dilation and MR: 0, none; 1, mild; 2, moderate; 3, moderate-severe; 4, severe.
Where possible, patients were assigned to a class of recommendation (COR) for mitral valve intervention as described in 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease. 1 Patients with moderate-severe (grade 3) MR were considered severe for the sake of assignment.
Patient 8 had very limited echocardiographic data and did not have description of LA or LV size.
Median age at time of surgery was 17 (7-32) years (Table 3). Few patients had other significant medical comorbidities. All patients had a left ventricular ejection fraction (LV EF) >55% at time of procedure with a median LV EF of 61% (59%-64%). Median grade of MR was 3.2–4 Surgical approach was either primary median sternotomy (n = 6) or robot-assisted, minimally invasive (n = 2). All cleft repairs were initially performed by simple suture closure (Figure 2). In four patients, testing of the valve after simple suture closure revealed mild persistent MR, necessitating placement of an annuloplasty ring (n = 3) or annuloplasty sutures (n = 1). One patient was noted to have chordal attachments to the left ventricular outflow tract without obstruction did not undergo surgical removal of the attachments. Median bypass time was 57 (37-70) minutes, and median cross-clamp time was 34 (23-51) minutes. Intraoperative mitral valve examination did not reveal additional structural factors that could account for the MR except for the MVC.
Characteristics and Outcomes of Patients Undergoing Surgery for Isolated Mitral Valve Cleft.
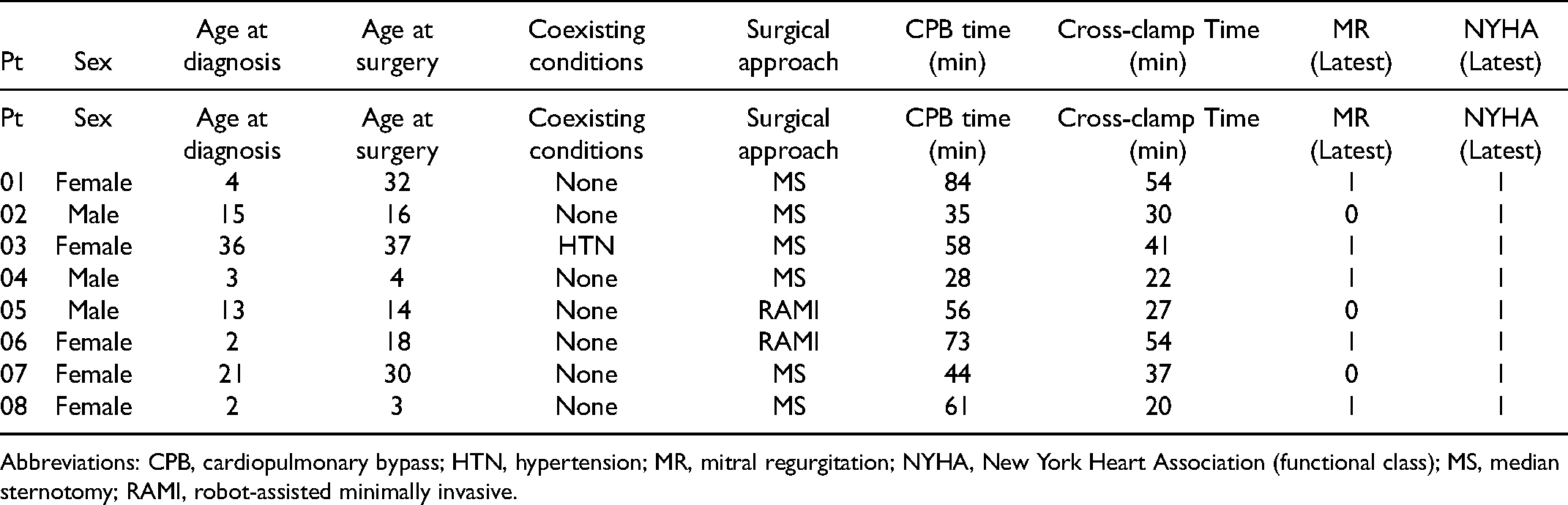
Abbreviations: CPB, cardiopulmonary bypass; HTN, hypertension; MR, mitral regurgitation; NYHA, New York Heart Association (functional class); MS, median sternotomy; RAMI, robot-assisted minimally invasive.
There was an insignificant decrease in median LV EF at time of hospital discharge to 58% (47%-64%). As expected, there was a significant, immediate improvement in median grade of MR to 0 (0-1) after surgery (P < .001). Median hospital stay was 4.53–7 days. There were no major adverse events and no operative mortality in the immediate and early postoperative period.
Upon review of the patients in the surgical cohort, the most common indication for repair was an increase in MR grade (n = 7). The other patient in the surgical cohort was asymptomatic with grade 2 (moderate) MR at the time of repair. The impetus for pursuing surgery was their desire to preemptively repair the cleft rather than to relieve any symptoms or to correct high-grade MR.
Follow-Up
Among the nonsurgical cohort, median follow-up time after initial diagnosis was 5 (0-12) years. At latest follow-up, no patients exhibited symptoms (NYHA Class 1). The median MR grade among this group was 11–4; one patient had grade 2, and two had grade 4 (Table 4). Additionally, two patients were noted to have Wolff-Parkinson-White (WPW) syndrome. At the time of our study, one of these patients with grade 4 MR had been advised to undergo surgical repair, driven mainly by the presence of WPW-related supraventricular tachyarrhythmias. As of October 2021, however, the patient had deferred surgical intervention.
Nonsurgical Cohort Echocardiographic Details at Earliest and Most Recent Clinical Evaluations for Mitral Valve Cleft.
Abbreviations: LA, left atrium; LV, left ventricle; EF, ejection fraction; MR, mitral regurgitation.
Grades of LA/LV dilation and MR: 0, none; 1, mild; 2, moderate; 3, moderate-severe; 4, severe.
Among the surgical cohort, median duration of follow-up after mitral valve repair was 8.51–14 years. During that time, no patients underwent additional mitral valve intervention. At latest follow-up, the median grade of MR was 1 (0-1), and median LV EF was 65% (59%-67%), both similar to the immediate postoperative result. All patients were asymptomatic (NYHA Class 1) with no documented arrhythmias.
Comment
Isolated MVC is a rare congenital anomaly.3,4 Most published reports about the surgical management of isolated MVC have been comprised of case reports or small case series.5–15 Larger series have consisted of postmortem studies or have included patients who have additional cardiac defects.16–19 An early, small surgical case series reported repair of isolated MVC via direct suturing or a pericardial patch in four patients. 20 All patients in our surgical cohort underwent suture repair of the MVC, irrespective of surgical approach (median sternotomy or robot-assisted minimally invasive), similar to more recent series.16,21 In addition, four patients required a partial or complete annuloplasty due to persistent incompetence after suture repair. Annuloplasty has been described as an adjunct to valve repair in prior series as well, with more recent reports describing its use less frequently than older reports.16,20
In general, surgery was performed to address a high grade of MR. Most patients had grade 3 or 4 MR on their last evaluation preoperatively. Although not our standard practice, one patient underwent elective repair of MVC with asymptomatic, grade 2 (moderate) MR (Table 3, patient 5
Some patients in our surgical cohort underwent MVC repair more than 10 years after initial diagnosis, while others underwent elective repair soon after diagnosis. The small number of patients and the heterogeneity of surgical timing limits our ability to draw conclusions about “optimal” timing of MVC repair from this group. By comparison, though, the patients in our nonsurgical cohort had similar follow-up duration without significant decline in mitral valve competence or change in functional capacity. These results suggest that incidentally found MVC does not necessarily require surgical repair, although we acknowledge that repair may eventually be indicated for some patients.
Considering these findings, we recommend that the decision to repair isolated MVC be driven by clinical status and severity of MR, rather than by the presence or appearance of the mitral cleft itself. Asymptomatic patients with MVC and moderate or less (grade 1-2) MR should be monitored longitudinally for progression of M.As noted above, two patients in our “non-surgical” cohort had not yet undergone surgical repair despite having severe (grade 4) MR. Despite these outliers, our practice is to advise repair of symptomatic (COR 1) or asymptomatic (COR 2a) high grade MR, consistent with current ACC/AHA guidelines for the management of chronic primary M.
Limitations
Due to our reliance on available medical records for this retrospective review, this report is limited by the accuracy of those data. Given the small number of patients included, our ability to apply these findings to larger, more diverse cohorts of patients is limited. We also recognize that the demographics of the patients presented herein may not represent that of the general population. As such, our data should not be interpreted to imply a natural history of MVC. In addition, our report focused on isolated MVC without additional cardiac defects. The presence of other complicating defects, such as left ventricular outflow tract obstructive lesions or ventricular septal defects will necessarily affect the indications for surgical intervention. We do not suggest that the same approach to management of MVC should be taken in such patients.
Conclusions
Durable surgical repair of isolated, congenital MVC can be performed safely in select patients. The decision to intervene should be based on the severity of mitral regurgitation and patient symptoms rather than the identification of the MVC alone.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.