
Abstract
Background:
Long-term morbidity and mortality outcomes of the arterial switch operation (ASO) in patients with transposition of the great arteries and Taussig-Bing anomaly are excellent. With an increasing number of patients reaching adolescence and adulthood, more attention is directed toward quality of life. Our study aimed to determine the health-related quality of life (hrQoL) outcomes in patients after the ASO and identify factors influencing their hrQoL.
Methods:
In this cross-sectional study, hrQoL of patients after ASO was assessed with the German version of the Short Form-36 (SF-36) and the potential association of specified clinical factors was analyzed. Patients of at least 14 years of age who underwent ASO in our institution from 1983 were considered eligible.
Results:
Of the 355 questionnaires sent to eligible patients, 261 (73%) were available for analysis. Compared to the reference population, patients who had undergone ASO had a significantly higher score in all subscales of the SF-36 except for vitality (P < .01). Patients with an implanted pacemaker (P = .002), patients who required at least one reoperation (P < .001), and patients currently taking cardiac medication (P < .004) or oral anticoagulation (P = .036) had lower physical component scores compared to patients without these factors.
Conclusions:
Patients’ self-assessed and self-reported hrQoL after ASO (using German version of the Short Form 36) is very good. In this population, hrQoL is influenced by reoperation, the need for a pacemaker, and current cardiac medication or anticoagulant use. The development of strategies designed to mitigate or minimize the requirements for, and/or impact of these factors may lead to better hrQoL in this patient population.
Keywords
Introduction
The arterial switch operation (ASO) is the treatment of choice for newborns with transposition of the great arteries (TGA), yielding excellent morbidity and mortality outcomes. 1,2 Reoperation rates range between 10% after three years 3,4 and 20% after ten years. 5 –7 With increasing numbers of patients surviving ASO and reaching adulthood, attention is increasingly directed at quality of life outcomes.
Only a few health-related quality of life (hrQoL) studies focus on patients with congenital heart disease (CHD), and data describing hrQoL in adults after ASO are scarce. 8 Furthermore, objective assessments such as exercise testing do not correlate sufficiently with subjective findings of hrQoL, nor do external judgments by friends or family members. 8,9 Nevertheless, some factors influencing quality of life in children and adults with CHD have been identified, including socioeconomic status, physical status, amount of emotional support, and level of anxiety. 10,11 In particular, psychosocial factors seem to have extensive relevance, 12 but cardiopulmonary function is also essential. 13 For patients who have undergone ASO, no factors affecting hrQoL have previously been identified. This study aimed to analyze hrQoL in patients after ASO compared with a reference population and to identify morphological and surgical factors influencing hrQoL in patients after ASO.
Methods
The trial was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the institutional review committee of the Technical University of Munich, and informed consent was taken from all individual participants. For all patients younger than 18 years, written informed consent of the parents was obtained.
Patient Population
This single-center, cross-sectional study included all patients who underwent an ASO since 1983 at the German Heart Center in Munich and were at least 14 years old at the time of the study. We identified the patients from the departmental database, and German language self-completion questionnaires were sent by mail. Patients younger than 18 years of age were asked to fill out the questionnaire with the help of an adult if required. Patients living in a non-German-speaking foreign country and patients who did not return the questionnaire after three requests were excluded. All patients underwent yearly follow-up at our outpatient clinic or with their referring pediatric cardiologist. All medical reports, including reoperation and medication data, were reviewed. The following clinical factors were drawn from the latest medical report and were analyzed: the type of TGA (with or without ventricular septal defect), Taussig-Bing anomaly, associated anomalies (aortic arch obstruction and coronary artery anomaly), need for major cardiac reoperation, residual (at least moderate) pulmonary stenosis, residual (at least moderate) aortic regurgitation, current NYHA (New York Heart Association) classification, left ventricular function, history of rhythm disturbances and implanted pacemaker systems, and need for anticoagulation or other current cardiac medication.
Health-Related Quality of Life Questionnaire
Health-related quality of life is a multimodal construct, including the physical, mental, and social well-being of an individual. 14 Instruments measuring hrQoL contain categories focusing on health status, as well as categories representing the quality of life. 15
In this study, hrQoL was assessed with the German version of the Short Form-36 (SF-36), a validated and standardized questionnaire first introduced in the 1990s. 16 –19 The SF-36 consists of eight subscales containing 36 items that cover different aspects of hrQoL representing physical functioning (the extent of limitation in performing every day physical activities), role function physical (the extent of limitation in participating in daily activities, such as work), bodily pain (the extent of limitation in daily activities due to pain), general health perception (personal evaluation of the current health status), vitality (feeling energetic versus feeling worn out), social functioning (the extent of limitation due to physical or emotional problems on social activities), role functioning emotional (the extent of limitation of daily activities due to emotional problems), and mental health (perception of mental health; Supplemental data). The subscales are converted into values of 0 to 100 for evaluation and comparison between groups. 16 –20 Furthermore, there is the possibility to calculate two component scores from the subscales. The physical component score (PCS) contains the first four of the mentioned subscales, the mental component score (MCS) the lesser four. 16
For this study, SF-36 subscales and component score values of all patients were calculated and compared to age- and gender-matched samples of a German reference population collected during the SF-36 scoring process. 16 Every individual score was matched with the adjusted age and gender-matched reference, redefining the reference score as 100. All scores are presented in percentage of the individual age and sex-adjusted reference value (%pred), with scores less than 100 indicating a worse hrQoL, and scores over 100 indicating a better hrQoL compared to the reference group. Additionally, the potential association of abovementioned clinical factors on the component scores of the SF-36 was statistically analyzed.
Statistical Analysis
Statistical analysis was performed using SPSS 22.0 software (IBM SPSS, IBM Corp). Frequencies are expressed as absolute numbers and percentages. All metric variables were tested with the Kolmogorov-Smirnov test for normal distribution. None were normally distributed (Kolmogorov-Smirnov test: P < .05), and therefore values are presented as medians and the divergence as quartiles.
Subscales and summary scales of the SF-36 were compared to age- and gender-matched controls of the German reference population published in 1998 by Bullinger and Kirchberger by the Wilcoxon signed-rank test. 16
Comparisons between groups were calculated with the nonparametric Mann-Whitney U and the Kruskal-Wallis tests. Two-sided significance testing was performed for all tests, with P values less than .05 considered being significant.
Results
Patient Characteristics
During the study period, 688 patients underwent an ASO at our institution. After exclusion of 243 patients younger than 14 years, 10 patients living in a non-German-speaking country, and 41 patients who had died, the SF-36 questionnaire was sent to 355 patients. A total of 261 (73%) questionnaires were available for analysis. The baseline characteristics of the participating patients are provided in Table 1.
Patients’ Baseline Characteristics After ASO.a,b
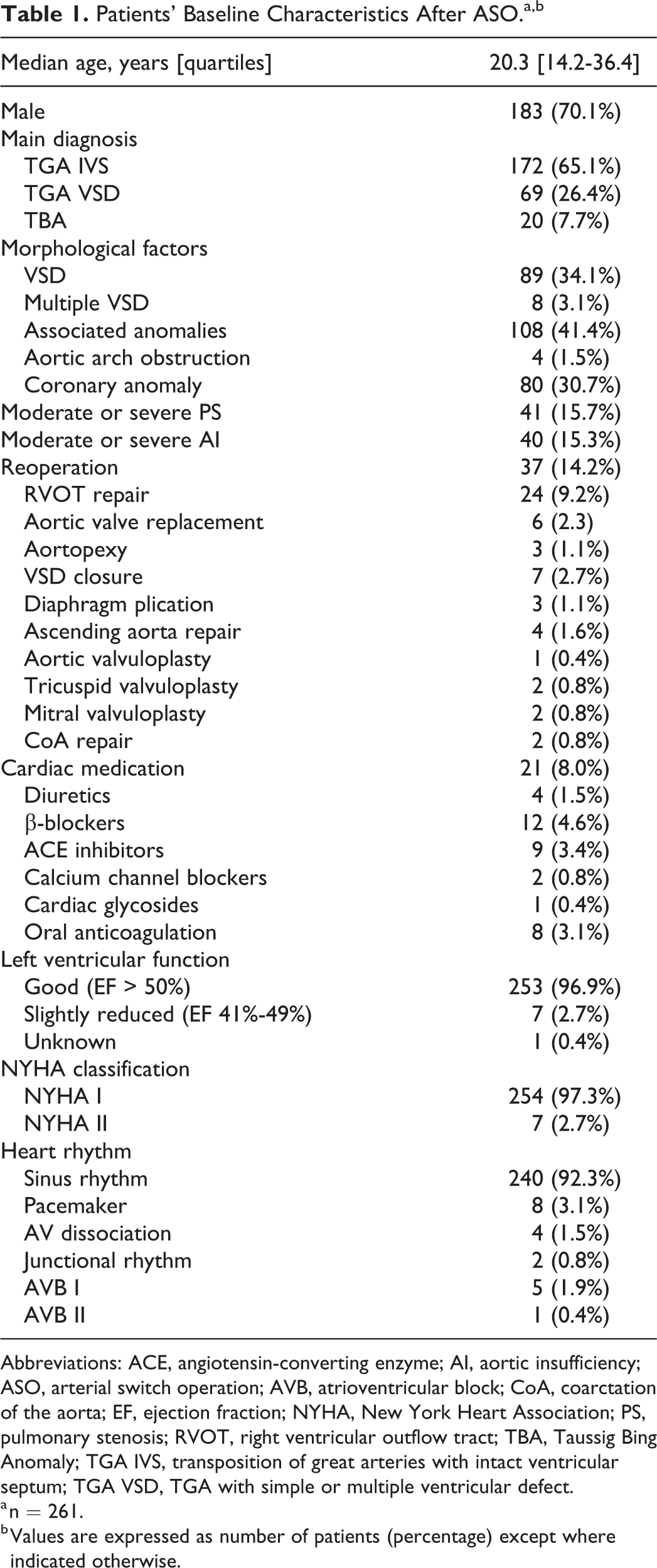
Abbreviations: ACE, angiotensin-converting enzyme; AI, aortic insufficiency; ASO, arterial switch operation; AVB, atrioventricular block; CoA, coarctation of the aorta; EF, ejection fraction; NYHA, New York Heart Association; PS, pulmonary stenosis; RVOT, right ventricular outflow tract; TBA, Taussig Bing Anomaly; TGA IVS, transposition of great arteries with intact ventricular septum; TGA VSD, TGA with simple or multiple ventricular defect.
a n = 261.
b Values are expressed as number of patients (percentage) except where indicated otherwise.
Health-Related Quality of Life
Analysis of the subscales and component scores of the SF-36 showed following results: physical function (%pred) 103.94 [IQR: 99.15-104.37], role physical (%pred) 104.36 [IQR: 101.74-107.54], bodily pain (%pred) 108.98 [IQR: 108.98-112.47], general health (%pred) 112.81 [IQR: 93.36-120.83], vitality (%pred) 96.02 [IQR: 75.45-111.08], social functioning (%pred) 106.18 [IQR: 93.96-107.39], role emotional (%pred) 105.86 [IQR: 105.36-105.86], mental health (%pred) 105.92 [IQR: 91.73-117.50], PCS (%pred) 104.35 [IQR: 101.01-106.86], and MCS (%pred) 105.33 [IQR: 94.16-113.24].
Compared to the reference population, patients who underwent ASO had a significantly higher percentage of predicted scores in the SF-36 in all categories except for vitality (P < .01). Results are shown in Figure 1.
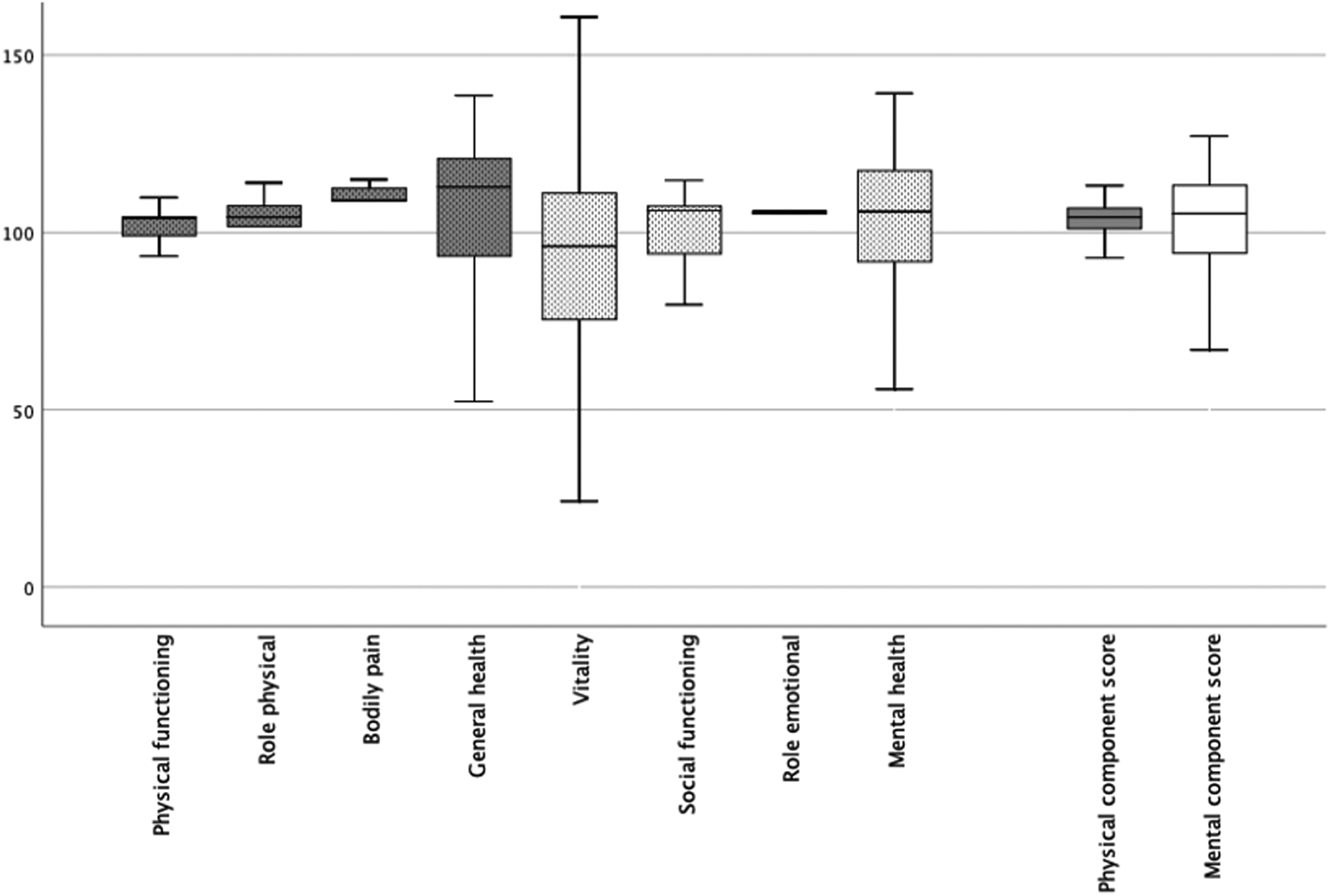
Boxplots showing the Short Form-36 (SF-36) scores (%pred) and component scores (%pred), the grey dotted subscales are represented in the physical component score, the white dotted subscales are represented in the mental component score.
Parameters Affecting SF-36 Scores
Of the analyzed clinical parameters, we found multiple parameters that are affecting hrQoL. Patients who required at least one reoperation had a lower PCS (%pred) compared to patients without reoperation (102.5 [IQR: 94.1-104.2] vs 104.7 [IQR: 101.4-107.0], P < .001). Furthermore, lower PCS (%pred) were observed in patients currently taking cardiac medication or oral anticoagulants (100.9 [IQR: 86.3-105.0] vs 104.6 [IQR: 101.5-106.9], P < .004 and 101.7 [IQR: 94.1-103.5] vs 104.4 [IQR: 101.3-106,9], P = .036), respectively. Also, patients with an implanted pacemaker had a significantly lower PCS (%pred) (91.2 [IQR: 81.4-101.9] vs 104.5 [IQR: 101.4-106.9], P = .002; Figure 2).
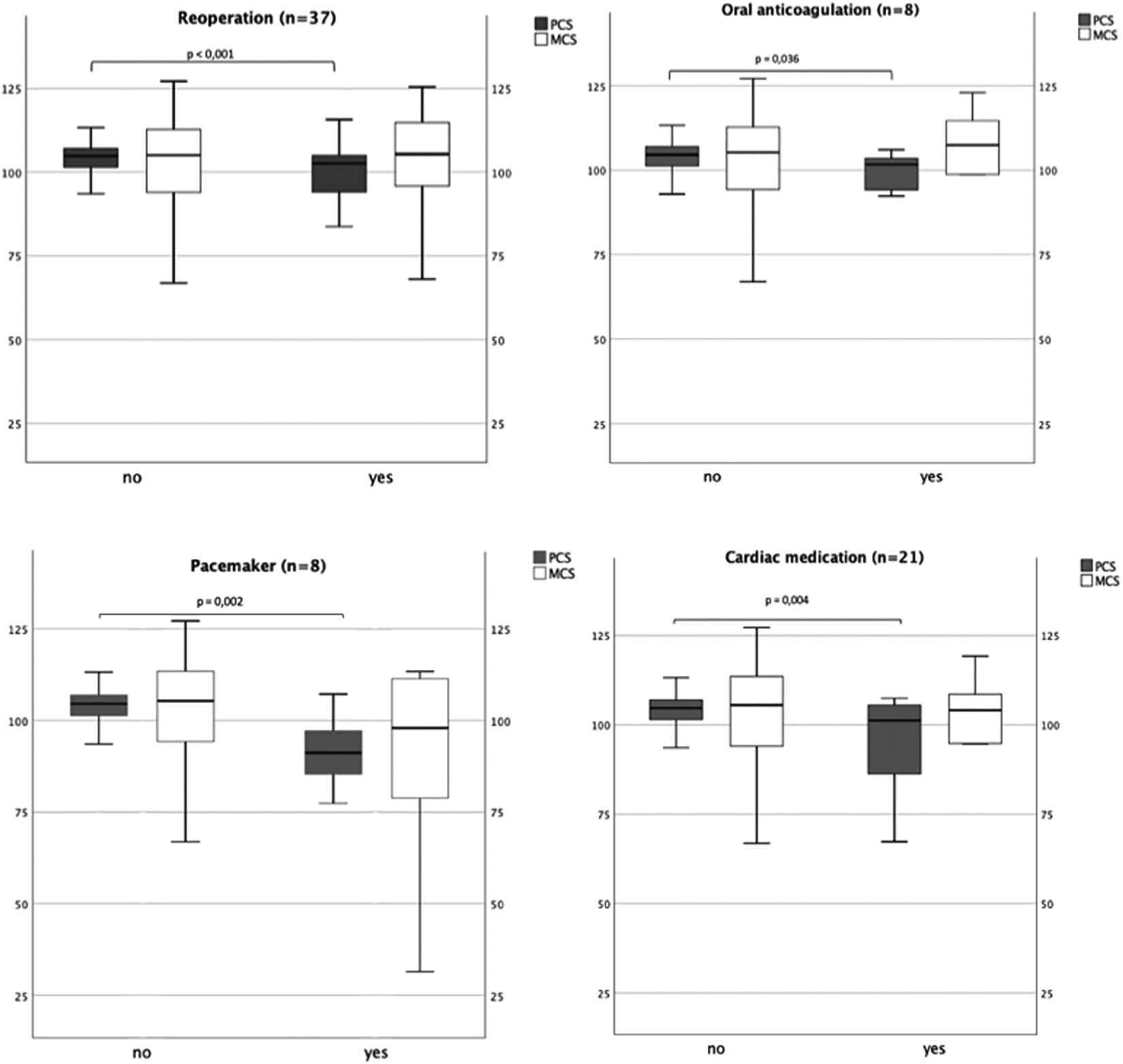
Boxplots showing the association of clinical parameters on the physical component score (PCS).
The only parameter having a significant effect on the MCS was the NYHA classification. Patients in NYHA class II had a lower MCS (%pred) compared to patients in NYHA class I (64.5 [IQR: 49.1-85.6] vs 105.9 [IQR: 94.5-113.5], P < .001; Figure 3). All other parameters such as gender, diagnosis group, associated anomalies, coronary anomalies, and left ventricular function had no significant effects on PCS or MCS (Table 2).
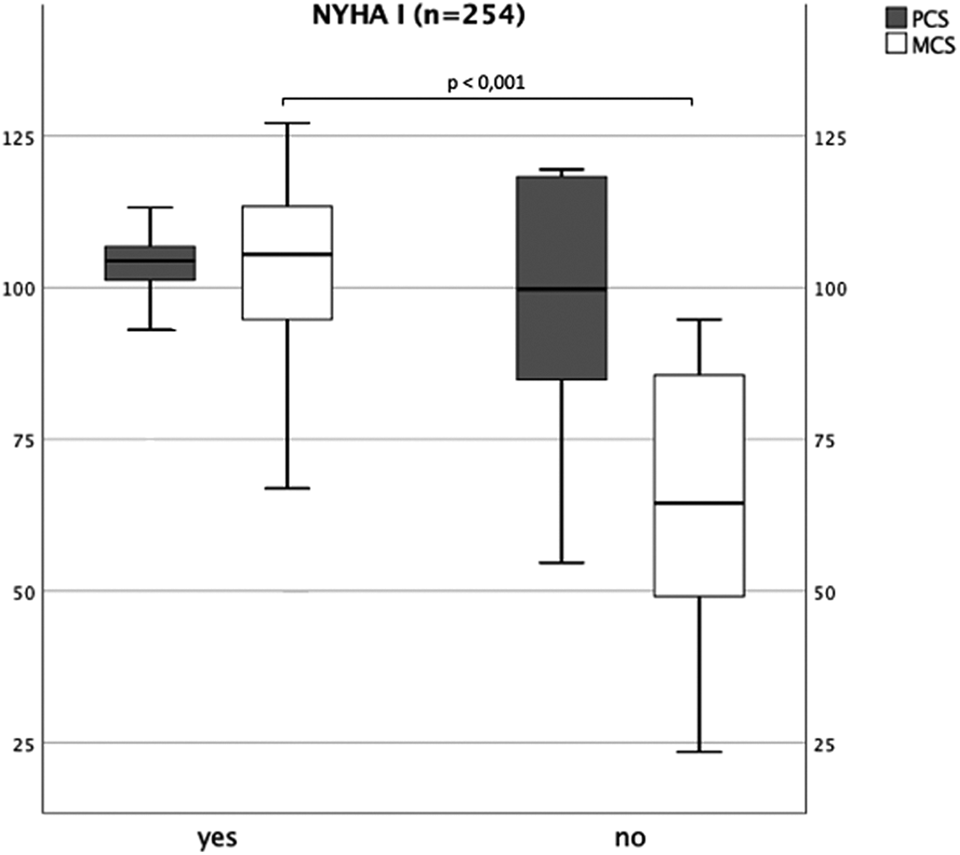
Boxplot showing the association of New York Heart Association (NYHA) classification on the mental component score (MCS).
Association of Clinical Parameters on Physical Component Score and Mental Component Score.a
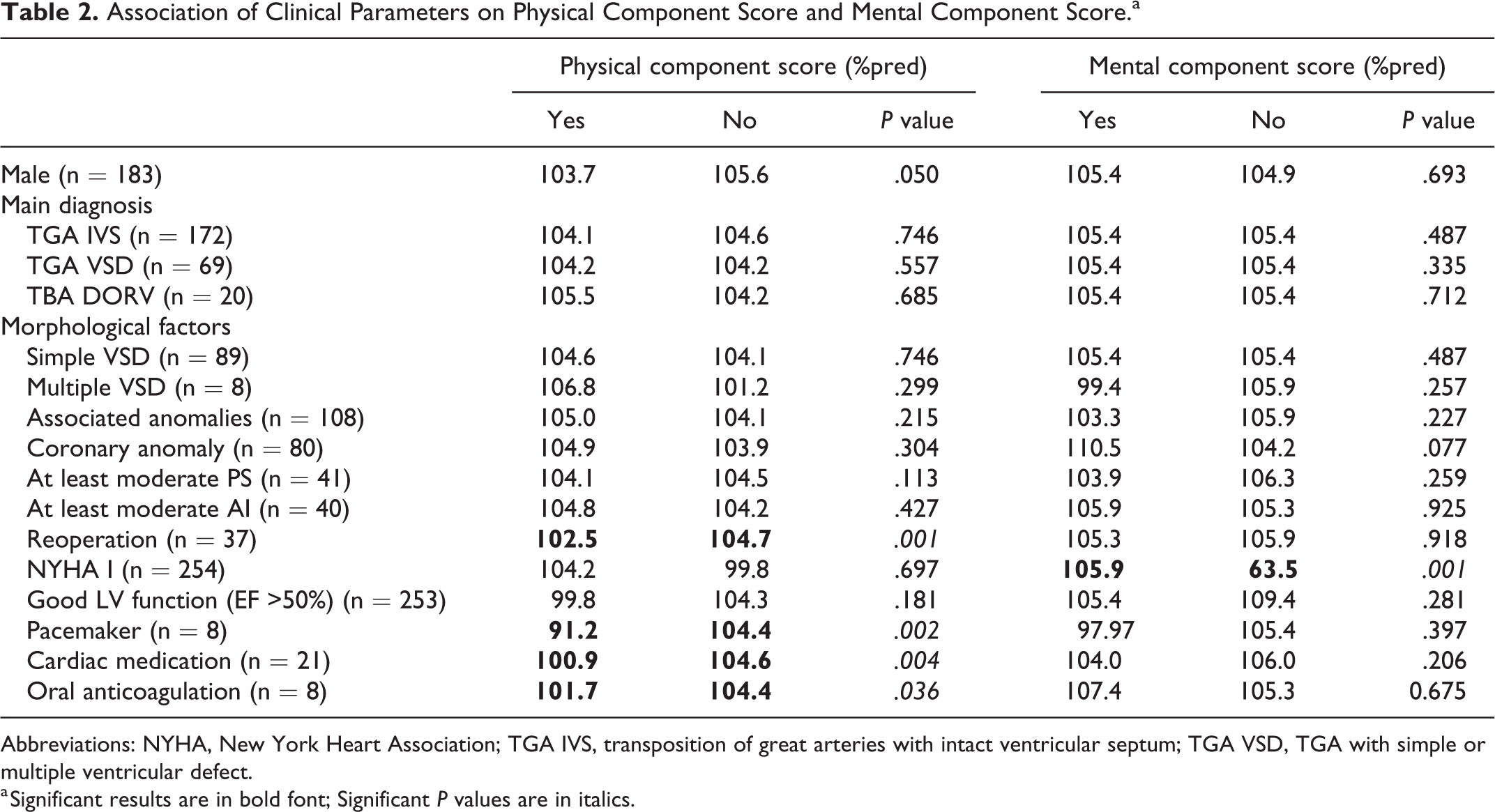
Abbreviations: NYHA, New York Heart Association; TGA IVS, transposition of great arteries with intact ventricular septum; TGA VSD, TGA with simple or multiple ventricular defect.
a Significant results are in bold font; Significant P values are in italics.
Comment
In this study, we showed that patients who have undergone ASO have a very good hrQoL, scoring higher than the reference population in all categories except vitality. Further, we identified that reoperation, an implanted pacemaker, and the need for regular medication were associated with a lower physical hrQoL, whereas a higher NYHA class was associated with a lower mental hrQoL.
Several studies confirm a high hrQoL in patients with corrected CHD, reporting a satisfactory overall hrQoL. 1,8,14,20 –22 As TGA is considered a complex CHD, it is notable to consider that some authors describe a worse hrQoL for complex CHD. 14,23,24 However, other studies could not show a correlation between hrQoL and the complexity of the CHD. 25,26 Moons et al conclude that the hrQoL is more associated with the functional status of the individual than with the severity of the CHD. 25 Indeed, complex CHD showed especially low scores for physical functioning and functional status in different studies, resulting in a worse hrQoL for this patient group 13,23,24,27
What limits the comparability of these studies to ours is a high variability in the included complex CHDs, with different surgical procedures performed that might have progressed over the years. Patients with TGA and especially after ASO are scarcely represented in those studies. Kamphuis et al, for example, included only 44 patients with TGA in their study, of which only one patient had an ASO. 23 Lane et al included 21 patients with TGA, of which none received an ASO. 23,24 A recent cross-sectional study included 356 patients with TGA showing the best outcomes for the PCS in complex CHD, although scores were below values of 100, which is worse than the patients in our study. Unfortunately, the type of TGA and the kind of treatment of the patients are not described in the study, which makes a comparison difficult. 27
Several studies assessing hrQoL in patients with TGA could demonstrate very good results in accordance to this study. Both Culbert et al and Müller et al showed excellent hrQoL for patients with TGA after different types of procedures with better scores than the reference population. Moreover, both studies showed very good physical functioning scores. In both studies, patients after ASO had significantly higher scores for hrQoL and physical functioning than patients after other procedures. 21,28
Although comparative data are sparse, patients after ASO seem to stand out from the pool of other complex heart diseases and might not be represented adequately in studies comparing different types of CHD instead of comparing procedures.
Some authors have associated a high hrQoL in patients with corrected CHD with the sense of coherence, 8,29 which describes a mechanism for helping a person handle challenging circumstances and deal positively with them. Patients with TGA live with their condition from the beginning of their consciousness and grow up with limitations that they must integrate into their social life. 30
In our study, we observed that patients scored higher in the subscale “bodily pain” compared to the other subscales. This corresponds to the results of a study reported by Lane et al, who observed that patients with corrected CHD had better scores for bodily pain than the reference population. 24 Accordingly, patients achieved significantly higher scores for bodily pain in a study reported by Vigl involving over 700 patients with CHD. 20 Vigl et al speculated that patients with CHD, a chronic disease, have a variant perception of “normal” and might have an altered and higher threshold for pain. 20 Another explanation is based on the presumption that a CHD does not cause pain, while individuals of the reference population may not all be healthy and might very well experience more pain than patients who have undergone ASO.
After assessing hrQoL after ASO, identification of influencing factors may improve the delivery of the best possible aftercare and support. Notably, in this study preoperative conditions, such as the diagnosis group (TGA with or without VSD and Taussig-Bing anomaly), as well as associated cardiac and coronary anomalies had no impact on hrQoL. This might seem surprising in the first place, as a previous study reported that main diagnosis groups are linked to objective outcome parameters such as early mortality or the occurrence of aortic insufficiency in patients undergoing ASO. 2 Additionally, patients with a complex TGA or a VSD are more prone to reoperation or pacemaker implantation, having a significant influence on the PCS. A recent study showed that complex TGA is a risk factor for right ventricular outflow tract obstruction, which is the most common indication for reoperation after ASO. 31,32 However, as mentioned above, the complexity of the condition is not the most influential factor on hrQoL. 25,26 For further statements, a more detailed analysis would be required. Due to the low number of patients affected, a multivariate regression analysis was not suitable for this study. Patients who require reoperation and patients taking cardiac medication are subjected to frequent medical visits, which could affect their hrQoL. Current cardiac medication has been shown to have a negative impact on hrQoL in children and adolescents with CHD. 13,14 Dependency on medication may especially affect children and young adults, as spontaneous activities are limited, and side effects may alter the individual’s sense of well-being.
In this study, a higher NYHA class than I was associated with a worse mental hrQoL, represented in the MCS. These results are consistent with those of a previous study involving 218 CHD patients, showing lower scores for the MCS for NYHA class over I. 13 Although physical limitations seem to be linked to physical well-being, these results show that they also have a significant impact on emotional quality of life after ASO. Limited participation in physical activities with friends and peers obviously creates significant emotional distress.
To support hrQoL after ASO, it is important to address the special needs of patients with a pacemaker, cardiac medication requirements, and lower functional status. Patients who need reoperation should receive extensive support and rehabilitation to help with recovery and improving their functional status and reintegrate them as soon as possible in their social environment. To reduce medical visits for patients receiving anticoagulants, self-management of the international normalized ratio has been shown to be an effective option for patients of all ages in previous studies. 33,34
The presence of a strong sense of coherence has been related to a better quality of life in children with chronic disease. Caregivers have an important role in promoting sense of coherence in patients after ASO by educating patients and encouraging them to address their health issues actively. 30 As social support is known to influence and improve quality of life, outpatient models for self-management and self-support could combine education and active exchange among patients. Those models have been primarily developed for senior patients with chronic conditions but may be adapted to the needs of younger patients after ASO. 35,36
Limitations
With this study being a single-center study, the number of patients is limited. Especially for a more detailed analysis of influencing factors, larger case numbers are necessary. The scores in this study were compared to age- and gender-matched values of the reference population to reduce bias. However, the reference population for the German SF-36 was questioned in the year 1998, which can be a limiting factor as we don’t know if the health status and the hrQoL of the population have changed over time. Nevertheless, as the values of the reference population are being used in several studies using the SF-36, it can also bring consistency. Lastly, although a response rate of almost 75% is satisfactory, there is the possibility of a nonresponder bias.
Conclusion
Patients’ self-assessed and self-reported hrQoL after ASO (using German version of the Short-Form 36) is very good. Although TGA is considered a complex anomaly, patients after ASO reported high scores for physical functioning. Health-related quality of life in this population appears to be negatively influenced by reoperation, the need for a pacemaker, and current cardiac medication or anticoagulant use. Caregivers should actively support and educate patients and their parents to help them manage these clinical burdens. In addition, the development of strategies designed to mitigate or minimize the requirements for, and/or impact of these factors may lead to better hrQoL in this patient population.
Supplemental Material
Supplemental Material, sj-docx-1-pch-10.1177_2150135121990651 - Factors Affecting Health-Related Quality of Life After the Arterial Switch Operation
Supplemental Material, sj-docx-1-pch-10.1177_2150135121990651 for Factors Affecting Health-Related Quality of Life After the Arterial Switch Operation by Julie Cleuziou, Anna-Katharina Huber, Martina Strbad, Masamichi Ono, Alfred Hager, Jürgen Hörer and Rüdiger Lange in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Authors’ Note
J.C. and A-.K.H. contributed equally to the manuscript.
Acknowledgment
The authors thank Dr. Med. Tanja Kottman (Clinical Research Organisation, Hamm Germany) for assistance with the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.