
Abstract

In this issue of the World Journal for Pediatric and Congenital Heart Surgery, Bryan and coworkers from Stanford report results of mechanical testing of cadaver porcine aortic, pulmonary and “neoaortic,” or “autograft” roots using a “left heart simulator.” 1 They constructed the neoaortic roots by suturing porcine coronary button tissue into 2 of the pulmonary root sinuses, then suturing a cuff of aortic tissue to the distal portion of the pulmonary root, thus mimicking the Ross root. They subjected roots to 30 min of simulated left heart pressures, during and after which they measured a few solid and fluid mechanical characteristics. The authors found some abnormalities they felt could contribute to the long-term complications associated with the Ross autograft.
Multiple studies over the past 20 years have reported a concerning incidence of failure of the unsupported Ross autograft. In a study by Kumar and coworkers of 316 patients undergoing the Ross procedure, 47 patients (15%) required autograft reintervention a median of 5.5 years after the Ross procedure, 20 primarily for valve failure and 27 for root dilation. 2 Recently, Bove and coworkers reported on 137 patients undergoing Ross (110) or Ross-Konno (27) operation. Fourteen patients required autograft-related reoperation at a median interval of 14 years; 2 primarily for valve failure and 12 for root dilation. 3 Pettersson and coworkers reported 60 reoperations after the Ross procedure, 32% for valve failure and 53% for root or ascending dilation. 4 Clearly, because valve failure can occur without root dilation, the root and valve are in part independently susceptible.
It is presumed that this intermediate and late failure is most frequently caused by “maladaptive” remodeling of the autograft root (aortic wall) and leaflet tissue in response to flow at systemic pressure over time. This process is likely exacerbated by the presence of a vasculopathy such as that present in congenital bicuspid aortic valve (BAV) patients (a common reason for performing the Ross operation). After the Ross in these patients, “neo-” aortic insufficiency (AI) is commonly secondary to autograft dilation at the sinutubular junction (STJ). Preoperative predominant AI and ascending aortic enlargement also appear to be risk factors for autograft dilation. 5 Serial echocardiographic studies in pediatric patients who had undergone the Ross procedure show an average increase in sinus and STJ z-score of 0.14 ± 0.25/year and 0.17 ± 0.34/year, respectively. 3 Histologically, the root wall media shows intralamellar components showing varying degrees of disorganization. This maladaptation has also been demonstrated at the proteomic level by Chiarini and coworkers, who found differences in expression levels of Paxillin, Vimentin, Jagged-1 fragment, and Notch1 intracellular domain fragment between control aortic tissue and human autograft tissue excised 8 to 16 years after the Ross procedure. 6 Chronically, valve leaflets show thickening due mainly to the addition of a layer of “neointima” consisting of radial elastic fibers, collagen bundles, and glycosaminoglycans on the ventricular aspect of the leaflet.7,8
Bryan and coworkers used an ingenious “left heart simulator” which they have employed in multiple other studies. 9 The principal changes they observed in the autograft group with simulation were twofold. (1) The closing velocity of the noncoronary leaflet was increased compared to that of the native aortic valve group. This finding may be related to the difference in compliance between the coronary and noncoronary sinuses due to the implanted coronary buttons. Although the clinical implications are unclear, this finding could be further studied using a computational model. (2) After explantation, the autograft leaflets were observed to be thinner by 39% and Young's (or elastic) modulus decreased by 70% compared to those of a separate pulmonary valve group not subjected to left heart simulation. While reversible stretching and thinning might be expected, the intriguing result was that the altered leaflet characteristics persisted after removing the stress. In the language of solid mechanics, the leaflet was plastically deformed, implying an acute intrinsic structural change in the leaflets, in turn accounting for the observed change in Young's modulus. In short, it is an acute injury. If true, then maladaptive healing might partially explain later autograft valve failure especially in the absence of root dilation.
This finding should be looked at with some caution, however. The investigators also measured a 47% decrease in Young's modulus of native aortic valve leaflet tissue. Why should aortic valve leaflets suddenly change their intrinsic structure in the simulator, when they are already accustomed to the systemic pressure of 6 to 9-month-old piglets (about 100 mm Hg)? Perhaps, as the authors point out, the changes were due to the use of a crystalloid perfusate and xenografts that were nonviable for up to 24 h. There was also considerable variance in the measurements, suggesting the need for careful consideration of possible measurement error (especially with the bulge tests) and consideration of a modified study design (including measurement technique) in which (at least for some measurements) grafts could serve as their own control.
The authors also noted the absence of significant root dilation in the simulated autografts. They explain this by suggesting that the coronary buttons added stiffness to the root. In clinical studies, however, root dilation has been observed within 1 week of autograft implantation. 10 Propensity to early dilation likely depends on the relative size and location of the coronary buttons, the absolute initial diameter of the root and the presence of vasculopathy. The clinical relevance is unclear but could be studied by comparing the rate of chronic changes in patients with and without “early” dilation.
The currently favored approach to reducing the incidence of autograft root dilation and some cases of valve failure is to externally “support” the autograft with synthetic material of limited compliance. The technique was described in 2005. 11 In 2013, Brown and coworkers published their series of Ross patients (mean age 16 years) in the World Journal. 12 Fifty-one patients underwent a “supported” Ross consisting of reinforcing the aortic valve annulus and STJ and replacing the ascending aortic if it was dilated. At a mean follow up of approximately 4 to 5 years, 94% of the 51 patients had not required surgical reintervention on their autografts. In 2016, Carrel and Kadner reported a small series (22 adults, 10 of whom had BAV) of patients who underwent a Ross in which the autograft was supported with a Dacron graft. 13 One patient required early valve replacement. At mean follow up of 5.8 years (range 1.2-9 years) freedom from more than trivial neo-AI was 75% and no cases of autograft dilation were observed. In 2019, Riggs and coworkers reported excellent results with a modification in which the autograft is implanted within a sinus of Valsalva graft, then the composite is implanted into the left ventricular outflow tract. 5 Among 40 patients with median age 16 years (range 10-35 years) undergoing this procedure, the prevalence of more than a mild degree of valvar regurgitation was 2.5% (1 patient) at a median follow up of 3.5 years. Four patients (10.0%) had an aortic sinus z-score >2.5 but no patient had z-score >4. No patient had required reintervention on the valve or root.
Despite these encouraging results, many concerns related to this approach remain unresolved. These include the following:
The follow up in these series is relatively short (median 3-6 years). In the world of valve prostheses, the supported Ross would still be considered a new valve, yet to undergo the “acid test” of comparing it with many prosthetic options over 10, 20 even 30 years of follow up. The supported Ross is not an option for patients less than 10 to 12 years old, and generally not recommended for pulmonary annulus diameters less than 24 mm.
5
External support with a contiguous, zero compliance graft reduces the strain on the autograft, but not the stress. The dominant “normal” stress is systemic pressure on the luminal side, with an equal and opposite stress exerted by the prosthetic support on the autograft from the adventitial side. The compressive stress may result in a chronic “maladaptive” cellular response. The root may take on the identity of its external support, with zero compliance. This produces a ventriculo-arterial impedance mismatch. Over 20,30,40 years, one must be concerned about long-term ventricular function as a result.
14
External support does not resolve the potential problem of primary leaflet failure due to chronic increased leaflet stresses, despite the use of the Valsalva graft. It remains to be seen whether the autograft valve functions better over time than our best current—and future—prostheses.
The authors of the present study acknowledge that a 30 min simulation will unlikely uncover the mechanisms by which some autografts gradually undergo root dilation or valve failure. A much longer duration of simulation would be fraught with overall cadaver xenograft deterioration. Since the simulations did not produce significant root dilation, evaluating methods of “supporting” the root also would unlikely yield useful information.
Perhaps it is time to work “out of the box” to develop alternatives to the noncompliant synthetic graft. For example, focusing on the problem of root dilation, Francesco Nappi and his collaborators at the Cardiac Surgery Centre Cardiologique du Nord de Saint-Denis in Paris have spent the better part of the last decade developing a composite “semi-absorbable armoured” external support prosthesis.15–17 This composite graft consists of an inner layer of biodegradable polydioxanone (PDS) mesh and an outer “armour” of specifically fashioned e-polytetrafluoroethylene (PTFE) loose wrap (Figure 1). The 2 materials work in concert, the PDS, acting as a cellular scaffold, reacting with the autograft to produce gradual “arterialization” of the wall, and the somewhat compliant PTFE controlling early tendency for root dilation during the arterialization process. The Paris group has extensively tested the graft in the descending aorta of growing lambs and has shown that the graft increases in size in concert with overall somatic growth from 20 to 60 kg. Their series of papers is a remarkable display of combining bioengineering (computational) modeling, detailed tissue engineering, and a large animal model. There appears to be plenty of space for other investigators to verify this group's results, expand the development of this or other novel models, and incorporate bioengineered modifications to the leaflets to insure longevity of valve function itself. Perhaps there could be a role for the “left heart simulator” in these complex but potentially impactful studies.
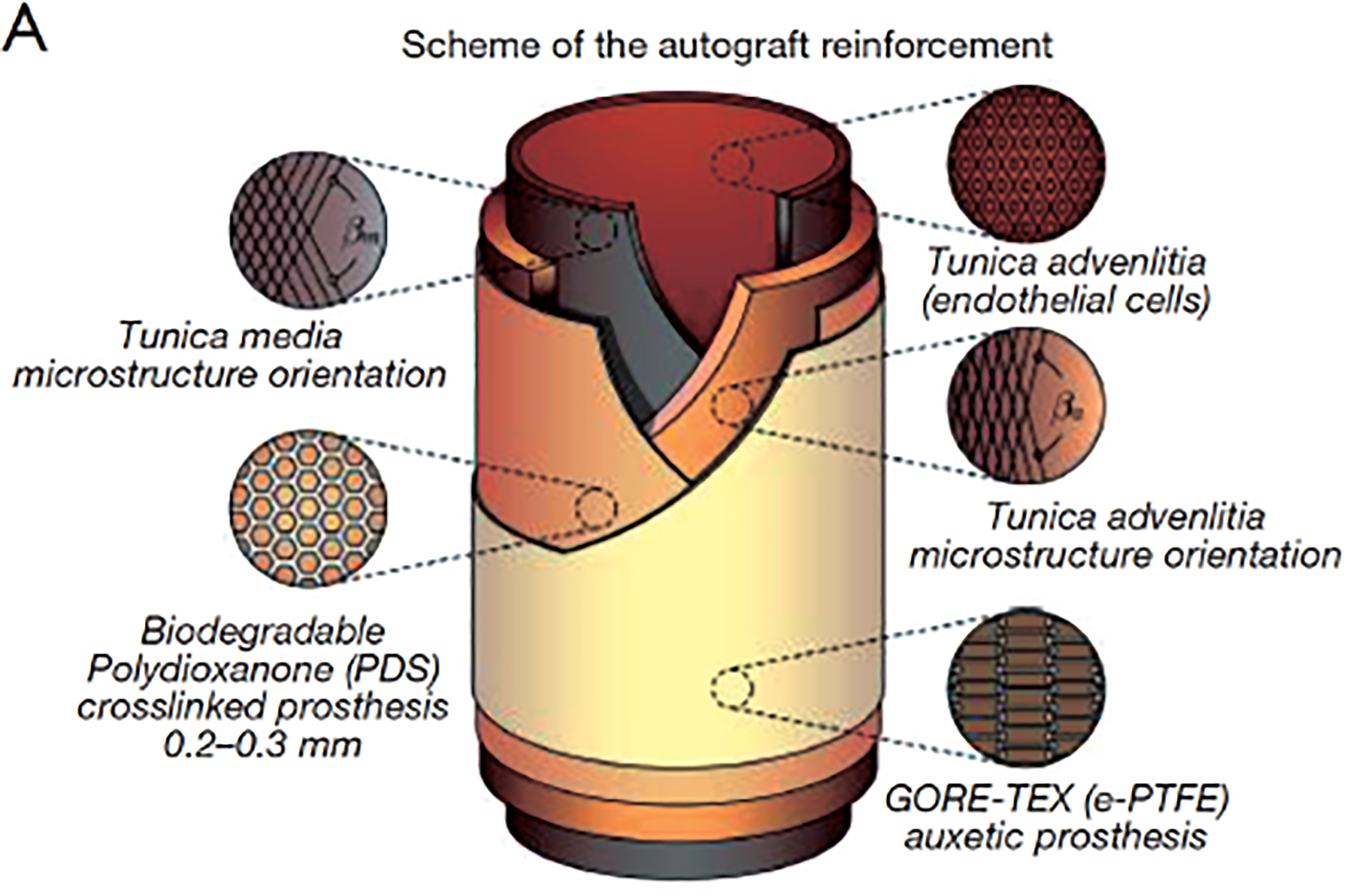
Modified composite Ross graft consisting of an inner layer of biodegradable cross-linked polydioxanone, and an outer layer of e-PTFE auxetic prosthesis. From Nappi et al, 14 used with permission of the publisher.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.