
Abstract
Background
Institutional survival following Norwood procedures is traditionally correlated with a center's surgical volume. Multiple single and multi-institutional studies conducted at large-volume centers have recently demonstrated improved survival following Norwood procedures. We report both short- and long-term outcomes at a single, small-volume institution and comment on factors potentially influencing outcomes at this institution.
Methods
All patients undergoing Norwood procedures from January 1, 2005, to January 1, 2020, at our institution were included in this study. Kaplan-Meier survival and Cox regression risk factor analyses were performed in addition to first interstage risk factor scoring to compare observed versus expected survival.
Results
The cohort included 113 patients. Kaplan-Meier freedom from death or transplant was 88%, 80%, and 76% at 1, 5, and 10 years, respectively. Freedom from death following hospital discharge after Norwood procedures was 94%, 87%, and 83% at 1, 5, and 10 years, respectively. The presence of genetic syndromes was a significant risk factor for mortality. First interstage observed-to-expected mortality following discharge was 0.57 (P = .04). Postoperative length of stay was comparable to that reported for the period 2015 to 2018 in the Society of Thoracic Surgeons Database.
Conclusions
Survival outcomes at this single, small-volume institution were similar to those reported by large-volume centers and multi-institutional collaborative studies. These results may be related to structural and functional features that have been demonstrated to influence outcomes in other studies. These factors are achievable by small-volume programs with sufficient resource allocation.
Keywords
Introduction
HLHS and other similar conditions consisting of single ventricular physiology with ductal dependence are fatal if interventions are not performed in the neonatal or early infancy period.1,2 The Norwood procedure and its variants constitute the first of three operations currently used to manage these patients.2,3
Mortality following Norwood procedures remains significant. The 2019 STS Congenital Database cites a 14.4% perioperative mortality rate. 4 Previous studies have shown that survival rates vary considerably among institutions and may be associated with the number of Norwood procedures performed at the center.5,6 Although large-volume individual centers and multi-institutional collaborations have published analyses of their Norwood experiences, experiences of individual smaller volume centers are not often published.
We present the cumulative experience of managing patients requiring Norwood procedures at one smaller volume center. We present results for risk-adjusted perioperative, interstage, and cumulative survival, and compare actual outcomes to “expected” outcomes based on STS perioperative and NPCQIC interstage survival scoring methods.4,7 Additionally, we describe structural and functional features employed at this center to manage these patients.
Patients and Methods
The Orlando Health Institutional Review Board approved this retrospective chart review. Patient consent was waived. We extracted preoperative risk factors, operative data, perioperative complications, survival status, LOS, and postoperative LOS from medical records of all patients (N = 113) undergoing Norwood or Hybrid Stage 1 (hereafter referred to as Hybrid Norwood) procedures between January 1, 2005, and January 1, 2020. We determined survival status as of January 1, 2020, using medical records for 100 patients. We determined statuses for 13 patients using the Center of Disease Control's National Death Index. We defined survival as transplant-free survival and survival time as the time from the date of the Norwood (“time zero”) to January 1, 2020, or the date of death if earlier. “Mortality” in the context of this study refers to death or transplantation. We used IBM SPSS 26.0 (IBM) for analysis.
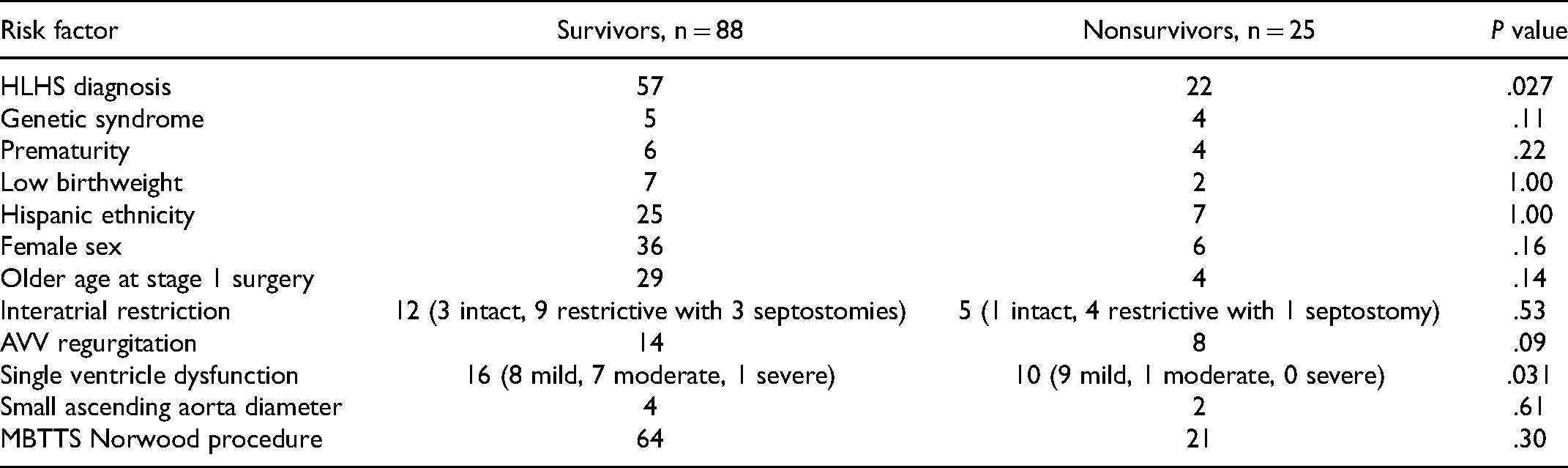
Preoperative Risk Factors
For risk-adjusted modeling, we examined previously studied factors for Norwood mortality including prematurity, low birthweight, Hispanic ethnicity, female sex, older age at the time of operation, genetically related syndromes, HLHS diagnosis, significant neonatal AVV regurgitation, highly restrictive interatrial communication, reduced single ventricular function, small ascending aorta diameter, surgeon performing the operation, and type of Norwood.8–17 Genetic syndromes included DiGeorge's, Down's, Turner's, Partial Trisomy 7, Distal 10q Deletion, and 18q Deletion. We defined premature birth as birth before 37 gestational weeks and low birthweight as <2,500 grams. We defined older age at the time of operation as >7 days old. We defined highly restrictive interatrial communication as trans-atrial pressure gradients >8 mm Hg by echocardiogram, intact septum, or need for preoperative atrial septostomy (intact septum, restriction, and septostomy data were documented). We defined significant AVV regurgitation as “moderate” or “severe” using echocardiogram reports. We defined reduced preoperative single ventricular function as “depressed” or “decreased” using echocardiogram reports and the degree of dysfunction was documented. We defined small ascending aorta diameter as ≤1.5 mm. We defined MBTTS Norwood procedure as a risk factor. All preoperative echocardiogram data were obtained from the most recent echocardiogram preceding the Norwood.
Surgical Procedures
We generally followed conventional technique for Norwood procedures with some variation over the 15-year period. The key steps included: (1) cardiopulmonary bypass with core cooling to 18 °C (22-25 °C later in the series), (2) atrial septectomy during a brief period of circulatory arrest, (3) selective cerebral perfusion with flow rate of 40 to 60 cc/kg/min during arch reconstruction, (4) proximal aortopulmonay amalgamation (Damus connection) and arch reconstruction with homograft patch material (with excision of the periductal segment of isthmus if a prominent ductal shelf is present), (5) placement of a 3.5 to 4.0 mm PTFE shunt from the innominate artery to right pulmonary artery, or for selected cases from 2013 to 2020, a 6 mm ringed PTFE “Sano” graft from the systemic ventricle free wall to the pulmonary artery bifurcation, performed during reperfusion and rewarming. Hybrid Stage 1 Norwood procedures were performed in our hybrid catheterization lab, consisting of ductal stenting and placement of bilateral branch pulmonary artery bands using PTFE, with balloon atrial septostomy as necessary. Two surgeons performed all Norwood procedures in this study.
Interstage Mortality Risk
We defined interstage mortality as all-cause mortality occurring between the discharge date following the Stage 1 Norwood and the bidirectional Glenn date. We compared observed mortality to expected mortality predicted by “NEONATE” scoring given the set of patient-specific risk factors. 7 The NPCQIC's “NEONATE” interstage risk scoring model predicts freedom from first interstage death using eight predischarge risk factors that include MBTTS Norwood selection, Hybrid Norwood selection, postoperative ECMO use, opiates prescribed at discharge, no digoxin prescribed at discharge, postoperative arch obstruction, moderate or greater tricuspid regurgitation without oxygen requirements at discharge, and moderate or greater tricuspid regurgitation with oxygen requirements at discharge. 7 We obtained the “NEONATE” regression model by permission and acquired the necessary data for 99 of 104 discharged survivors.
Statistical Analysis
We expressed cohort continuous descriptive variables using computed means and medians. We used Kaplan-Meier analysis to determine freedom from death following the Norwood in addition to freedom from death contingent on survival to discharge. We applied univariable Cox survival regression modeling to screen for significant preoperative risk factors using a cut-off P value <.20. We entered significant factors into a multivariable Cox regression to determine risk-adjusted survival, hazards ratios, and confidence intervals with final risk factors identified by P value <.05. We generated Cox regression survival curves showing survival in the presence or absence of each significant final risk factor, holding other risk factors constant at the average value for the cohort. Patient characteristics, “NEONATE” risk factors, preoperative risk factors, operative data, perioperative data, and perioperative complications were compared between survivors and nonsurvivors using two-tailed Fisher exact testing for binary variables and two-tailed unpaired t testing for continuous data with P value <.05 indicating significance.
We calculated expected interstage mortality using the logistic regression equations used to derive “NEONATE” risk scoring. Each patient's binary risk factor values (xi) were entered into the following equation to calculate each patient's individualized probability of an interstage event (Ej):
Results
Cohort Characteristics
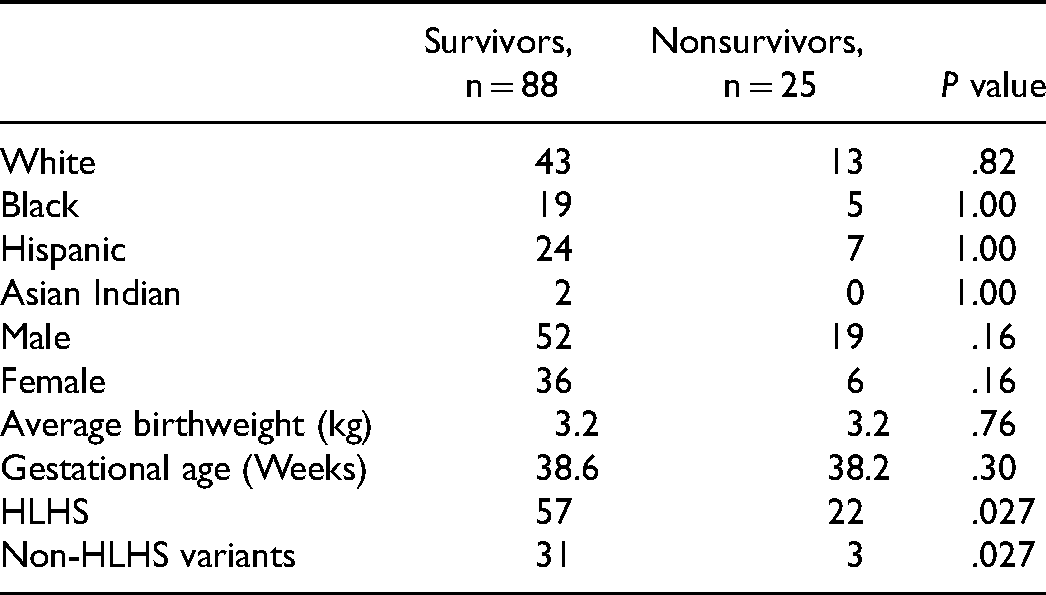
Characteristics of this cohort (N = 113) are shown in Table 1. Seventy-nine of the 113 patients were diagnosed with HLHS. Diagnoses for the remaining 34 patients included truncus arteriosus (1), critical left ventricular outlet obstruction with aortic arch interruption or hypoplasia (5), severe congenital mitral stenosis (2), single ventricle with heterotaxy (2), double inlet left ventricle (14), unbalanced atrioventricular canal (2), mitral atresia (2), tricuspid atresia (4), and double outlet right ventricle (2). Table 2 shows the distribution of preoperative risk factors.
Norwood Patient Characteristics.
Preoperative Risk Factor Distribution.
Operative and Perioperative Data
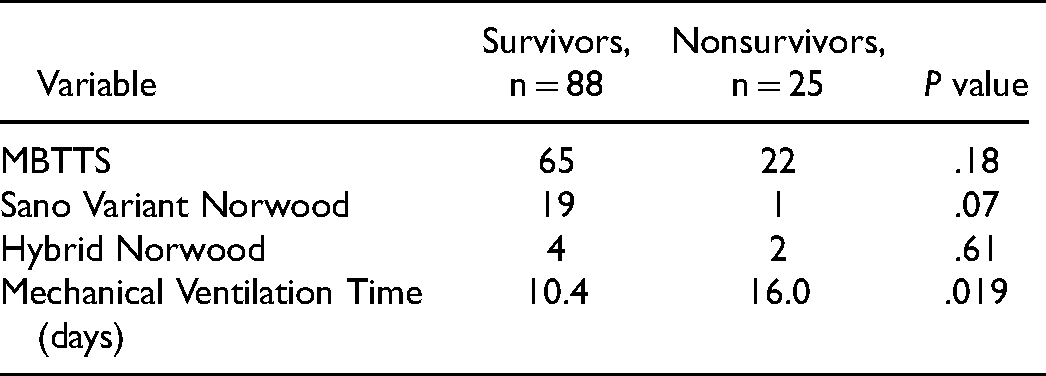
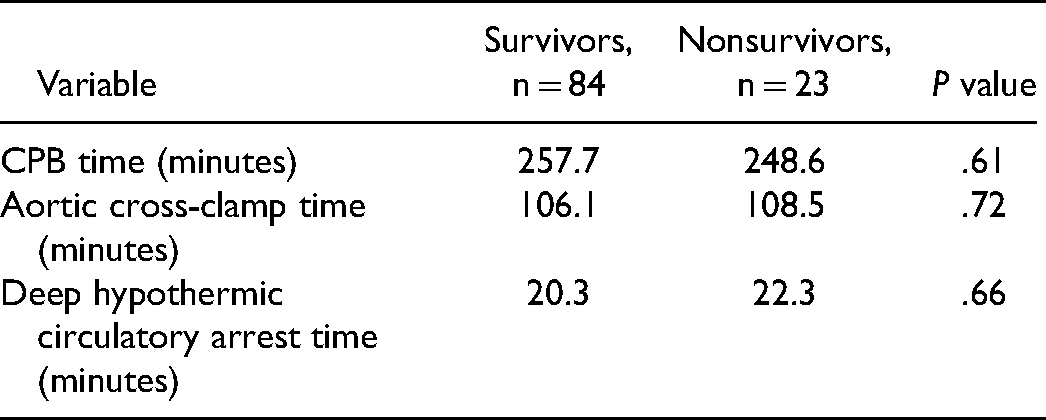
Table 3A shows perioperative and operative data for all patients. Table 3B shows operative data in patients undergoing conventional Norwood procedures.
Operative and Perioperative Data for All Patients.
Operative Data for Patients Undergoing Conventional Norwood Procedures.
Unadjusted Survival
As of January 1, 2020, 88 (77.8%) patients were living transplant-free with a median follow-up of 6.1 [5.3, 6.9] years. One patient underwent transplantation. 104 patients (92.0%) survived to discharge after the Norwood with 101 patients (89.4%) surviving to the Glenn procedure. Kaplan-Meier survival was 88%, 80%, and 76% at 1, 5, and 10 years, respectively (Figure 1). Kaplan-Meier survival contingent on survival to Norwood hospital discharge was 94%, 87%, and 83% at 1, 5, and 10 years, respectively (Figure 2). In patients surviving to the Glenn, there was one perioperative death after a comprehensive hybrid stage II operation and no early Fontan deaths.
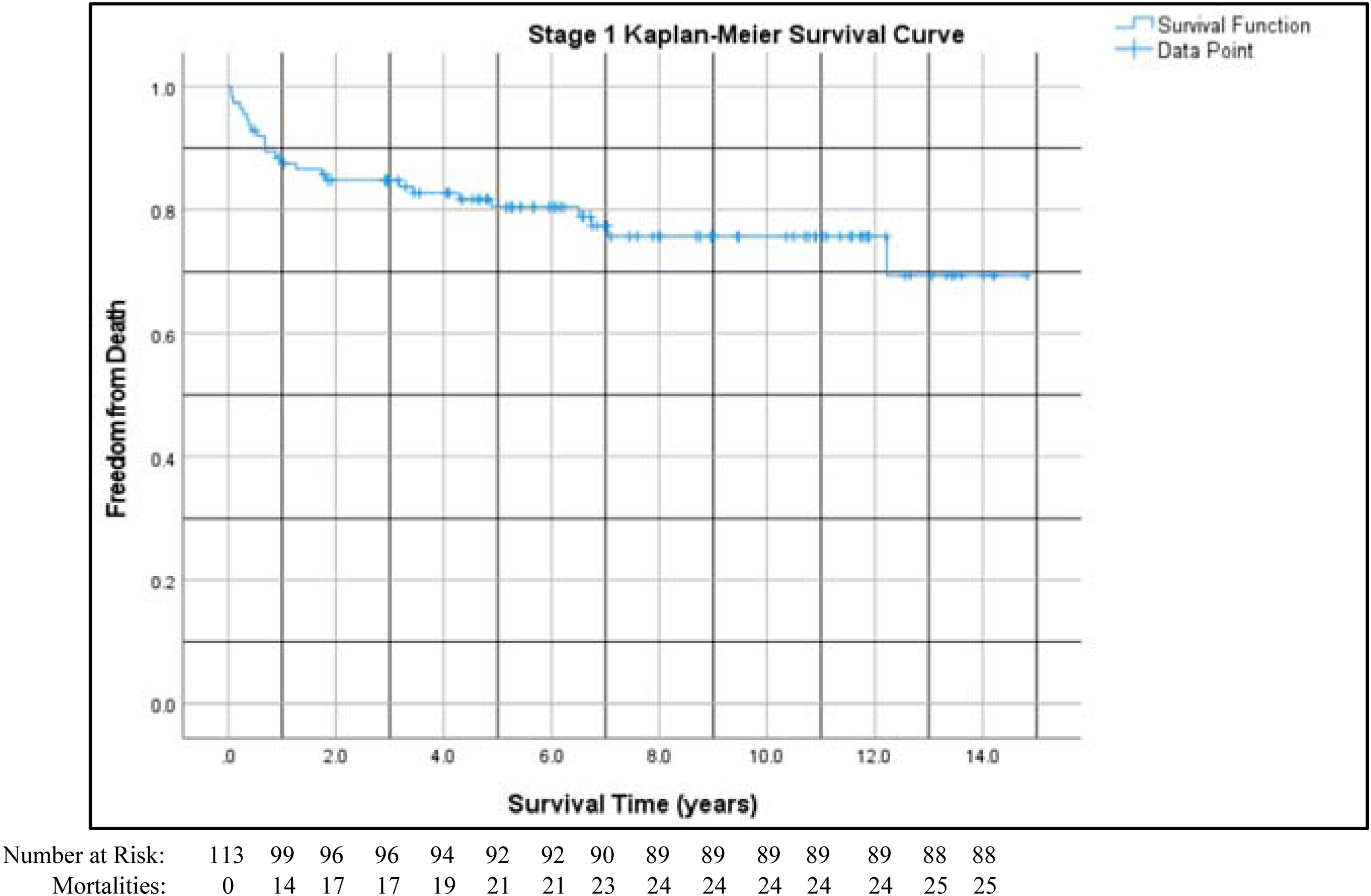
Kaplan-Meier survival in patients undergoing Norwood procedures (n = 113). “Time zero” is the day of the Norwood procedure.
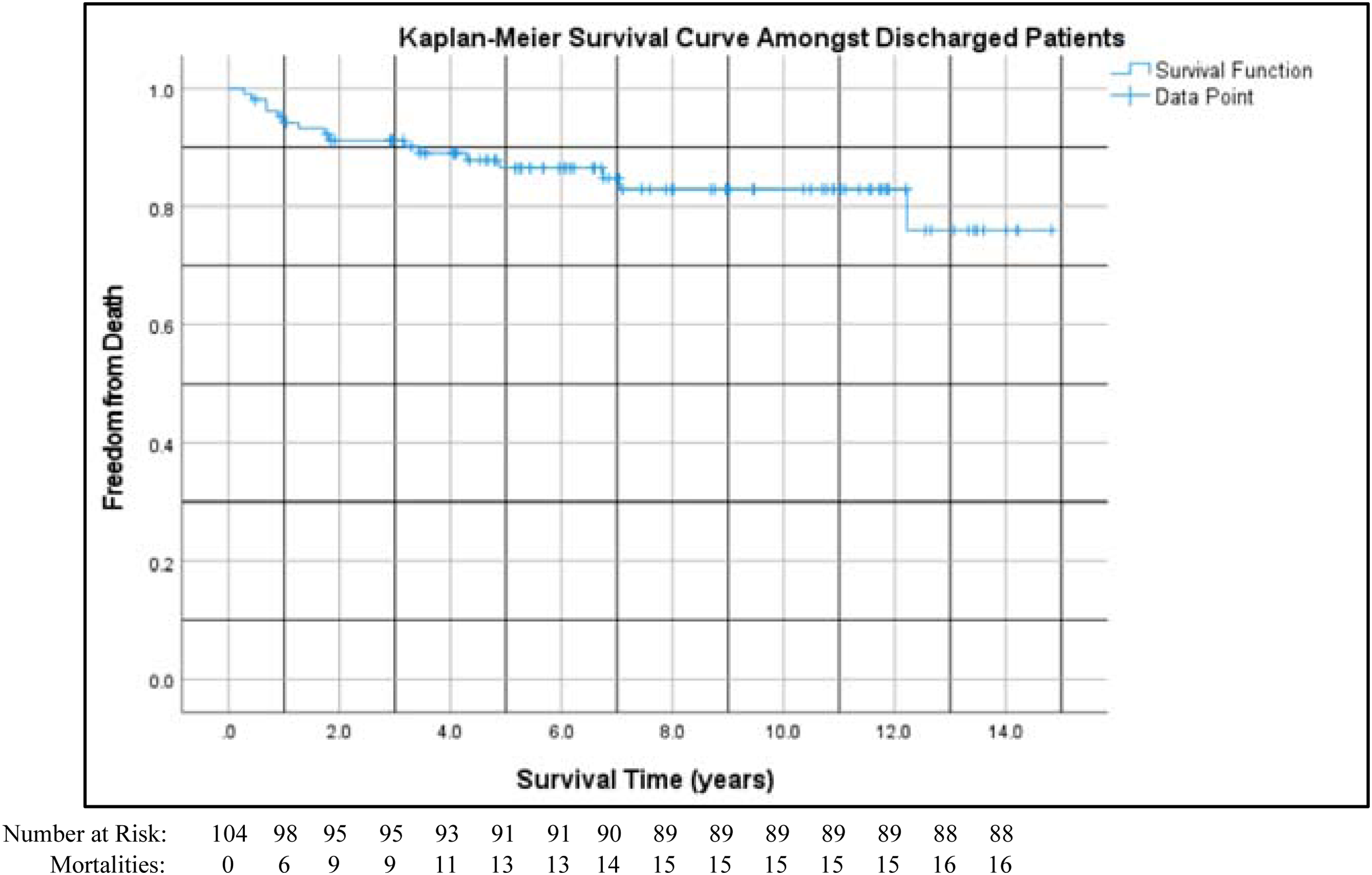
Kaplan-Meier survival in patients undergoing Norwood procedures (n = 104) who survived to the time of discharge. “Time zero” is the day of the Norwood procedure.
Interstage Survival
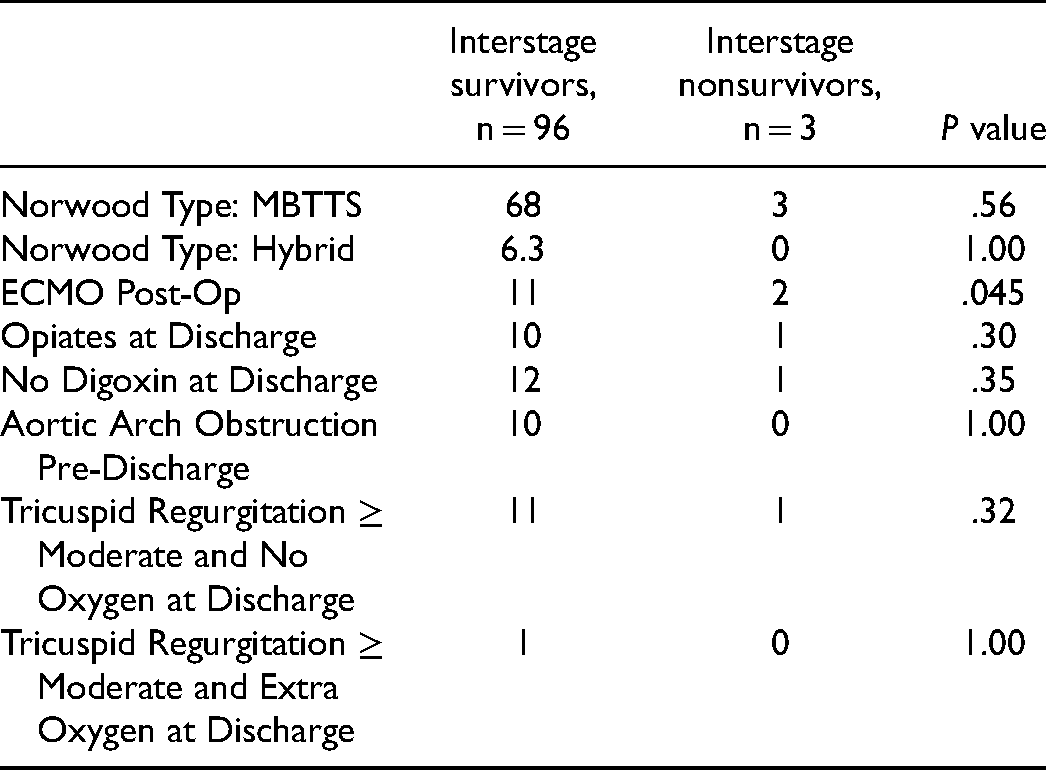
We included 99 patients in this analysis. There were three interstage deaths. Table 4 shows the distribution of “NEONATE” risk factors among interstage survivors and nonsurvivors. Using “NEONATE” scoring, expected deaths (E) was 5.28, yielding an O/E mortality ratio of 0.57 [0.18, 0.96], P = .04, compared to the mean of 1.0.
“NEONATE” Risk Factors Among Interstage Survivors and Nonsurvivors.
Risk-Adjusted Survival
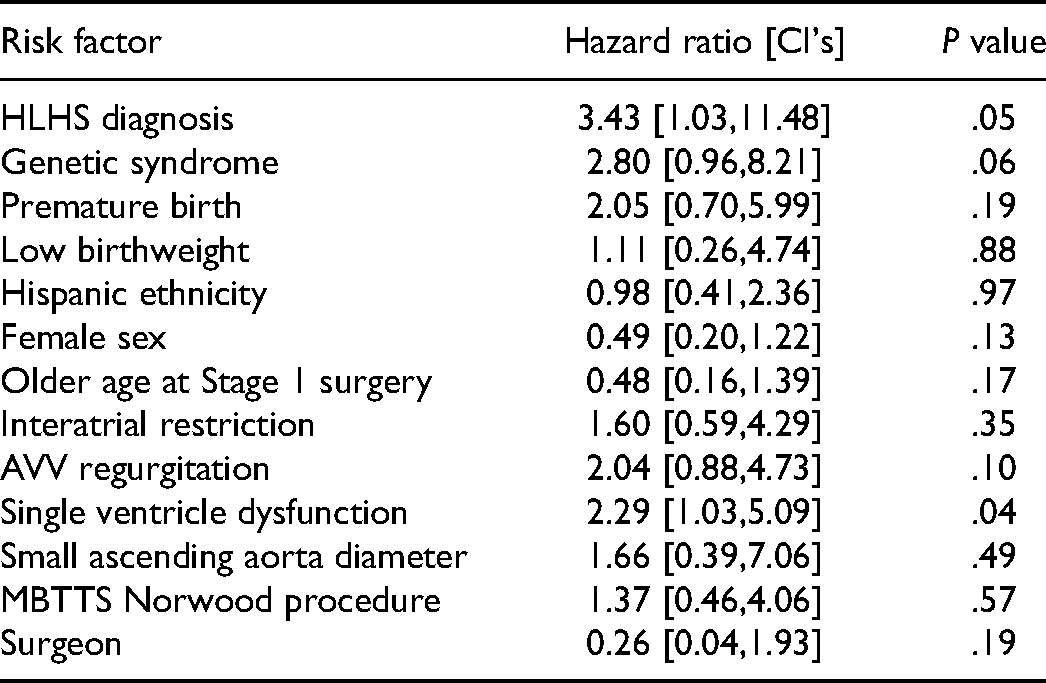
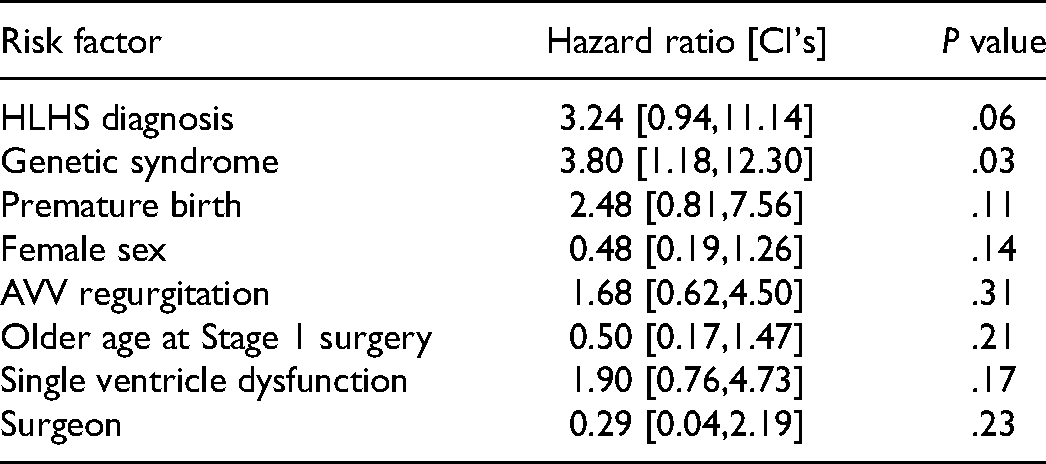
Table 5A shows hazard ratios, 95% confidence intervals and P values for univariable Cox regression models. HLHS, genetic syndromes, premature birth, female sex, older age at stage 1 surgery, AVV regurgitation, single ventricle dysfunction, and surgeon were then entered into a multivariable Cox regression and Table 5B shows the results. Genetic syndromes were the only final risk factor significantly affecting survival. Figure 3 illustrates the impact of genetic syndromes.
Univariable Cox Regression Models.
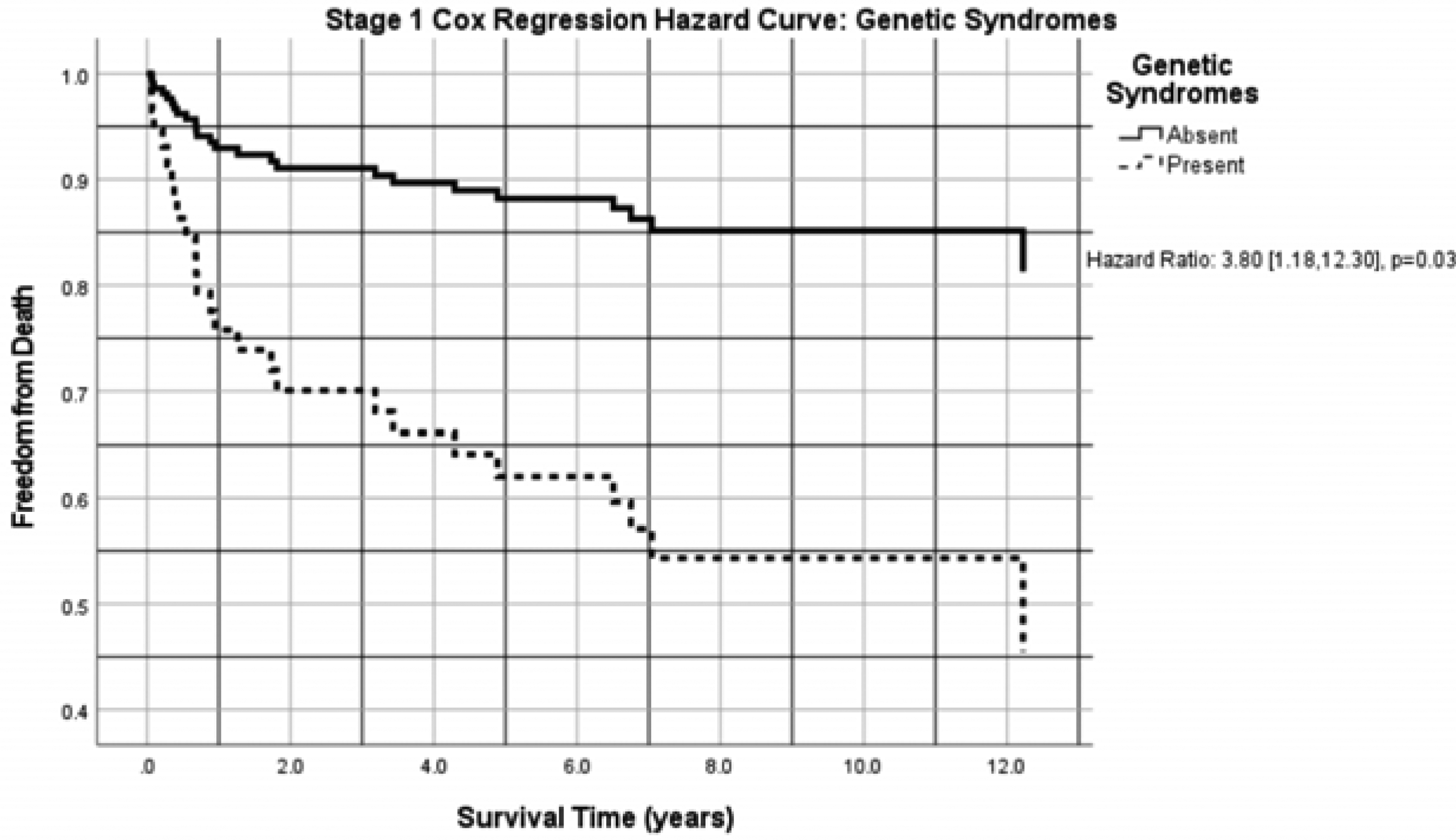
Cox regression modeling. The dotted line shows survival when genetic syndromes are present, and the solid line shows survival when they are absent.
Multivariable Cox Regression Model.
Length of Stay and Perioperative Complications
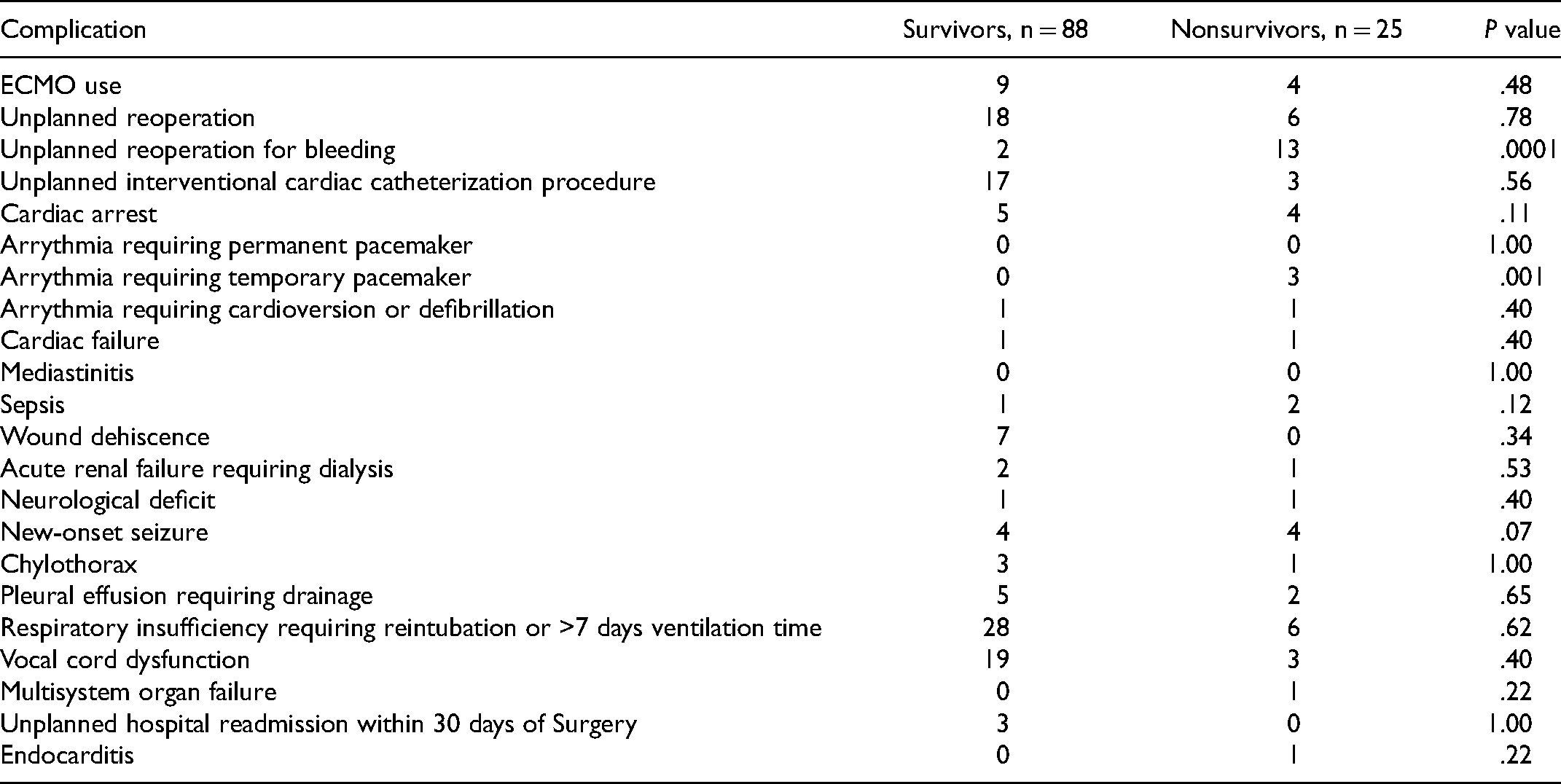
Table 6 shows LOS and postoperative LOS for discharged patients. The differences in total LOS (P = .70) and postoperative LOS (P = .55) between discharged survivors and nonsurvivors were not statistically significant. Mean postoperative LOS (50.9 days) was slightly less, and median postoperative LOS (43.5 days) was slightly greater than that reported for the period 2015 to 2018 by the STS Congenital Database (53 days and 35 days, respectively). 4 Table 7 compares perioperative complications between survivors and nonsurvivors.
LOS and Postoperative LOS for Patients Surviving to Hospital Discharge.

Perioperative Complications.
Comment
Single ventricle patients with ductal dependence comprise a challenging cohort in pediatric cardiac surgery. Mortality remains significant and resource requirements are considerable. Because these anomalies are not rare, most pediatric cardiac centers in the United States manage these cohorts. The variability in outcomes, however, is considerable and many believe that these outcomes can serve as an indicator of program performance.
In our cohort, Kaplan-Meier survival was 88%, 81%, and 76% at 1, 5, and 10 years, respectively. For comparison, a recent single, large-volume institutional study examined Norwood outcomes with 76% of patients living transplant-free at one year and another more recent single, large-volume institutional study demonstrated 1-, 5-, and 10-year survival to be 86%, 81%, and 77%, respectively.18,19 Another study of neonates at a large-volume institution found that survival to discharge in this demographic was 84.3% from 2009 to 2014. 20 Multi-institutional studies have demonstrated similar results. For example, the SVR 2.0 trial showed that 73% of 549 neonates undergoing Norwood procedures survived to the Glenn operation. 21 Moreover, another recent multi-institutional study of more than 500 cases found 1- and 5-year survivals of 69% and 61%, respectively. 22
This center performed 113 Norwood procedures over 15 years (7.5 Norwood operations and a total of 145 cardiac surgical procedures per year on average), qualifying it by some as a lower volume program.23,24 The positive association between volume and Norwood outcomes has been demonstrated in several studies.5,6,23,24 However, our analysis shows anecdotally that lower volume programs can ideally achieve Norwood survival outcomes similar to those of large-volume centers.
Overall, this center's risk-adjusted ratio of observed-to-expected operative deaths for STAT 5 cases using STS Congenital Database data for 2015 to 2018 was 0.58 [0.12, 1.56].
25
Additionally, this center's “NEONATE” O/E mortality ratio was 0.57 [0.18, 0.96].
7
Although only the “NEONATE” ratio was statistically significant, these results provide evidence that a small-volume institution can achieve favorable results compared to the collection of centers performing Norwood procedures. To put our Norwood results over 15 years in context of our overall program performance, we performed 2,170 pediatric cardiac surgical procedures with 42 total operative deaths (621 STAT 1 procedures with one operative death, 869 STAT 2 procedures with six operative deaths, 217 STAT 3 procedures with six operative deaths, 340 STAT 4 procedures with 21 operative deaths, 123 STAT 5 procedures with eight operative deaths). Although we were unable to determine specific factors that led to these results, we believe the adaptation of structures and processes that have been shown to improve outcomes at other programs was contributory.
26
These features include the following:
A comprehensive fetal echocardiography program with robust link to maternal–fetal medicine specialists: ductal-dependent neonates are delivered at an adjacent women's hospital and immediately cared for in the on-site Level 3 Neonatal Intensive Care Unit. This colocation of all related maternal and neonatal services obviates the need for lengthy transfer and has been shown to improve post-Norwood survival.
27
Deliberate multidisciplinary decision-making in choosing the hybrid Norwood or traditional Norwood utilizing either MBTTS or Sano shunts: consistent with large-volume centers, our institution uses hybrid Norwood procedures for high-risk unstable, very ill, or very low birthweight neonates (<2.0 kg).
28
Additionally, we use Sano shunts in neonates with aortic atresia, very small ascending aortas, or arch branching anomalies as this demographic has been shown to benefit from Sano shunts.
28
Selective perioperative ECMO use after the Norwood: 13 patients required ECMO after the Norwood and nine of them survived to discharge. ECMO utilization has been shown to improve survival outcomes in these patients.
29
A pediatric cardiac perfusionist is always at the patient's bedside during ECMO support. A 24-7 hybrid catheterization lab and interventional team with full inhouse surgical team coverage: 20 patients in our series required unplanned interventional cardiac catheter lab procedures perioperatively. Studies have shown its importance in the staged surgical management of HLHS patients.
30
Moreover, the cardiac operation room and its staff are dedicated to the Heart Center at all times without consideration for block time or shared resources with other surgical services. Dedicated pediatric cardiac anesthesiologists (with no noncardiac-related anesthetic responsibilities) who manage all cardiac procedures and post-Norwood patients undergoing additional cardiac surgical, interventional, and noncardiac surgical procedures in the future: the importance of this level of care has been especially demonstrated for these patients.
31
A protocol-driven management system of single ventricle and shunt-dependent infants using standardized hand-off checklists and clinical protocols derived from national studies or quality initiatives including the NPCQIC and SVR trial
32
A devoted and physically independent 18-bed CICU facility with 24-7 in-house coverage by dedicated cardiac critical care physicians from admission to discharge: we adhere to the “Adaptive Care Model” promoted by the Lurie Children's Hospital program to enhance patient safety in addition to patient and family comfort.
33
Highly skilled CICU nurses trained in a six-month course (“CardioKids”) that provides multidisciplinary instruction on pediatric CICU management: our average daily CICU census is between 8 and 10, and CICU nursing staff can “flex down” by floating to other areas of the hospital as needed. In-hospital care is carried through until patients achieve full enteral feeding either orally or via G-tube, which has been shown to improve interstage weight gain: our center conducts early postoperative VCD evaluation in all patients undergoing aortic arch repairs to help identify patients needing G-tubes.
34
Prompt VCD evaluation and G-tube placement have been shown to neutralize excess LOS due to VCD.
35
An interstage home surveillance program since 2010, which has been shown to improve first interstage survival
36
The use of digoxin during the first interstage period since 2005: this has been shown to improve interstage survival and is recommended by the NPCQIC.
37
Although associations between Norwood volume and survival outcomes have been established, a recent study analytically demonstrated that confounding variables may affect this association casting doubt on a causal relationship.
24
Moreover, a recent study analyzed STAT Category-specific O/E mortality ratios using data from multiple institutions of varying volumes.
38
This study uniquely accounted for “hospital-level capacity and resources” as a risk factor in its analysis and showed no relationship between volume and O/E mortality ratios for any STAT category.
38
Based on this, the authors concluded that volume should not be the “sole criterion” for determining the viability of congenital cardiac surgical programs.
38
In other words, volume may not independently predict better outcomes. Surgical volume is likely a surrogate for other factors, such as the listed programmatic processes and structures, which underpin good Norwood outcomes. Thus, smaller volume Norwood programs can have survival outcomes similar to large-volume centers as demonstrated in this report. It is encouraging that organizations like the Congenital Heart Surgeons Society are currently discussing quality improvement projects in which structures and processes of “underperforming” programs are examined, and changes are suggested by expert advisory teams.
Our report has important limitations. Although we listed other outcomes like perioperative complications, our primary analyzed outcome measure was survival. Although mortality is still significant in the Norwood population and remains a good metric of a program's Norwood performance, long-term outcomes including neurodevelopmental and functional health status are also important and should be further studied. Further, we did not rigorously establish the association between the structural features of our program and our program's survival outcomes. A single institutional study to achieve this would be difficult to execute. Finally, we compared this center's Norwood results to studies that were not necessarily matched by era or risk factors as the raw data from these studies were not available.
In conclusion, this paper reports survival outcomes of patients undergoing Norwood procedures at a single, lower volume center. Outcomes at this center were similar to those reported by other single institutional studies at large volume centers and multi-institutional collaboratives that included high volume institutions. Thus, this study anecdotally demonstrates that lower volume programs ideally can achieve the intermediate-term Norwood survival outcomes of high-volume programs. Perhaps other lower volume programs could achieve similar results by addressing structural and functional features in which there is evidence of their salutary effect on program performance and survival outcomes.
Footnotes
Abbreviations
Acknowledgments
This study was supported with a grant from the Orlando Health Foundation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.